

What’s a stronger regimen of furosemide, 40 daily or 20 bid?
I ask this question often on rounds. The answer: it depends.
Understanding what it depends ON is really helpful for dosing decisions.
Let’s explore. #tweetorial 1/
I ask this question often on rounds. The answer: it depends.
Understanding what it depends ON is really helpful for dosing decisions.
Let’s explore. #tweetorial 1/
It’s helpful to think of therapeutic effect as “episodes of diuresis” adding up to total diuresis.
A single “good” dose of a loop will result in excretion of about 250mEq (~6g) of Na in about 2-3L of urine.
For furosemide, this occurs over ~6 hours.
tinyurl.com 2/
A single “good” dose of a loop will result in excretion of about 250mEq (~6g) of Na in about 2-3L of urine.
For furosemide, this occurs over ~6 hours.
tinyurl.com 2/
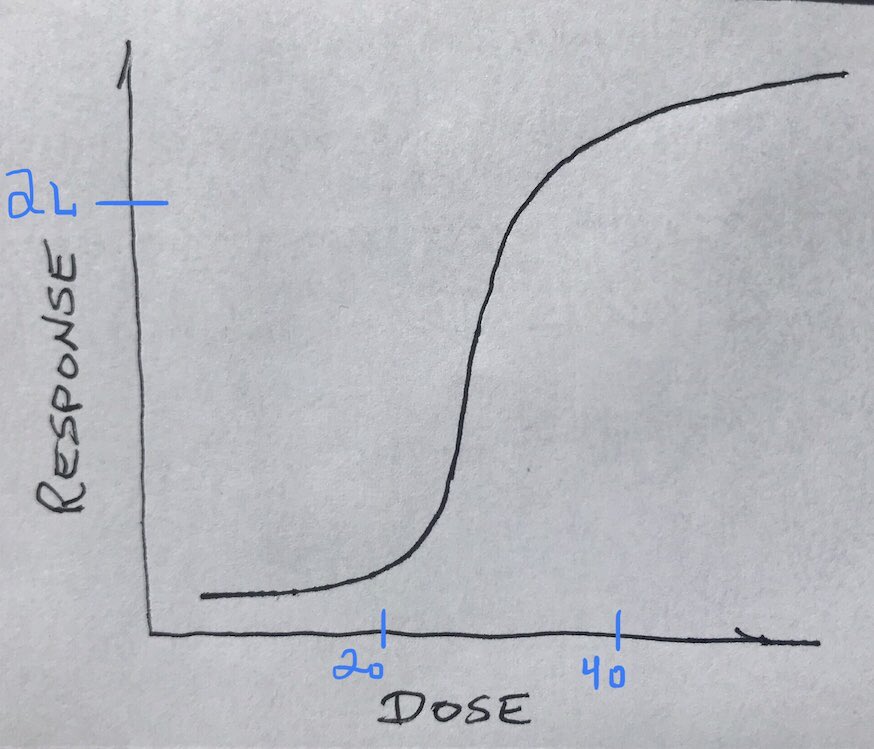
This is the dose-response curve for loop diuretics (roughly applies to each episode / dose).
The sigmoidal shape, similar to hgb-dissociation curve, means:
- at doses left of the steep part, nothing happens
- once you get past steep part, increasing dose more doesn’t do much
3/
The sigmoidal shape, similar to hgb-dissociation curve, means:
- at doses left of the steep part, nothing happens
- once you get past steep part, increasing dose more doesn’t do much
3/

These are called the threshold effect and ceiling effect, and the variable answer to the original question is all about these phenomena.
The “depends” is “depends on what the threshold dose is in this particular patient.” 4/
The “depends” is “depends on what the threshold dose is in this particular patient.” 4/

If threshold in this patient is <20, then:
40 daily: 2.5L once = 2.5L total
20 bid: 2L twice = 4L total
20 bid is stronger. 5/
40 daily: 2.5L once = 2.5L total
20 bid: 2L twice = 4L total
20 bid is stronger. 5/

But if threshold in this patient is >20 (but <40), then:
40 daily: 2.5L once = 2.5L total
20 bid: scant twice = scant total
40 daily is stronger. 6/
40 daily: 2.5L once = 2.5L total
20 bid: scant twice = scant total
40 daily is stronger. 6/
Let’s practice applying this:
Patient A is on 40IV bid in the hospital. Daily UOP is 1.5 liters.
How do you adjust? 7/
Patient A is on 40IV bid in the hospital. Daily UOP is 1.5 liters.
How do you adjust? 7/
40 clearly wasn’t reaching threshold (<<750 cc out per dose). Adding an additional episode of (non-)diuresis won’t help.
Better to increase dose and actually make each episode of diuresis effective. 8/
Better to increase dose and actually make each episode of diuresis effective. 8/
Patient B is on 40 IV bid, UOP is about 4000 per day. But they’re tolerating it well and have a long ways to go, and you’d like to augment diuresis further.
How do you adjust? 9/
How do you adjust? 9/
I would keep dose 40, make it tid.
Each dose is probably causing almost 2L out, and increasing dose further may have marginal effect.
Better to add a third episode of diuresis.
(Why no metolazone? If you can get away without it, do so. 10/
tinyurl.com )
Each dose is probably causing almost 2L out, and increasing dose further may have marginal effect.
Better to add a third episode of diuresis.
(Why no metolazone? If you can get away without it, do so. 10/
tinyurl.com )
Summary: picture speaks a thousand words. Be aware of and apply the threshold and ceiling effects of loop diuretic dose-response.
What determines these thresholds? How do you decide dosing before you’ve seen prior responses? Part two of this tweetorial coming later.
End/
What determines these thresholds? How do you decide dosing before you’ve seen prior responses? Part two of this tweetorial coming later.
End/

Loading suggestions...