

1/
Alright friends, let's pick up where we left off last week..
We'll start with a case:
A 60 yo man woke up with upper back pain and "wrapping sensations" around his chest.
2 hours later, he couldn't move his legs.
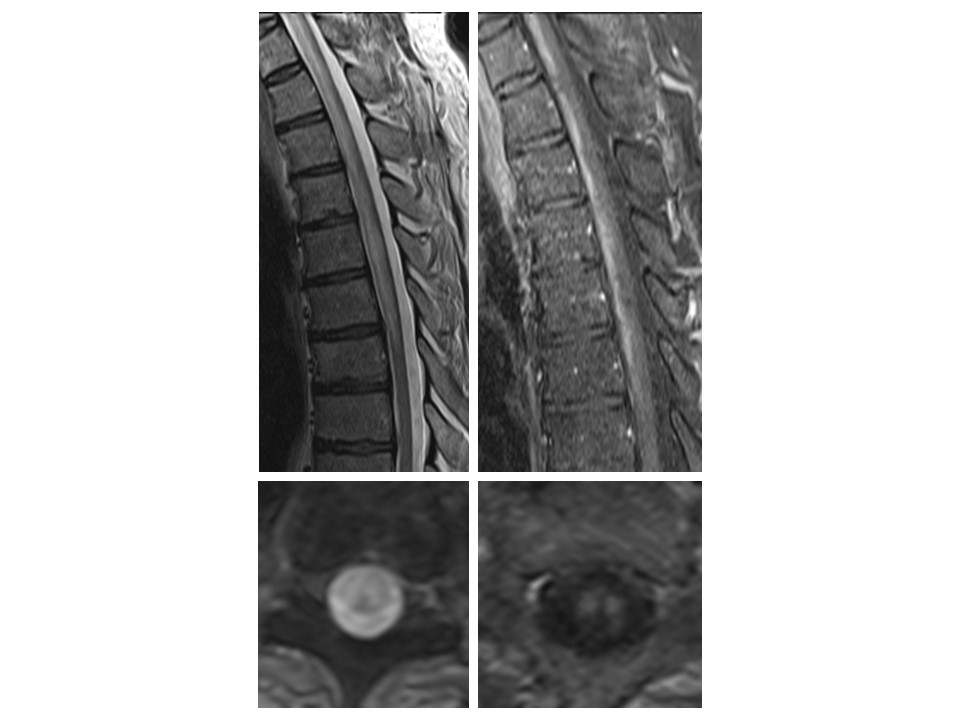
He was brought to the ED where the images below were obtained.
Alright friends, let's pick up where we left off last week..
We'll start with a case:
A 60 yo man woke up with upper back pain and "wrapping sensations" around his chest.
2 hours later, he couldn't move his legs.
He was brought to the ED where the images below were obtained.
2/
Physical examination was notable for:
▶️ BP 175/106
▶️ Flaccid paraparesis
▶️ Areflexia in the lower limbs
Physical examination was notable for:
▶️ BP 175/106
▶️ Flaccid paraparesis
▶️ Areflexia in the lower limbs
3/
Lumbar puncture was performed revealing:
▶️White blood cell count 1
▶️Protein 41
▶️Glucose 88
▶️Negative oligoclonal bands
He was diagnosed with "idiopathic transverse myelitis" and treated with IV methylprednisolone x 5 days and subsequently 5 sessions of plasma exchange.
Lumbar puncture was performed revealing:
▶️White blood cell count 1
▶️Protein 41
▶️Glucose 88
▶️Negative oligoclonal bands
He was diagnosed with "idiopathic transverse myelitis" and treated with IV methylprednisolone x 5 days and subsequently 5 sessions of plasma exchange.
4/
There was no improvement in symptoms.
Why?
Where did we go wrong?
There was no improvement in symptoms.
Why?
Where did we go wrong?
5/
Let's take a step back and approach the case from the beginning.
Last week we learned the importance of clinical time course and broke time from symptom onset to nadir into 3 categories:
▶️Hyperacute (<12 hours)
▶️Acute/subacute (1-21 days)
▶️Chronic/progressive (>21 days)
Let's take a step back and approach the case from the beginning.
Last week we learned the importance of clinical time course and broke time from symptom onset to nadir into 3 categories:
▶️Hyperacute (<12 hours)
▶️Acute/subacute (1-21 days)
▶️Chronic/progressive (>21 days)

6/
In this case, our patient's symptoms progressed to maximal deficit in just a few hours.
Remember, hyperacute presentations (<12 hours) of severe myelopathy should bring vascular myelopathy etiologies (e.g. spinal cord infarction) to the top of the differential.
In this case, our patient's symptoms progressed to maximal deficit in just a few hours.
Remember, hyperacute presentations (<12 hours) of severe myelopathy should bring vascular myelopathy etiologies (e.g. spinal cord infarction) to the top of the differential.
7/
Spinal cord infarction (SCI) is an extremely underrecognized cause of acute myelopathy, as highlighted by my friend and mentor @nzalewski2 in what I consider this truly seminal piece of literature.
jamanetwork.com
Spinal cord infarction (SCI) is an extremely underrecognized cause of acute myelopathy, as highlighted by my friend and mentor @nzalewski2 in what I consider this truly seminal piece of literature.
jamanetwork.com
8/
While patient's may have typical vascular risk factors (e.g., HTN, HLD, DM2), not all do and SCI can occur at any age.
A large proportion of SCIs are also caused by aortic dissection or fibrocartilaginous embolism.
While patient's may have typical vascular risk factors (e.g., HTN, HLD, DM2), not all do and SCI can occur at any age.
A large proportion of SCIs are also caused by aortic dissection or fibrocartilaginous embolism.
9/
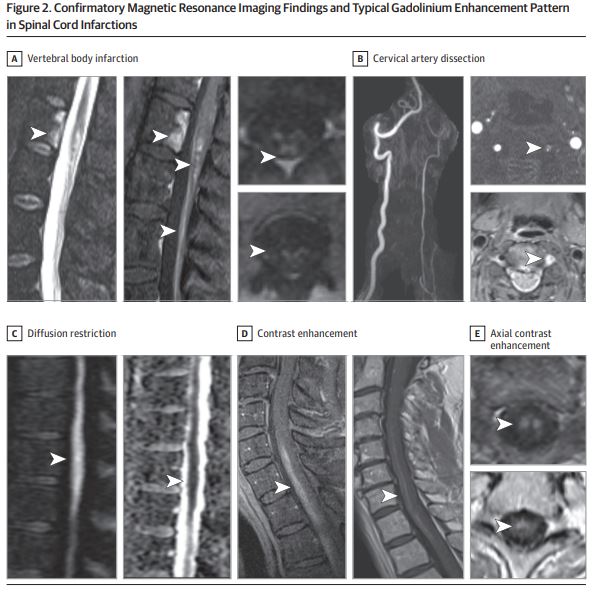
Sometimes, classic neuroimaging findings can be quite helpful:
▶️"Pencil-like" linear enhancement pattern on sagittal sequences
▶️"Owl or snake eyes" enhancement pattern on axial sequences
Referring back to Part 1 of this thread, hopefully these appear more clear now...
Sometimes, classic neuroimaging findings can be quite helpful:
▶️"Pencil-like" linear enhancement pattern on sagittal sequences
▶️"Owl or snake eyes" enhancement pattern on axial sequences
Referring back to Part 1 of this thread, hopefully these appear more clear now...
10/
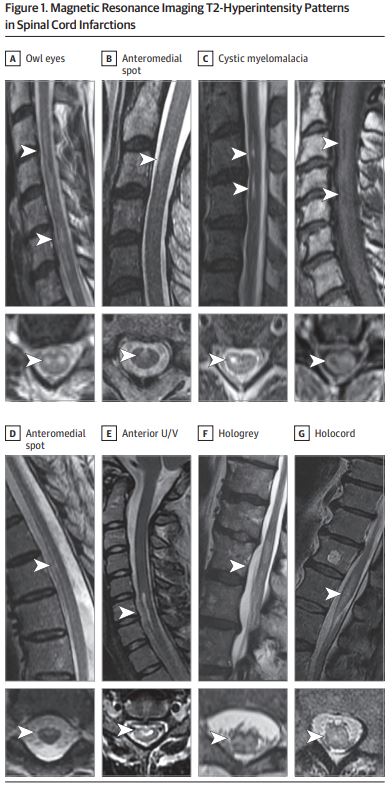
Other common T2-hyperintense patterns are highlighted well in @nzalewski2's paper as shown below.
Other common T2-hyperintense patterns are highlighted well in @nzalewski2's paper as shown below.
11/
When present, diffusion restriction and/or corresponding vertebral body infarction can be helpful to seal the diagnosis.
The sensitivity of these findings are not perfect, however, and should not exclude the diagnosis when absent.
When present, diffusion restriction and/or corresponding vertebral body infarction can be helpful to seal the diagnosis.
The sensitivity of these findings are not perfect, however, and should not exclude the diagnosis when absent.
12/
In terms of treatment, once acute spinal cord infarction is suspected consider:
▶️IV thrombolytics if within the typical window for acute ischemic stroke
and/or:
▶️Lumbar drain with blood pressure augmentation to increase spinal cord perfusion.
sciencedirect.com
In terms of treatment, once acute spinal cord infarction is suspected consider:
▶️IV thrombolytics if within the typical window for acute ischemic stroke
and/or:
▶️Lumbar drain with blood pressure augmentation to increase spinal cord perfusion.
sciencedirect.com
13/
Afterwards,
Similar to cerebral infarcts, explore potential mechanisms for SCI and optimize/treat vascular risk factors.
Afterwards,
Similar to cerebral infarcts, explore potential mechanisms for SCI and optimize/treat vascular risk factors.
14/
Key takeaways:
▶️Hyperacute myelopathy (<12 hours) ➡️ think SCI
▶️Recognize key imaging findings (pencil, owl eyes)
▶️Treatment is focused on increasing spinal cord perfusion
Key takeaways:
▶️Hyperacute myelopathy (<12 hours) ➡️ think SCI
▶️Recognize key imaging findings (pencil, owl eyes)
▶️Treatment is focused on increasing spinal cord perfusion
15/
Hope this was fun and educational!
We'll continue with another case next week!!
Hope this was fun and educational!
We'll continue with another case next week!!

Loading suggestions...