

1/ I walk up to the middle-aged woman who is terribly worried
This is the third time her husband is in the ICU
Each time, worse than the previous
This time, he is in a coma, and the reasons for him going into recurrent altered behavior remain elusive
Only one clue - cirrhosis
This is the third time her husband is in the ICU
Each time, worse than the previous
This time, he is in a coma, and the reasons for him going into recurrent altered behavior remain elusive
Only one clue - cirrhosis
2/ Shankar, her husband has diagnosed with cirrhosis just a two months ago
At the time, he had swelling of both feet and an evaluation revealed low platelets and features of cirrhosis on imaging
Absolutely no complications of cirrhosis
Complications of cirrhosis come in stages
At the time, he had swelling of both feet and an evaluation revealed low platelets and features of cirrhosis on imaging
Absolutely no complications of cirrhosis
Complications of cirrhosis come in stages
3/ Stage 1 and 2 feature changes associated with cirrhosis and high liver pressure (called portal hypertension)
Stage 3 and 4 is when clinical events in form of various complications take place
These include ascites (fluid in abdomen), vomiting blood or passage of black stools
Stage 3 and 4 is when clinical events in form of various complications take place
These include ascites (fluid in abdomen), vomiting blood or passage of black stools
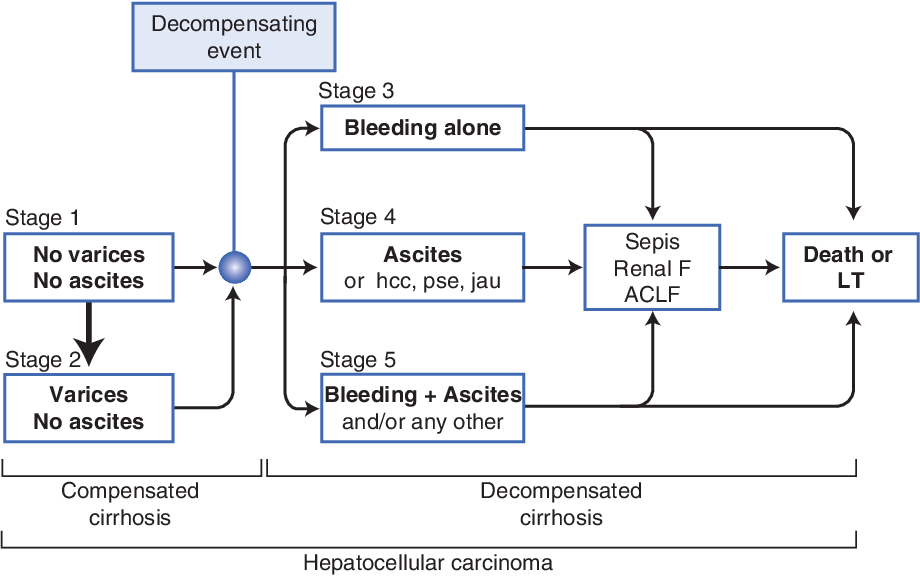
4/ In stages beyond these, patients develop features of liver failure - such as jaundice (defined as bilirubin levels > 3mg/dL)
and brain failure (called hepatic encephalopathy or HE)
In natural history of the cirrhosis, HE happens in advanced stages and predicts early death
and brain failure (called hepatic encephalopathy or HE)
In natural history of the cirrhosis, HE happens in advanced stages and predicts early death
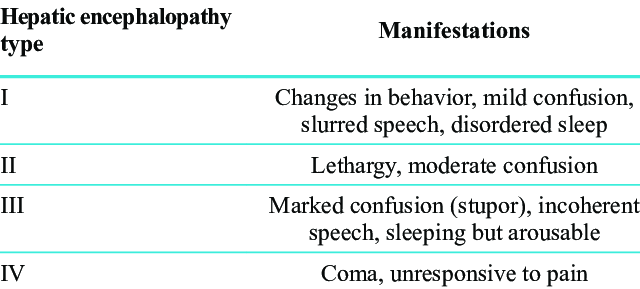
5/ In HE patients progress through various stages
From slight memory loss and difficulty in calculation to slurred speech, confusion and finally coma
30%-45% of cirrhosis patients experience HE (prevalence or commonness)
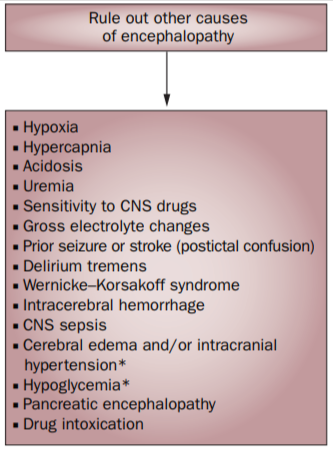
Diagnosing HE is pretty easy - rule out other causes...
From slight memory loss and difficulty in calculation to slurred speech, confusion and finally coma
30%-45% of cirrhosis patients experience HE (prevalence or commonness)
Diagnosing HE is pretty easy - rule out other causes...
6/ of brain failure or neurological dysfunction
So essentially, HE is a diagnosis of EXCLUSION
Other causes such as stroke, brain infections, brain tumors, intoxication, trauma etc.. has to be ruled out
Once HE is diagnosed, then the most important part is to look for the...
So essentially, HE is a diagnosis of EXCLUSION
Other causes such as stroke, brain infections, brain tumors, intoxication, trauma etc.. has to be ruled out
Once HE is diagnosed, then the most important part is to look for the...
7/ reason for precipitation of HE
In the ER, Shankar was being put on the ventilator because he is in a coma and chances of aspiration of saliva into his lungs was very high and lung failure was very high
They were small, loving, close knit family
Father, mother and daughter
In the ER, Shankar was being put on the ventilator because he is in a coma and chances of aspiration of saliva into his lungs was very high and lung failure was very high
They were small, loving, close knit family
Father, mother and daughter
8/ Their daughter was 22 years old, engaged to a gentleman and wedding was planned in three months
After the engagement, her father was diagnosed with cirrhosis and within two months of his diagnosis, he was admitted thrice with HE
And now in a coma, she was worried...
After the engagement, her father was diagnosed with cirrhosis and within two months of his diagnosis, he was admitted thrice with HE
And now in a coma, she was worried...
9/ that she would end up on wedding day, without her beloved Appa
My colleagues take a detailed history - Shankar was a teetotaler, a sweet man who followed doctors orders to the T and worked hard to make ends meet
He was overweight
No drug use apart from what was prescribed
My colleagues take a detailed history - Shankar was a teetotaler, a sweet man who followed doctors orders to the T and worked hard to make ends meet
He was overweight
No drug use apart from what was prescribed
10/ The first time he got sick, it started off with him mistaking the living room for the bathroom and was readying himself to urinate on the living room floor
Disoriented and confused, he was rushed to a nearby hospital where he was diagnosed with HE and treated accordingly
Disoriented and confused, he was rushed to a nearby hospital where he was diagnosed with HE and treated accordingly
11/ The second HE attack came after 3 weeks - this time, he was disoriented while riding his bike and crashed onto a pole very close to his home
No brain injuries, and again, treatment for HE improved his condition and he was taken home
The third time, he went into a coma...
No brain injuries, and again, treatment for HE improved his condition and he was taken home
The third time, he went into a coma...
12/ in front of my eyes
Time was running out and we had to find what was causing his recurrent brain failure
To make things worse, his liver functions were perfect and his cirrhosis was in stage 2 - HE is not expected in this supposedly stable stage
What was causing it?
Time was running out and we had to find what was causing his recurrent brain failure
To make things worse, his liver functions were perfect and his cirrhosis was in stage 2 - HE is not expected in this supposedly stable stage
What was causing it?
13/ When a patient with stable cirrhosis, presents with recurrent brain failure in the absence of identifiable causes for precipitation of HE it is called "spontaneous HE"
As we wait for the blood reports, we also send Shankar for a CT scan of the abdomen
This would help us...
As we wait for the blood reports, we also send Shankar for a CT scan of the abdomen
This would help us...
14/ identify an important cause for his supposed recurrent spontaneous HE
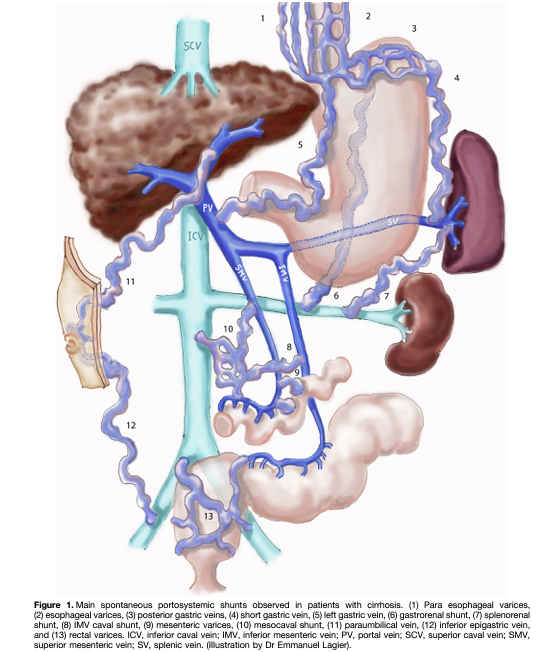
This is called as portosystemic shunts
Portosystemic shunts are LARGE blood vessels that form inside the abdomen in cirrhosis, when the liver pressure increases as the liver shrinks
When liver shrinks...
This is called as portosystemic shunts
Portosystemic shunts are LARGE blood vessels that form inside the abdomen in cirrhosis, when the liver pressure increases as the liver shrinks
When liver shrinks...
15/ the pressure inside the liver increases and blood flow into the liver gets difficult
But blood has to flow around
Akin to a block on the highway and how vehicles take the bypass and service roads, for the blood to flow, new large blood vessels form which bypass the liver
But blood has to flow around
Akin to a block on the highway and how vehicles take the bypass and service roads, for the blood to flow, new large blood vessels form which bypass the liver
16/ These are called portosystemic shunts or PSS
- they ferry the blood away from the liver and go straight into the system, including the brain
Without going into the liver, the bypassed blood is rich in ammonia - an important waste toxin that causes brain failure
- they ferry the blood away from the liver and go straight into the system, including the brain
Without going into the liver, the bypassed blood is rich in ammonia - an important waste toxin that causes brain failure
17/ In Shankar's case, we did not find any shunts and hence, large PSS as a cause for brain failure was ruled out
Meanwhile, the blood reports come
And everything was normal
Except two small things
Potassium levels - this was very low in Shankar
Ammonia - was raised
Meanwhile, the blood reports come
And everything was normal
Except two small things
Potassium levels - this was very low in Shankar
Ammonia - was raised
18/ Low potassium levels - called HYPOKALEMIA is an important risk factor that can precipitate HE
So we had it
We found the cause for his HE this admission
When potassium levels drop, capacity for urea synthesis reduce in the liver (urea generation occurs in liver, UREA CYCLE)
So we had it
We found the cause for his HE this admission
When potassium levels drop, capacity for urea synthesis reduce in the liver (urea generation occurs in liver, UREA CYCLE)
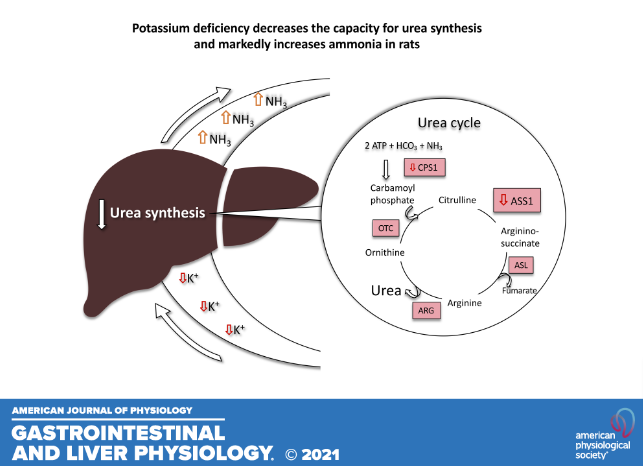
19/ and this leads to increase in ammonia which then cause brain failure
But also, when potassium goes low, it triggers conversion of amino acid glutamine in kidneys to excess ammonia
Excess ammonia then enters circulation, reaches brain and causes HE
Treatment was simple...
But also, when potassium goes low, it triggers conversion of amino acid glutamine in kidneys to excess ammonia
Excess ammonia then enters circulation, reaches brain and causes HE
Treatment was simple...

20/ Correct potassium levels and Shankar will be fine
So we start potassium correction for Shankar and tell his wife and daughter that, things are going to be well
But we did not yet, have the reason for Shankar's recurrent brain failure
So we ask the family about reasons...
So we start potassium correction for Shankar and tell his wife and daughter that, things are going to be well
But we did not yet, have the reason for Shankar's recurrent brain failure
So we ask the family about reasons...
21/ doctors who treated Shankar for the first and second attacks of brain failure gave them
'High ammonia', says his wife
'But potassium was also low Amma', says his daughter
I sit up, listen & ask, ' Both times?'
& they nod
'Can I see the discharge summaries'? I ask them
'High ammonia', says his wife
'But potassium was also low Amma', says his daughter
I sit up, listen & ask, ' Both times?'
& they nod
'Can I see the discharge summaries'? I ask them
22/ And we see something intriguing.
Shankar, during all his three attacks of brain failure had low potassium levels
This meant that not only he had recurrent HE, but he also had recurrent hypokalemia every time that gave rise to HE
Why was his potassium going low repeatedly?
Shankar, during all his three attacks of brain failure had low potassium levels
This meant that not only he had recurrent HE, but he also had recurrent hypokalemia every time that gave rise to HE
Why was his potassium going low repeatedly?
23/ And we know it was time..
Time we stopped being super-specialists and got back to the heart and soul of real medicine
Internal Medicine - back to the mothership
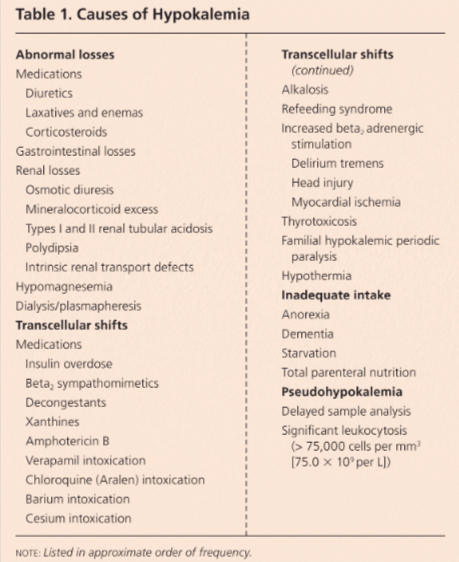
Causes of low potassium is a huge list
But we were interested in causes of recurrent low potassium
Time we stopped being super-specialists and got back to the heart and soul of real medicine
Internal Medicine - back to the mothership
Causes of low potassium is a huge list
But we were interested in causes of recurrent low potassium
24/ And to get to it, we needed the help of the best thing ever in clinical medicine practice
Algorithms
So we pull up an algorithm and try to figure out how Shankar was losing potassium
But first, we looked at his drugs list.
A host of drugs can cause low potassium...
Algorithms
So we pull up an algorithm and try to figure out how Shankar was losing potassium
But first, we looked at his drugs list.
A host of drugs can cause low potassium...
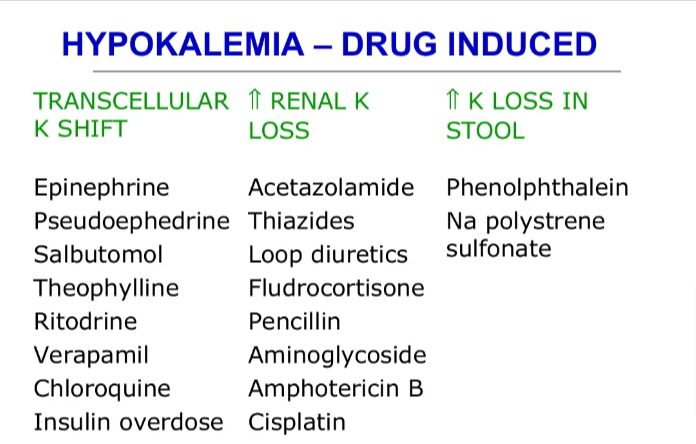
25/ and Shankar was not on any such.
So we move onto the algorithm to figure out why this was happening
Investigations require us to look at 2 things
If potassium was lost through kidneys or non-kidney causes &
potassium level in urine & % (fractional) excretion of potassium
So we move onto the algorithm to figure out why this was happening
Investigations require us to look at 2 things
If potassium was lost through kidneys or non-kidney causes &
potassium level in urine & % (fractional) excretion of potassium

26/ Following this pattern, we find that in Shankar...
Urine potassium was was high and his blood was alkaline (called metabolic alkalosis)
His admission blood pressures were on the higher side and this was true for every prior admission
And major potassium handling hormone,
Urine potassium was was high and his blood was alkaline (called metabolic alkalosis)
His admission blood pressures were on the higher side and this was true for every prior admission
And major potassium handling hormone,
27/ called aldosterone, secreted by adrenal glands was low
This was strange
Low potassium
High blood pressure
Alkaline blood
All were common at every admission
High aldosterone levels can cause these
But Shankar had low aldosterone levels
This was called..
This was strange
Low potassium
High blood pressure
Alkaline blood
All were common at every admission
High aldosterone levels can cause these
But Shankar had low aldosterone levels
This was called..
28/ Pseudo (false) hyperaldosteronism
- condition that mimics high aldosterone levels, when in fact, aldosterone levels were low or normal
This can happen in rare causes which include:
Endocrine diseases
Dietary factors
Genetic causes
- condition that mimics high aldosterone levels, when in fact, aldosterone levels were low or normal
This can happen in rare causes which include:
Endocrine diseases
Dietary factors
Genetic causes

29/
Endocrine and genetic diseases such as
Liddles syndrome
Apparent mineralocorticoid excess &
Congenital adrenal hyperplasia
DID NOT fit with main clinical and investigational features noted in Shankar
Endocrine and genetic diseases such as
Liddles syndrome
Apparent mineralocorticoid excess &
Congenital adrenal hyperplasia
DID NOT fit with main clinical and investigational features noted in Shankar

30/ So we were left with three other causes
that could cause
Pseudo hyperaldosteronism or clinical features that mimic high aldosterone levels when levels were in fact low or normal
Licorice consumption
A seldom used drug called carbenoxolone
Grape fruits
that could cause
Pseudo hyperaldosteronism or clinical features that mimic high aldosterone levels when levels were in fact low or normal
Licorice consumption
A seldom used drug called carbenoxolone
Grape fruits
31/ So we get back to the wife and daughter and ask them his dietary habits and they deny excessive use of
Licorice
Any other steroidal drugs
Grapefruits
Now we were truly lost
Without finding the cause of hypokalemia, Shankar was still at risk for brain failure because he..
Licorice
Any other steroidal drugs
Grapefruits
Now we were truly lost
Without finding the cause of hypokalemia, Shankar was still at risk for brain failure because he..
32/ was a cirrhosis patient and the chances of him getting through to attend his daughters wedding seemed very bleak
This depressed us and we did not know how to get through it
One day, while I was in the OPD, the staff comes in and tells me that Shankar's wife wanted to see me
This depressed us and we did not know how to get through it
One day, while I was in the OPD, the staff comes in and tells me that Shankar's wife wanted to see me
33/ I allowed her the time because I knew that we did everything we could to get to the root cause.
Even though Shankar would improve and get discharged from this episode (he was getting better on the ventilator, showing signs of waking up), we were not sure about his future.
Even though Shankar would improve and get discharged from this episode (he was getting better on the ventilator, showing signs of waking up), we were not sure about his future.
34/ The wife walks in and looks at me and I compose myself to apologize to her, because we thought we could do it, but we failed her too.
She speaks. 'Doctor, I thought long about the diet queries you asked me. And even though he did not consume any of those fruits you...
She speaks. 'Doctor, I thought long about the diet queries you asked me. And even though he did not consume any of those fruits you...
35/ mentioned, he was taking some laxative powder.'
I sit up and ask her the name of the powder
She says she did not know, because he kept it inside the bathroom shelf & she never looked at it.
Cirrhosis patients are usually prescribed lactulose - a safe laxative that helps..
I sit up and ask her the name of the powder
She says she did not know, because he kept it inside the bathroom shelf & she never looked at it.
Cirrhosis patients are usually prescribed lactulose - a safe laxative that helps..
36/ pass soft stools and also reduces ammonia
Lactulose did not suit Shankar - because a common side effect is excessive bloating and hence he went for some other laxative option, the name only he knew
'Only he can tell us and for that he has to be weaned off the ventilator'..
Lactulose did not suit Shankar - because a common side effect is excessive bloating and hence he went for some other laxative option, the name only he knew
'Only he can tell us and for that he has to be weaned off the ventilator'..
37/ I tell the wife.
Now every bit of energy and focus from the critical care team and Hepatology unit was to get Shankar off the ventilator, so that he can tell us his diagnosis.
We go all out treating his brain failure as per evidence and by the book
Even though it took us..
Now every bit of energy and focus from the critical care team and Hepatology unit was to get Shankar off the ventilator, so that he can tell us his diagnosis.
We go all out treating his brain failure as per evidence and by the book
Even though it took us..

38/ more than a week to get to our goal, we finally wean off Shankar from the ventilator
His voice is raspy and he is weak
His swallowing is affected and he is dazed
The critical care nursing team do an intense job on rehabilitating him from speech, swallow and nutritional..
His voice is raspy and he is weak
His swallowing is affected and he is dazed
The critical care nursing team do an intense job on rehabilitating him from speech, swallow and nutritional..
39/ point of view.
And after another week in the ICU, Shankar is finally shifted out to the room
His potassium levels are fine
His blood pressures are fine
His blood is no more alkaline
And that day finally came, when on rounds, I could ask him about the powder he was having.
And after another week in the ICU, Shankar is finally shifted out to the room
His potassium levels are fine
His blood pressures are fine
His blood is no more alkaline
And that day finally came, when on rounds, I could ask him about the powder he was having.
40/ Kayam Churnam is a traditional Ayurvedic medicine used to treat constipation.
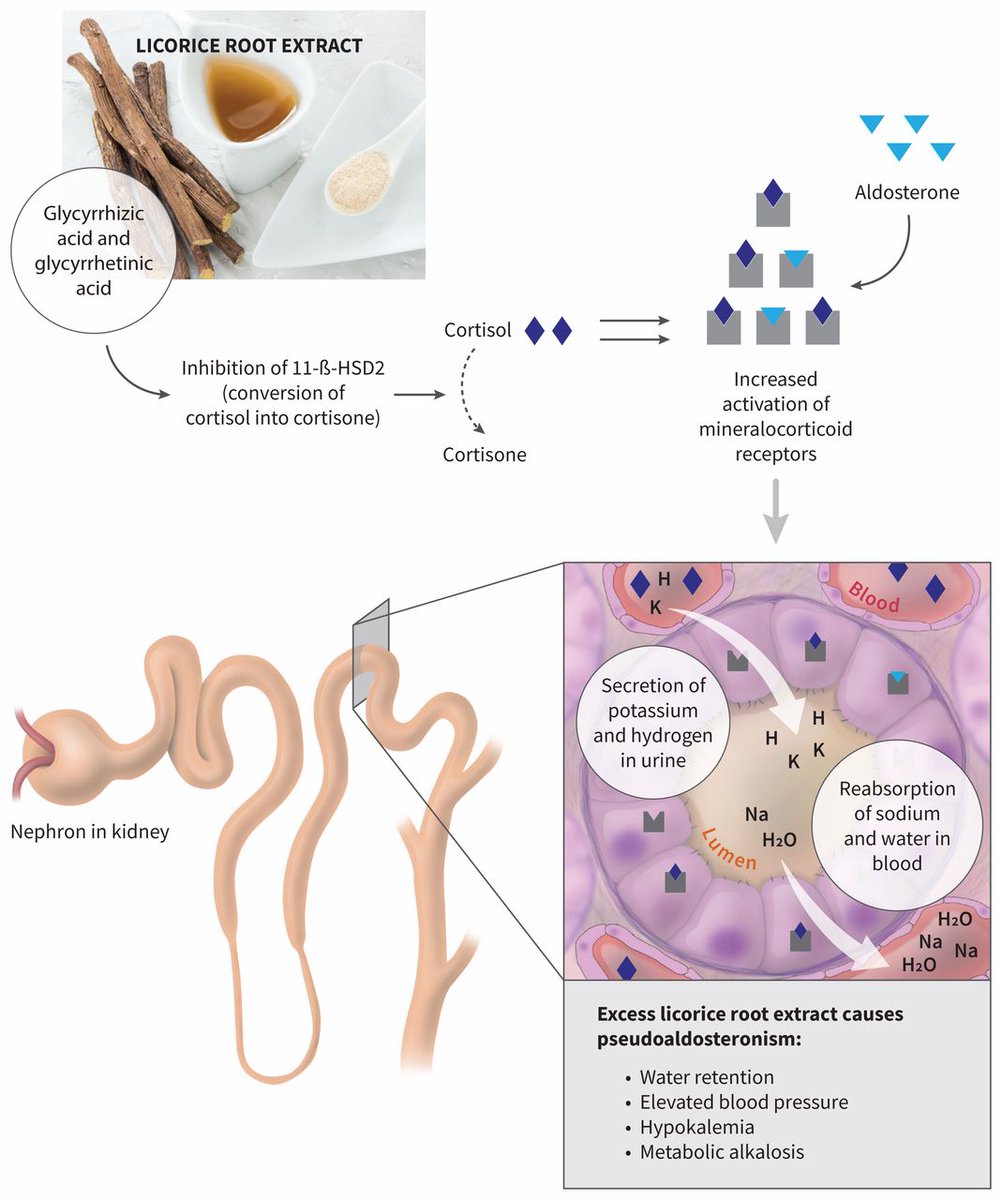
It contains Senna leaves which are known herbal laxatives and more importantly, Yashtimadhu or Glycyrrhiza glabra - also called Licorice.
Licorice consumption has been very strongly associated..
It contains Senna leaves which are known herbal laxatives and more importantly, Yashtimadhu or Glycyrrhiza glabra - also called Licorice.
Licorice consumption has been very strongly associated..


41/ with low potassium.
Excessive licorice intake is a well-known cause of hypertension
The licorice component glycyrrhizin inhibits an enzyme in the kidney
This leads to rise in the hormone cortisol level leading to loss of potassium and increase in blood pressure!
Excessive licorice intake is a well-known cause of hypertension
The licorice component glycyrrhizin inhibits an enzyme in the kidney
This leads to rise in the hormone cortisol level leading to loss of potassium and increase in blood pressure!
42/ The problem with Kayam Churnam and products that contain Senna laxatives is that they reach a threshold and then they do not work, unless doses are increased
Across 2 months of daily use, Shankar had slowly & steadily increased Kayam use which led to severe potassium loss..
Across 2 months of daily use, Shankar had slowly & steadily increased Kayam use which led to severe potassium loss..
43/ leading to hypokalemia which thereafter precipitated hepatic encephalopathy or brain failure.
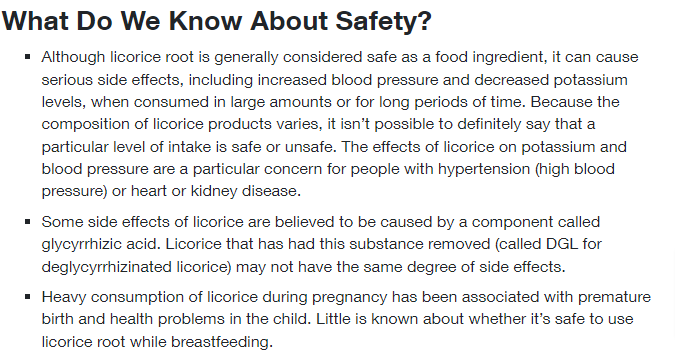
Licorice herbal products MUST BE taken with caution especially in high risk patient groups such as cirrhosis
They may appear and are marketed as safe, but truth is not always sweet
Licorice herbal products MUST BE taken with caution especially in high risk patient groups such as cirrhosis
They may appear and are marketed as safe, but truth is not always sweet
44/ After spending almost three weeks in the hospital, Shankar was finally discharged home
Back home, first thing he did was throw away Kayam Churnam out the window
Shankar teary eyed, watched his daughter dance with her husband on the day of her wedding
He sent me a message..
Back home, first thing he did was throw away Kayam Churnam out the window
Shankar teary eyed, watched his daughter dance with her husband on the day of her wedding
He sent me a message..
45/ on that day.
It did not contain any words.
Only two emoticons
This one <3 and :-)
It has been two years
Shankar has never had a brain failure since the last time we fought for him and he fought on the ventilator.
It did not contain any words.
Only two emoticons
This one <3 and :-)
It has been two years
Shankar has never had a brain failure since the last time we fought for him and he fought on the ventilator.
Loading suggestions...