

1/19
A middle-aged man presents with acute sudden-onset dyspnea and hypotension. He is sitting upright. What do you notice? Let’s see if we can figure out the cause of hypotension.
A middle-aged man presents with acute sudden-onset dyspnea and hypotension. He is sitting upright. What do you notice? Let’s see if we can figure out the cause of hypotension.

2/19
First.
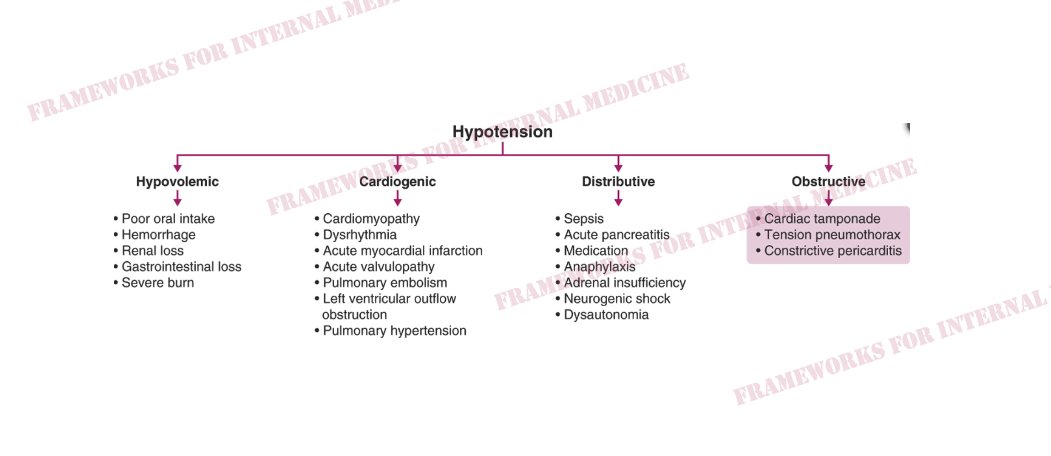
What are the 4 basic mechanisms of hypotension?
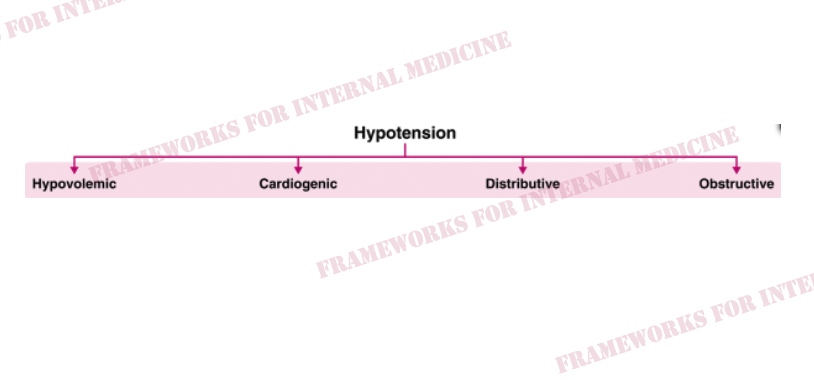
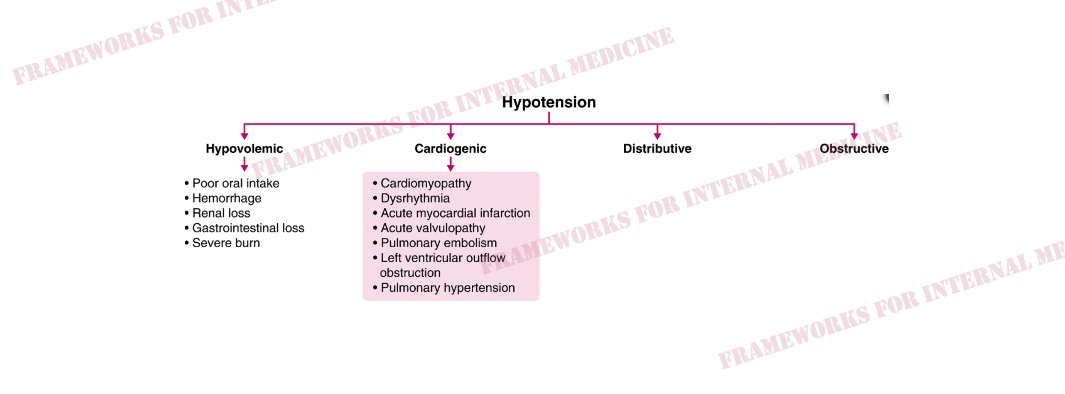
Hypotension can be hypovolemic, cardiogenic, distributive, or obstructive.
First.
What are the 4 basic mechanisms of hypotension?
Hypotension can be hypovolemic, cardiogenic, distributive, or obstructive.
3/19
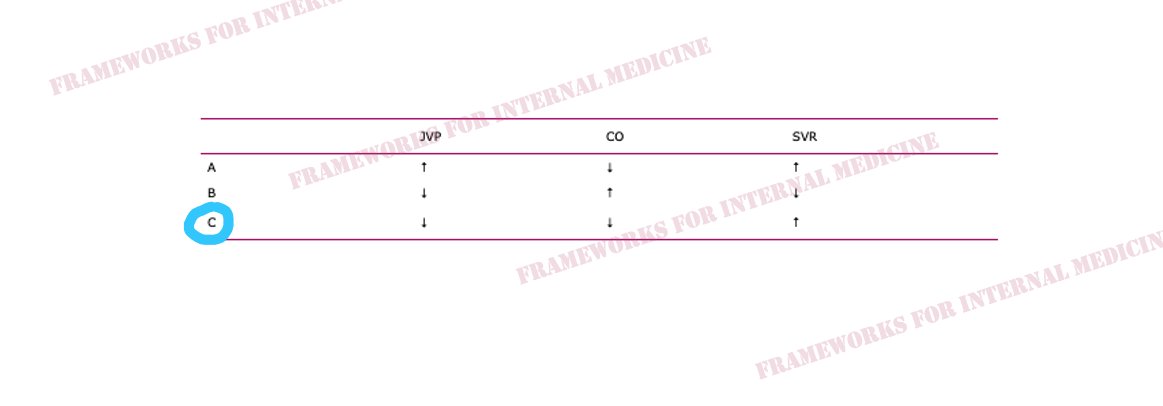
Hypovolemic hypotension occurs as a result of decreased hydrostatic pressure within blood vessels, and decreased cardiac preload with an associated decrease in cardiac output. It is characterized by decreased CVP (primary issue), decreased CO, and increased SVR (choice C).
Hypovolemic hypotension occurs as a result of decreased hydrostatic pressure within blood vessels, and decreased cardiac preload with an associated decrease in cardiac output. It is characterized by decreased CVP (primary issue), decreased CO, and increased SVR (choice C).
4/19
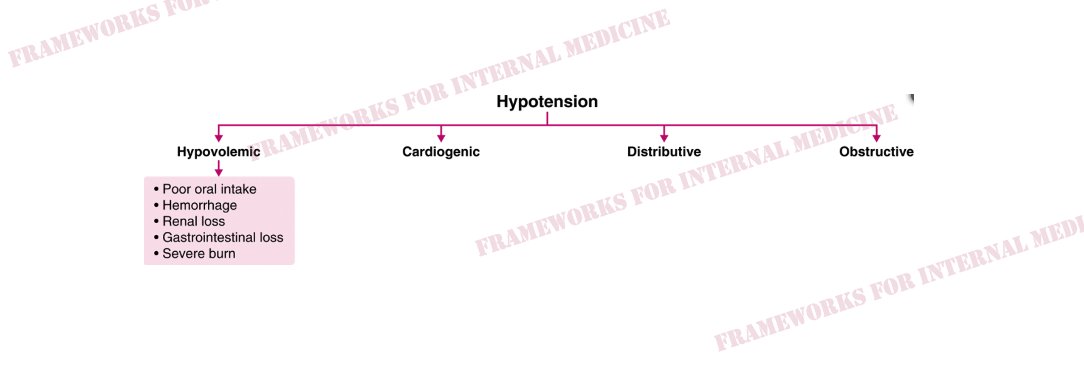
What are the causes of hypovolemic hypotension?
What are the causes of hypovolemic hypotension?
5/19
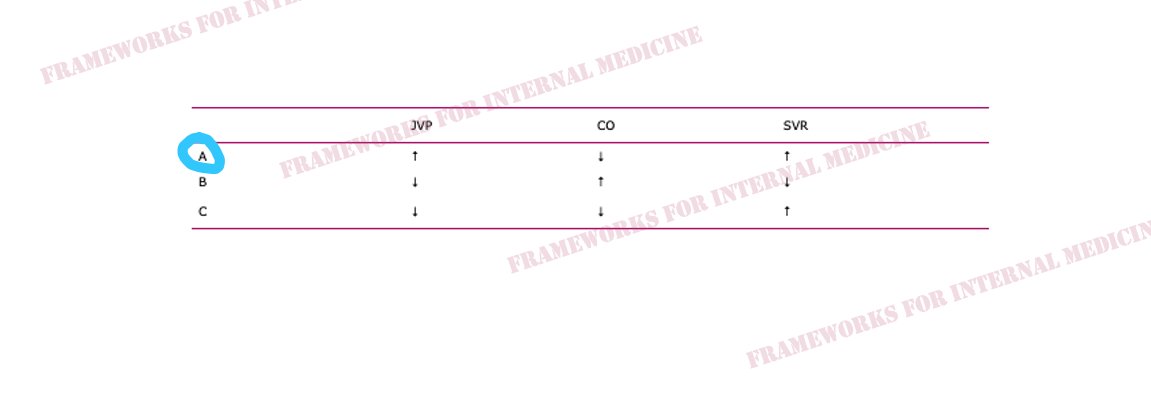
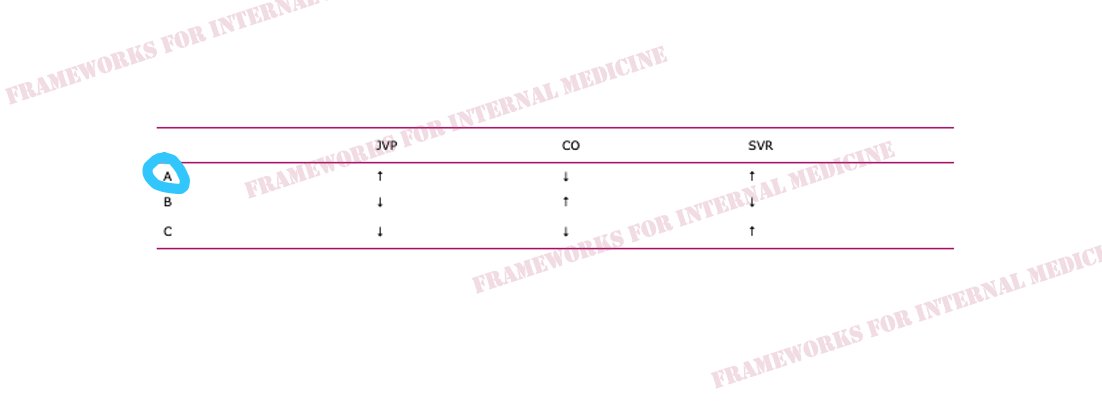
Cardiogenic hypotension occurs as a result of pump failure with an associated decrease in cardiac output. It is characterized by increased CVP, decreased CO (primary issue), and increased SVR (choice A).
Cardiogenic hypotension occurs as a result of pump failure with an associated decrease in cardiac output. It is characterized by increased CVP, decreased CO (primary issue), and increased SVR (choice A).
6/19
What are the causes of cardiogenic hypotension?
What are the causes of cardiogenic hypotension?
7/19
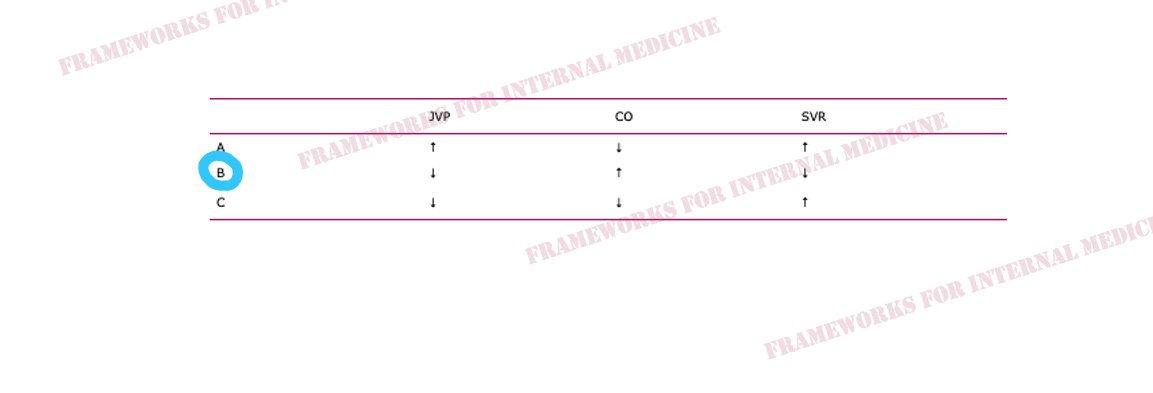
Distributive hypotension occurs as a result of pathologic peripheral vasodilation with an associated decrease in SVR. It is characterized by decreased CVP, increased CO, and decreased SVR (primary issue) (choice B).
Distributive hypotension occurs as a result of pathologic peripheral vasodilation with an associated decrease in SVR. It is characterized by decreased CVP, increased CO, and decreased SVR (primary issue) (choice B).
8/19
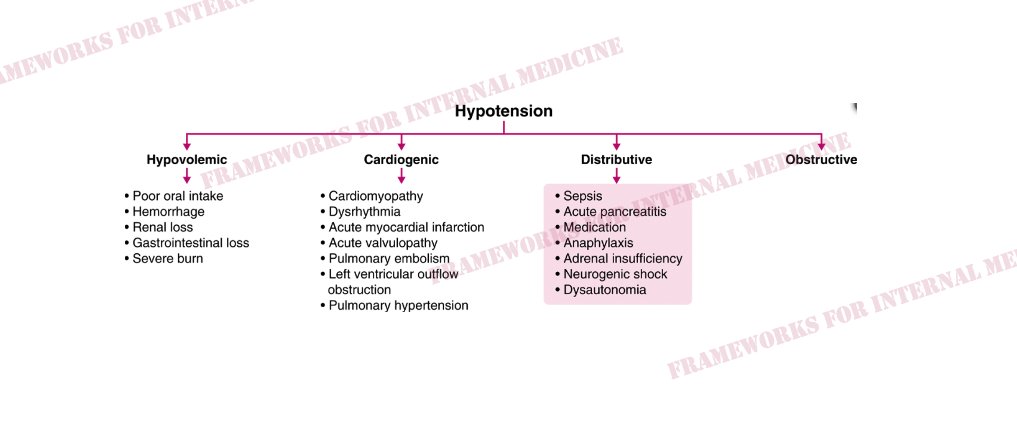
What are the causes of distributive hypotension?
What are the causes of distributive hypotension?
9/19
Obstructive hypotension occurs as a result of decreased cardiac filling with an associated decrease in both preload and cardiac output. It is characterized by increased CVP (primary issue), decreased CO, and increased SVR (choice A).
Obstructive hypotension occurs as a result of decreased cardiac filling with an associated decrease in both preload and cardiac output. It is characterized by increased CVP (primary issue), decreased CO, and increased SVR (choice A).
10/19
What are the causes of obstructive hypotension?
What are the causes of obstructive hypotension?
11/19
Physical examination is critical in the evaluation of hypotension. Our surrogate for CVP is the JVP; our surrogate for CO is the strength of the peripheral pulse; and the surrogate for SVR is warm/cool extremities. Here is Quincke’s pulse in a patient with septic shock.
Physical examination is critical in the evaluation of hypotension. Our surrogate for CVP is the JVP; our surrogate for CO is the strength of the peripheral pulse; and the surrogate for SVR is warm/cool extremities. Here is Quincke’s pulse in a patient with septic shock.

12/19
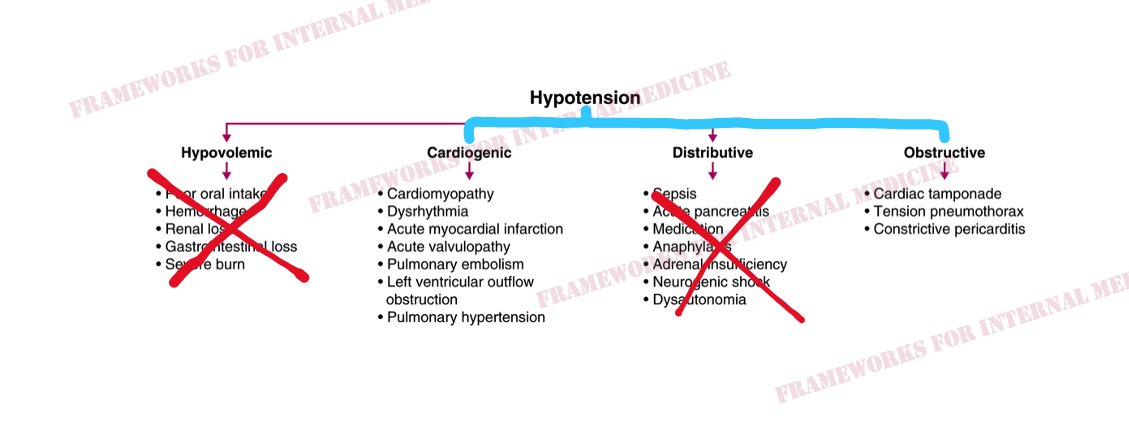
Back to our patient. His extremities are cool to the touch. What did you notice in the neck? JVP is elevated. This immediately cuts our differential diagnosis in half.
Back to our patient. His extremities are cool to the touch. What did you notice in the neck? JVP is elevated. This immediately cuts our differential diagnosis in half.
13/19
Our patient could have either cardiogenic or obstructive hypotension. Let’s go a little deeper. What do you notice in this video of our patient? (Turn sound up.)
Our patient could have either cardiogenic or obstructive hypotension. Let’s go a little deeper. What do you notice in this video of our patient? (Turn sound up.)

14/19
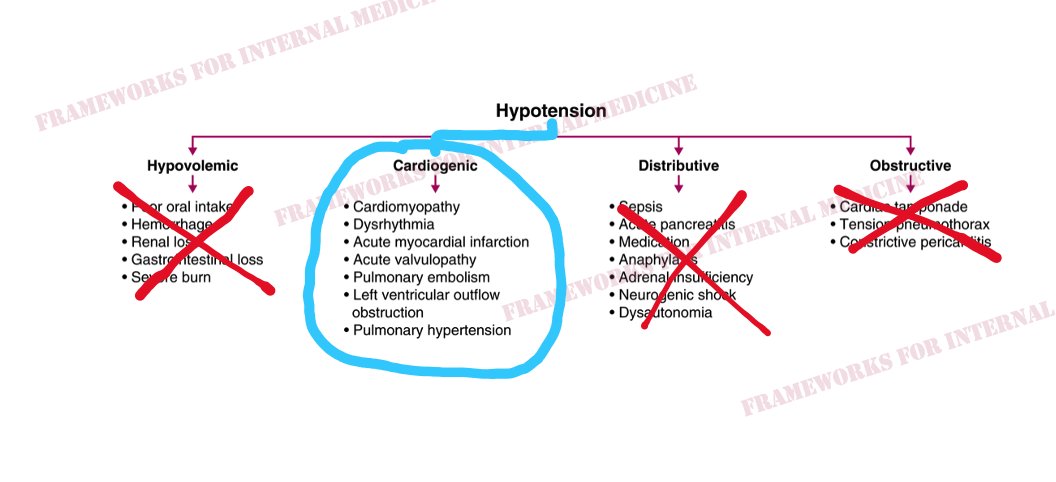
Contrary to popular believe, Kussmaul’s sign does not occur in pure cardiac tamponade. It can occur in constrictive pericarditis (or effusive-constrictive pericarditis) but the sudden-onset of symptoms points away from this. Cardiogenic hypotension it is. But from what?
Contrary to popular believe, Kussmaul’s sign does not occur in pure cardiac tamponade. It can occur in constrictive pericarditis (or effusive-constrictive pericarditis) but the sudden-onset of symptoms points away from this. Cardiogenic hypotension it is. But from what?
15/19
Is there a clue in the neck veins? You bet there is. Let's look at the original video. Which component of the waveform stands out to you?
Is there a clue in the neck veins? You bet there is. Let's look at the original video. Which component of the waveform stands out to you?

16/19
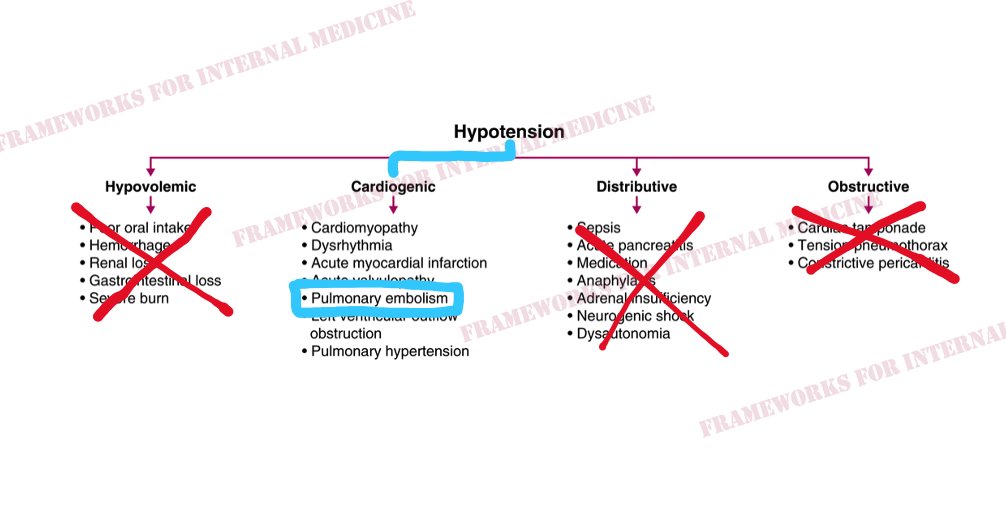
The giant a wave, as well as Kussmaul’s sign in the other video, lead us to causes of RV failure. And so does our patient's RV heave, shown below.
The giant a wave, as well as Kussmaul’s sign in the other video, lead us to causes of RV failure. And so does our patient's RV heave, shown below.

17/19
As we ponder the causes of sudden-onset RV failure, we begin to narrow our focus. And we anticipate what we might hear when we listen to the heart. (Sound up.)
"The ears can't hear what the mind doesn't know."
As we ponder the causes of sudden-onset RV failure, we begin to narrow our focus. And we anticipate what we might hear when we listen to the heart. (Sound up.)
"The ears can't hear what the mind doesn't know."

18/19
S2 is split. And the second of the two sounds (P2) is louder than the first (A2). This patient has an acute pulmonary embolism.
S2 is split. And the second of the two sounds (P2) is louder than the first (A2). This patient has an acute pulmonary embolism.
19//19
Hope you found this thread on hypotension helpful. A common cross-cover call for new interns in July. Keep this framework for reference. History and exam are all you need to make most diagnoses.
For more: amazon.com
Media from: Physical Diagnosis PDX
Hope you found this thread on hypotension helpful. A common cross-cover call for new interns in July. Keep this framework for reference. History and exam are all you need to make most diagnoses.
For more: amazon.com
Media from: Physical Diagnosis PDX
Loading suggestions...