

1/8
ELEVATED PT and aPTT
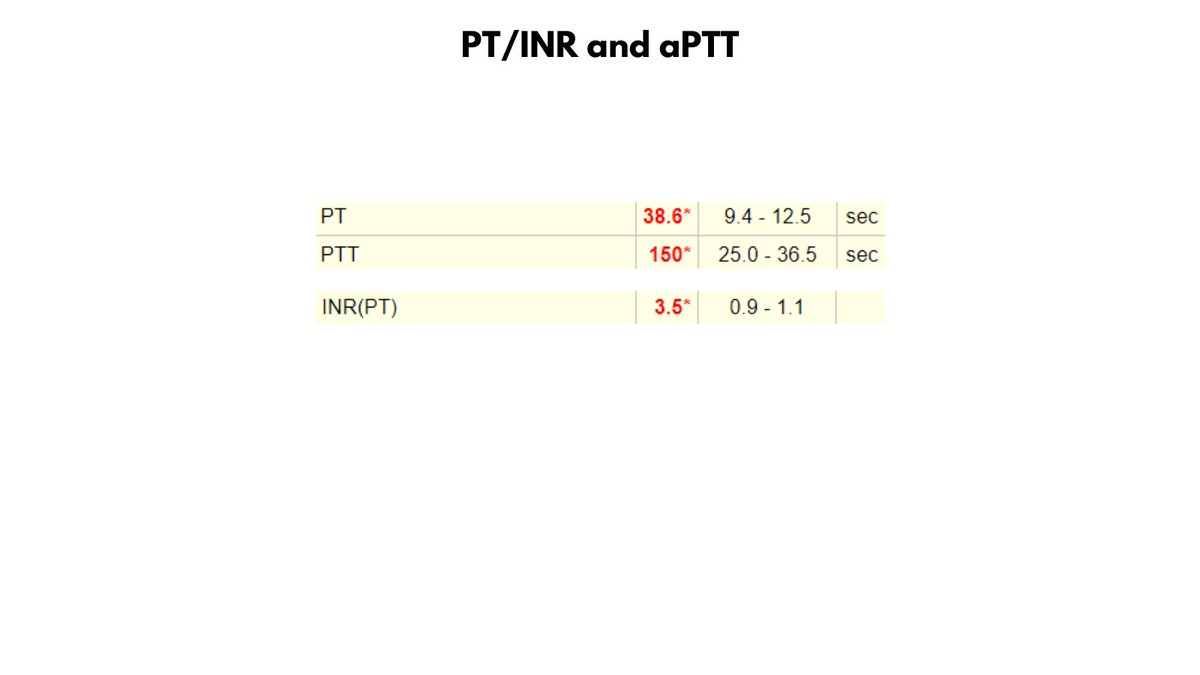
66 yo M with history of renal transplant presents to ED with swelling and pain of left thigh. CT shows large hematoma in the left rectus femoris muscle. Hb 6.9 (baseline 10), Plts 345K, aPTT > 150, PT 38.6 (aPTT/PT previously normal).
What is your ddx?
ELEVATED PT and aPTT
66 yo M with history of renal transplant presents to ED with swelling and pain of left thigh. CT shows large hematoma in the left rectus femoris muscle. Hb 6.9 (baseline 10), Plts 345K, aPTT > 150, PT 38.6 (aPTT/PT previously normal).
What is your ddx?
2/8
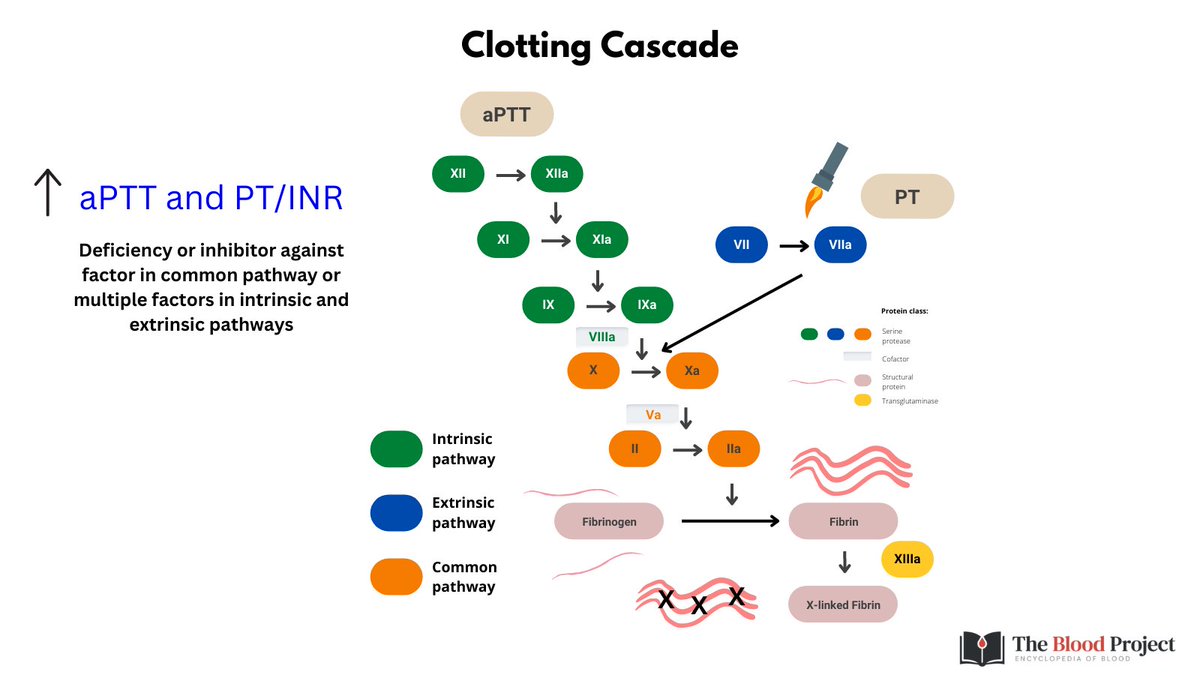
Elevated aPTT/PT = deficiency or inhibitor against factor(s) in the common pathway (FX, FII, FV) or multiple factors in the intrinsic and extrinsic pathways (as occurs in DIC, liver disease, heparin use, vitamin K def).
What questions and tests would you ask/order next?
Elevated aPTT/PT = deficiency or inhibitor against factor(s) in the common pathway (FX, FII, FV) or multiple factors in the intrinsic and extrinsic pathways (as occurs in DIC, liver disease, heparin use, vitamin K def).
What questions and tests would you ask/order next?
3/8
1. INHBITOR OR DEFICIENCY?
Mixing study - aPTT and PT corrected with 50:50 mix patient: normal plasma, indicating absolute deficiency rather than a neutralizing inhibitor.
2. WHICH FACTOR(S) ARE AFFEFCTED?
Factor assays revealed FV activity 2%
What are you thinking?
1. INHBITOR OR DEFICIENCY?
Mixing study - aPTT and PT corrected with 50:50 mix patient: normal plasma, indicating absolute deficiency rather than a neutralizing inhibitor.
2. WHICH FACTOR(S) ARE AFFEFCTED?
Factor assays revealed FV activity 2%
What are you thinking?

4/8
The data are c/w acquired absolute deficiency of FV, rarely reported in amyloidosis secondary to absorption of FV onto amyloid fibrils (though deficiency of FX more common in this setting). Work up did not reveal any evidence of amyloidosis.
The data are c/w acquired absolute deficiency of FV, rarely reported in amyloidosis secondary to absorption of FV onto amyloid fibrils (though deficiency of FX more common in this setting). Work up did not reveal any evidence of amyloidosis.
5/8
An alternative explanation is an anti-FV antibody that increases the clearance of FV.
A pro-clearance antibody would not interfere with FV in the mixing study, which would explain the apparent correction in that test.
How would you treat this patient?
An alternative explanation is an anti-FV antibody that increases the clearance of FV.
A pro-clearance antibody would not interfere with FV in the mixing study, which would explain the apparent correction in that test.
How would you treat this patient?
6/8
1. FFP 15-20 ml/kg/day to maintain FV level >20-30%
2. If bleeding worsens, treatment options include:
2a. Bypassing agents (rFVII or FEIBA)
2b. Platelet transfusions (platelets are a sustainable source of FV)
3. Prednisone/CSA/IVIG for presumed autoimmune mechanisms.
1. FFP 15-20 ml/kg/day to maintain FV level >20-30%
2. If bleeding worsens, treatment options include:
2a. Bypassing agents (rFVII or FEIBA)
2b. Platelet transfusions (platelets are a sustainable source of FV)
3. Prednisone/CSA/IVIG for presumed autoimmune mechanisms.
7/8
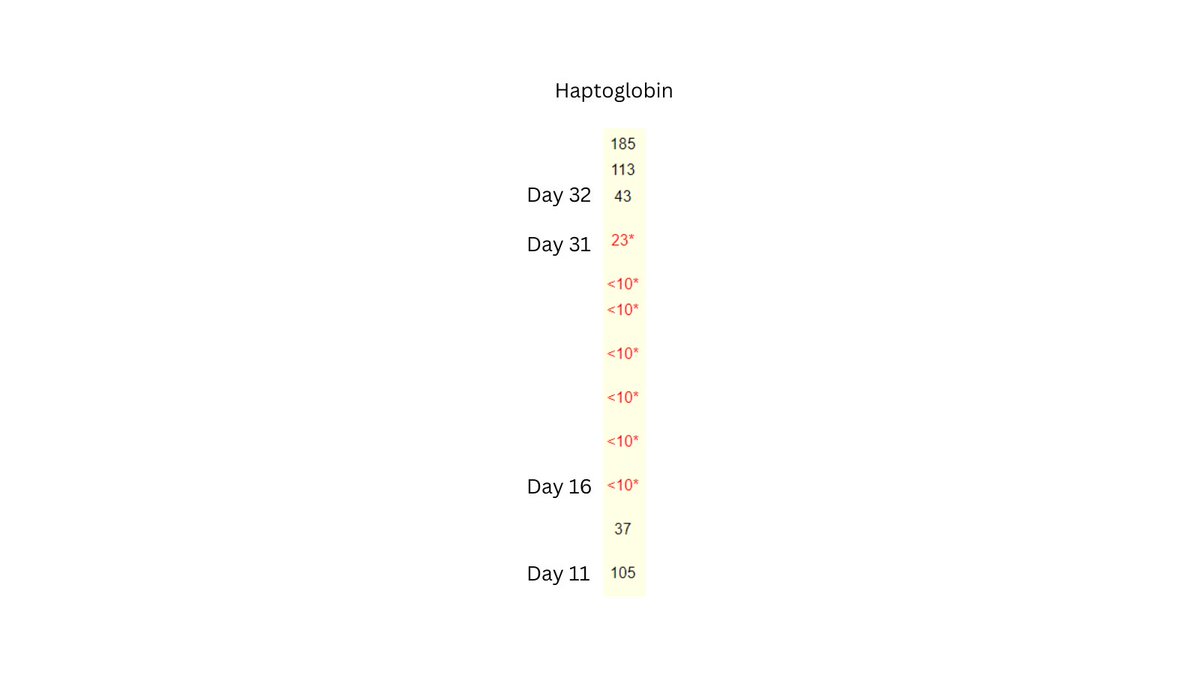
Factor V levels spontaneously normalized over the next 5 weeks. The precise cause of the deficiency/antibody was never determined.
Check out the labs in the graphic. Why did the haptoglobin fall several days later?
Factor V levels spontaneously normalized over the next 5 weeks. The precise cause of the deficiency/antibody was never determined.
Check out the labs in the graphic. Why did the haptoglobin fall several days later?
8/8
Resorption of hematoma - led to reduced haptoglobin, increased LDH/bilirubin/AST.
For more information on FV deficiency, see:
thebloodproject.com
Resorption of hematoma - led to reduced haptoglobin, increased LDH/bilirubin/AST.
For more information on FV deficiency, see:
thebloodproject.com
Loading suggestions...