

I was asked to talk about post myocardial infarction VSD for #SCAI2023 recently. In 8 mins I was a bit limited, so here's an expanded thread
Apologies that the movie compression makes things a bit jumpy, & if Twitter messes up the movie cropping I will add again at the end
1/
Apologies that the movie compression makes things a bit jumpy, & if Twitter messes up the movie cropping I will add again at the end
1/

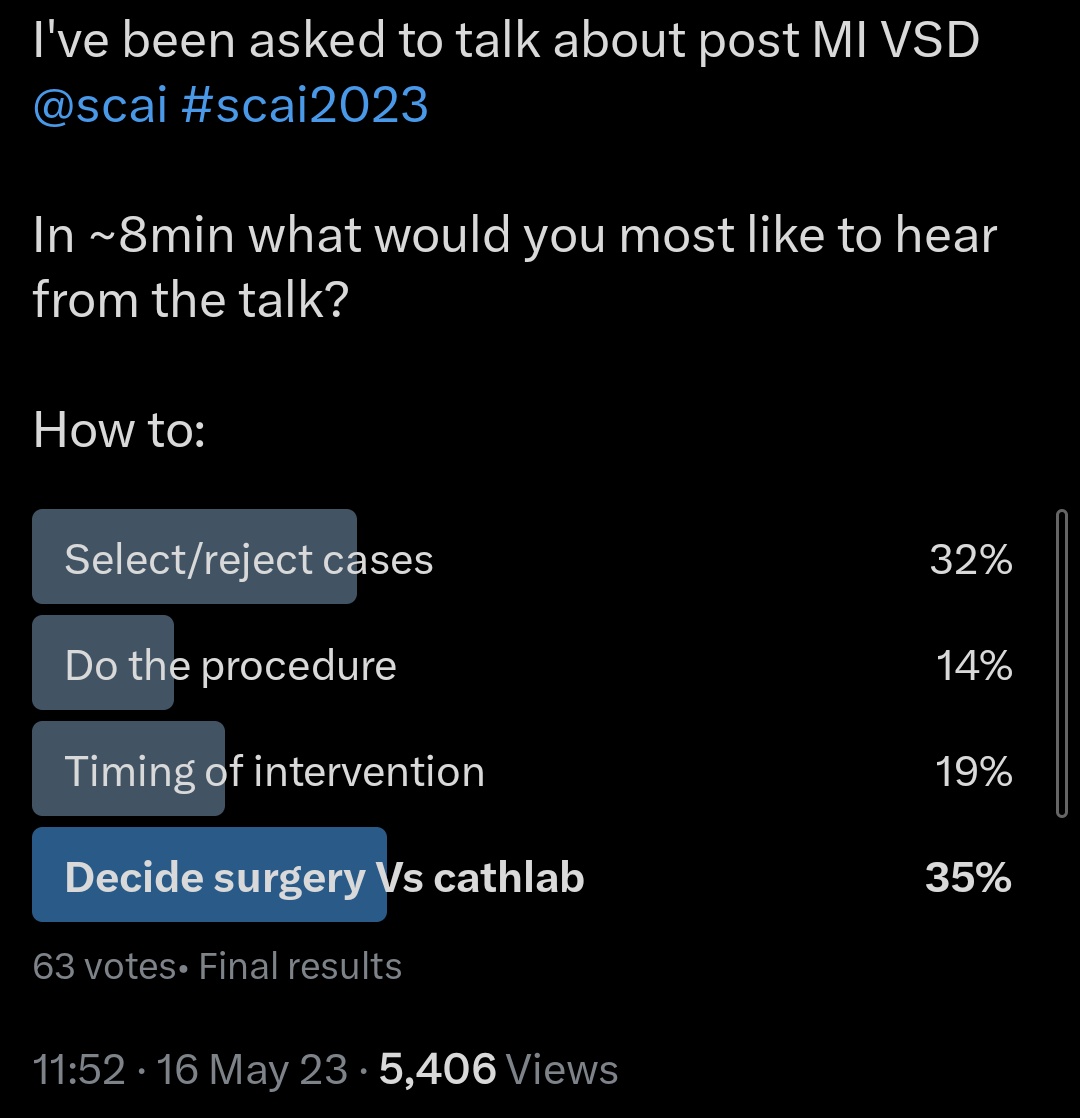
The pre-talk poll wanted coverage of 2 areas
Which patients not to treat?
And for those offered invasive surgery or percutaneous closure device - how to choose between the two?
I've added a bit of a "how to" at the end
2/
Which patients not to treat?
And for those offered invasive surgery or percutaneous closure device - how to choose between the two?
I've added a bit of a "how to" at the end
2/
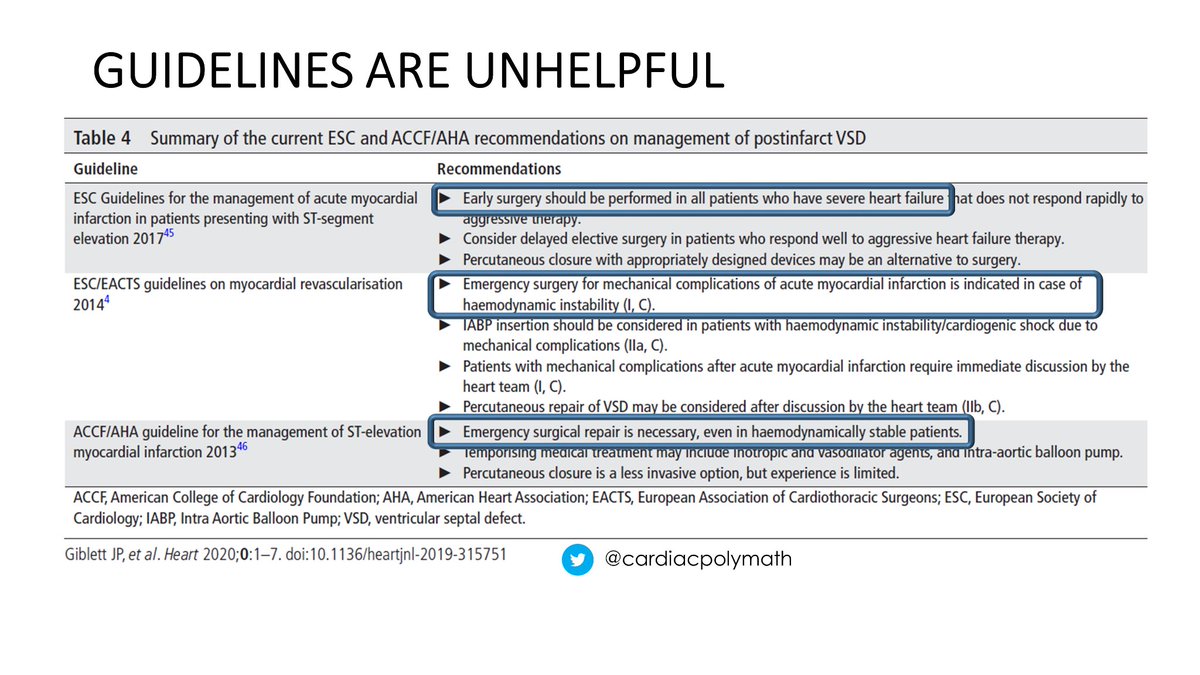
Guidelines exist but are unhelpful. No consensus on
1) when ("Early" Vs "Emergency")
Or
2) what ("heart failure" "hemodynamic instability" or "all")
To treat
Devices as an alternative to surgery"in some centres" but data lacking
Stephen Hawking had a nice phrase for it
3/
1) when ("Early" Vs "Emergency")
Or
2) what ("heart failure" "hemodynamic instability" or "all")
To treat
Devices as an alternative to surgery"in some centres" but data lacking
Stephen Hawking had a nice phrase for it
3/
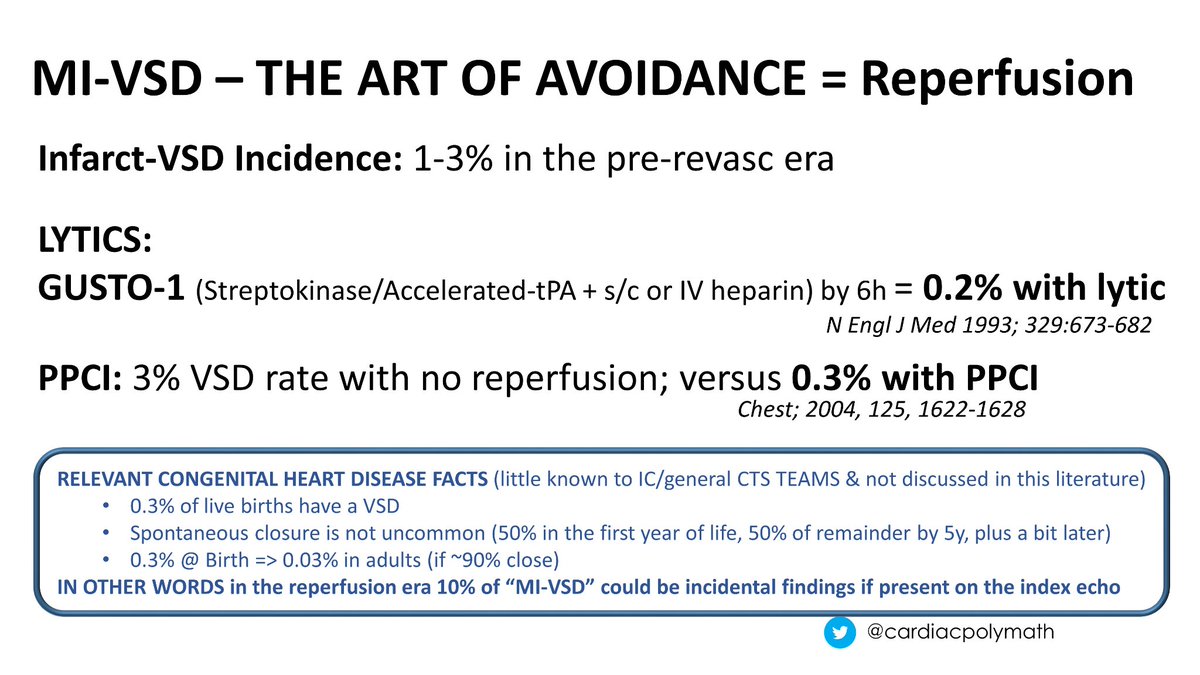
The prognosis of MI-VSD is poor - 95% mortality with medical therapy
The good news is that it can be avoided by prompt reperfusion (⬇️10x)
Ever wonder what was special about that 5% who survived with tablets?
There's a good chance some of these are VSDs present from birth
4/
The good news is that it can be avoided by prompt reperfusion (⬇️10x)
Ever wonder what was special about that 5% who survived with tablets?
There's a good chance some of these are VSDs present from birth
4/
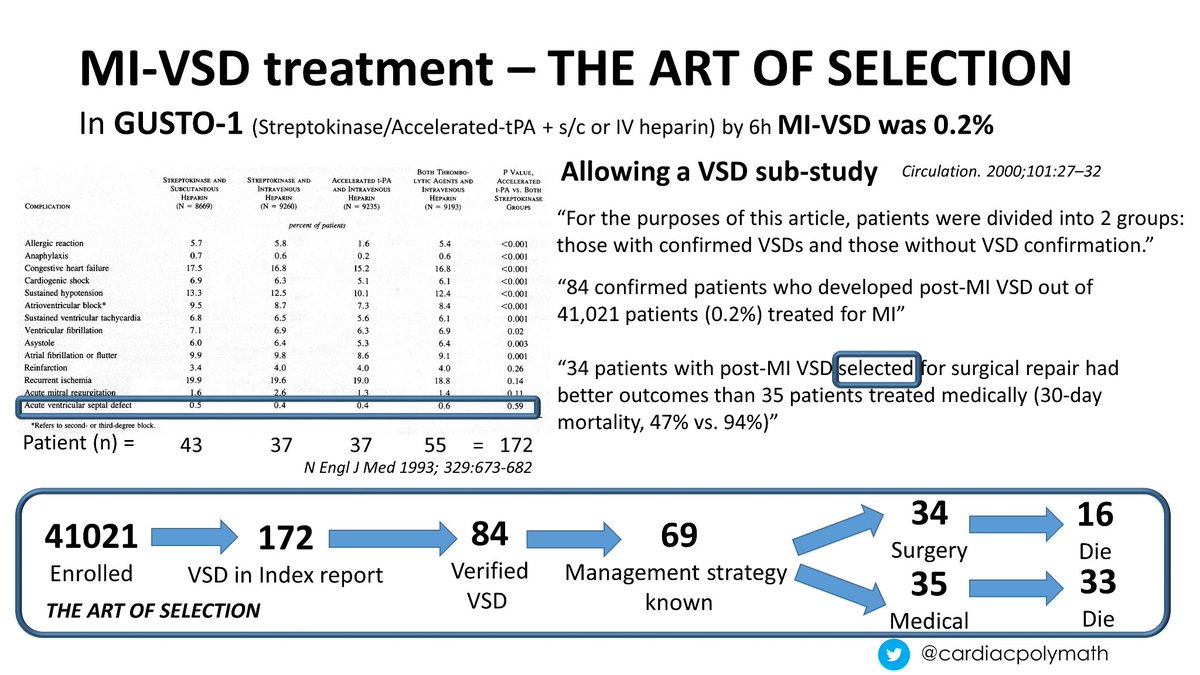
As we've never had an RCT in this area it is impossible to unpick the role that case selection has on outcomes
However it is clear that many patients are deemed to have no options beyond medical therapy (35 PT from GUSTO), only 34 getting surgery
30d mortality ~95% Vs 50%
5/
However it is clear that many patients are deemed to have no options beyond medical therapy (35 PT from GUSTO), only 34 getting surgery
30d mortality ~95% Vs 50%
5/
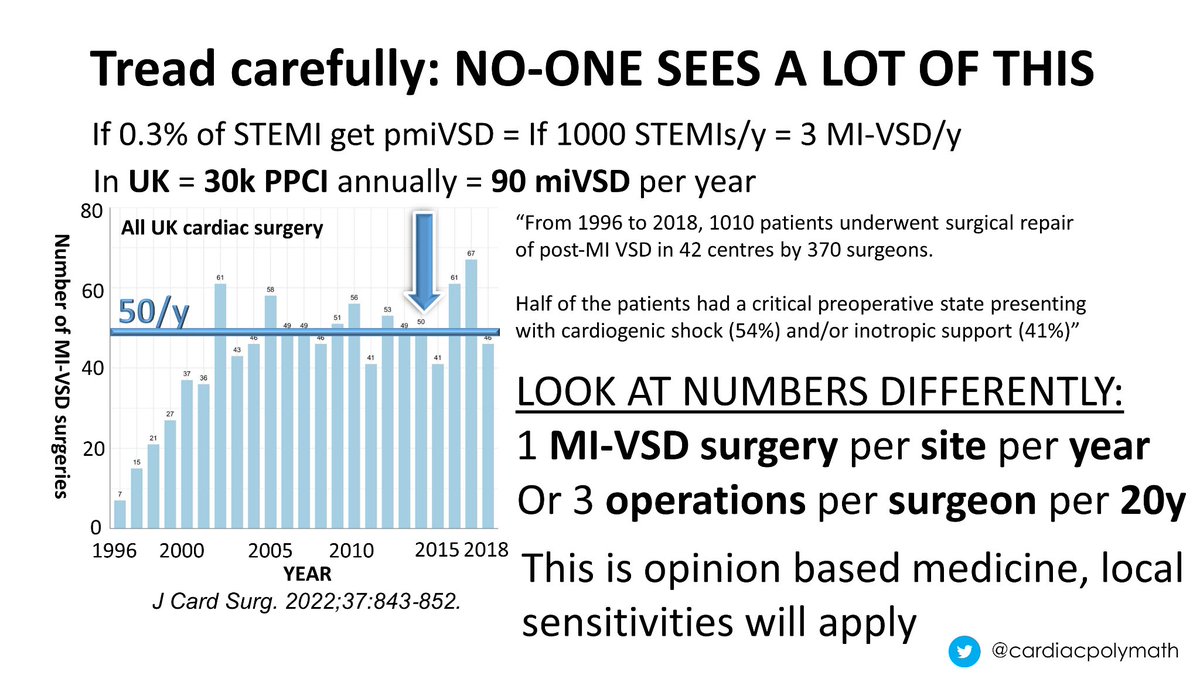
Cardiogenic shock is a difficult area to study - this is cardiogenic shock + mechanical complication (even harder)
Using whole UK cardiac surgery data, on average a centre might see 2 of these a year, & operate on 1 of them
A surgeon in a career may operate on 3
6/
Using whole UK cardiac surgery data, on average a centre might see 2 of these a year, & operate on 1 of them
A surgeon in a career may operate on 3
6/
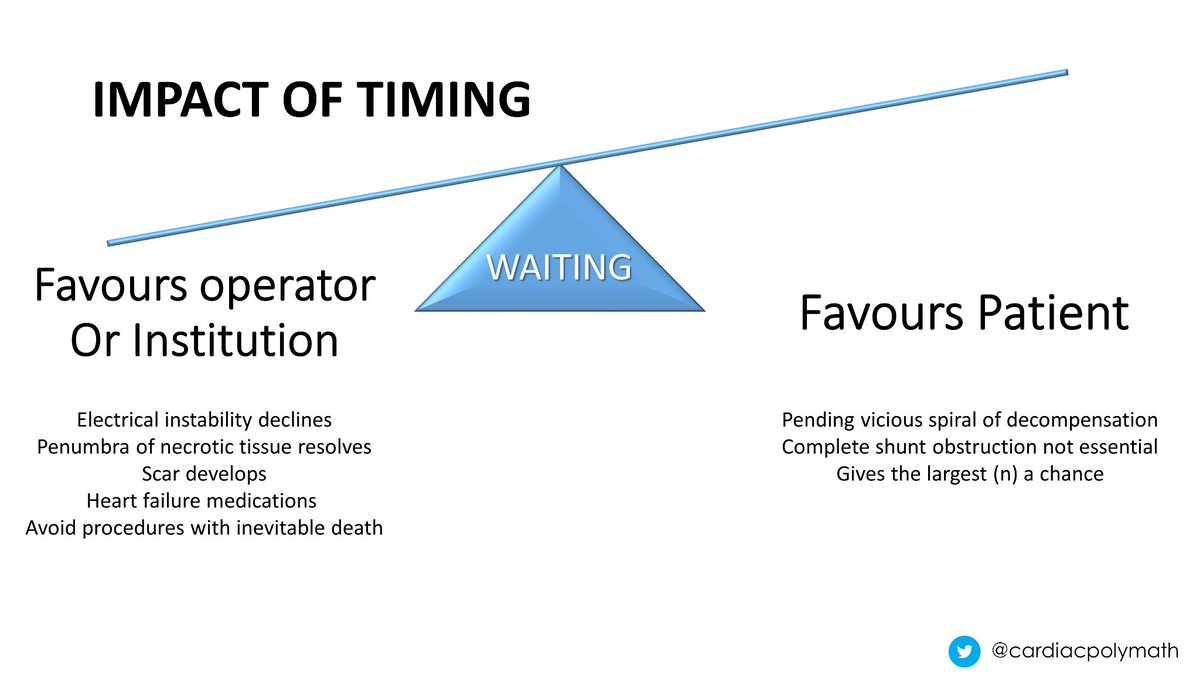
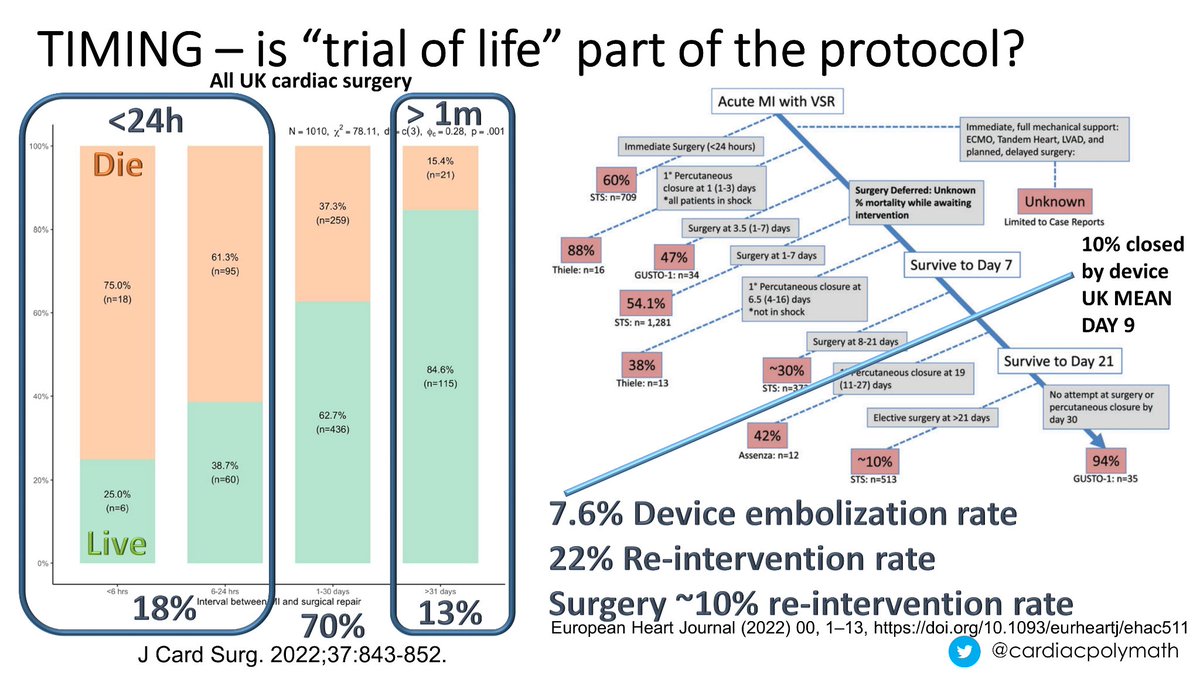
From the data we have collected, timing of intervention (surgery or catheter) appears important
The longer you wait, the better the outcomes
But waiting too long might deny some patients a chance to improve dismal odds (95% mortality) to long odds (<95% 30d mortality)
7/
The longer you wait, the better the outcomes
But waiting too long might deny some patients a chance to improve dismal odds (95% mortality) to long odds (<95% 30d mortality)
7/
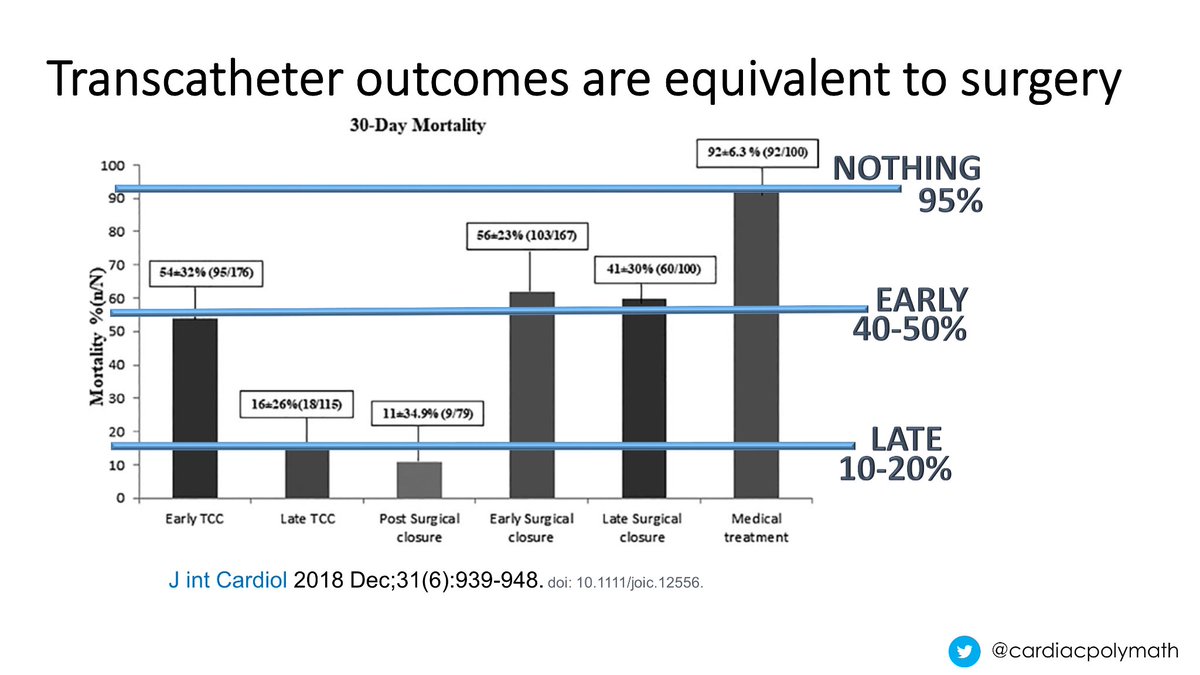
The impact is striking
Surgery<24h = ~80% mortality
"Early" intervention= 50% mortality
"Late" intervention= 10-20% mortality
Although the two routes to MI-VSD closure are different with devices or surgery, outcomes are about the same
Both appear better than tablets alone
8/
Surgery<24h = ~80% mortality
"Early" intervention= 50% mortality
"Late" intervention= 10-20% mortality
Although the two routes to MI-VSD closure are different with devices or surgery, outcomes are about the same
Both appear better than tablets alone
8/
These mortality stats are >10x routine work
Some argue that a "trial of life" helps patients (too sick to stand any chance of recovery) avoid futile intervention during their final illness
UK surgery or catheter closure is most commonly seen in week 2, but has known hazards
9/
Some argue that a "trial of life" helps patients (too sick to stand any chance of recovery) avoid futile intervention during their final illness
UK surgery or catheter closure is most commonly seen in week 2, but has known hazards
9/
There are 3 things to work out
What to do
When to do it
& Who needs to know
The last is the most important
Everyone needs to accept the inevitable risks & the decision is made for you if they don't
Deciding what/when follows, with usual vagaries of MDTs lacking experience
10/
What to do
When to do it
& Who needs to know
The last is the most important
Everyone needs to accept the inevitable risks & the decision is made for you if they don't
Deciding what/when follows, with usual vagaries of MDTs lacking experience
10/
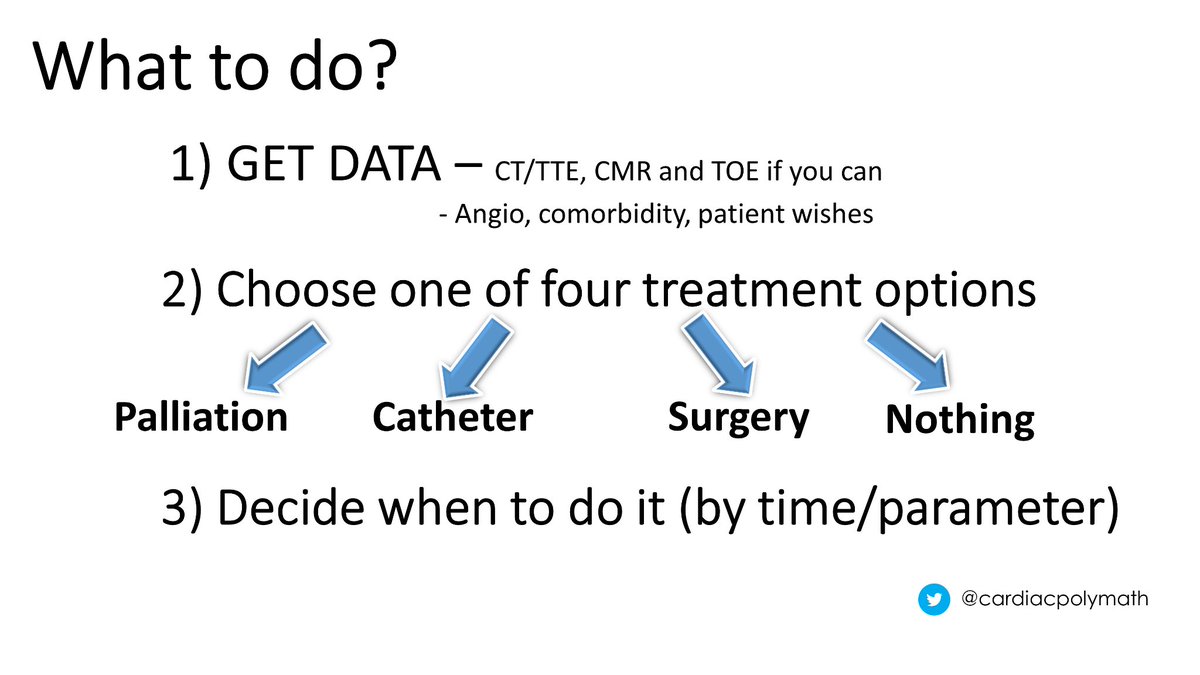
To get the best decision you need data, ideally as much as possible
But this is not complicated, there are only 4 possible outcomes
Palliative, surgical, catheter or wait
As patients are sick, it helps to define "red lines" that trigger reconsideration of timing/strategy
11/
But this is not complicated, there are only 4 possible outcomes
Palliative, surgical, catheter or wait
As patients are sick, it helps to define "red lines" that trigger reconsideration of timing/strategy
11/
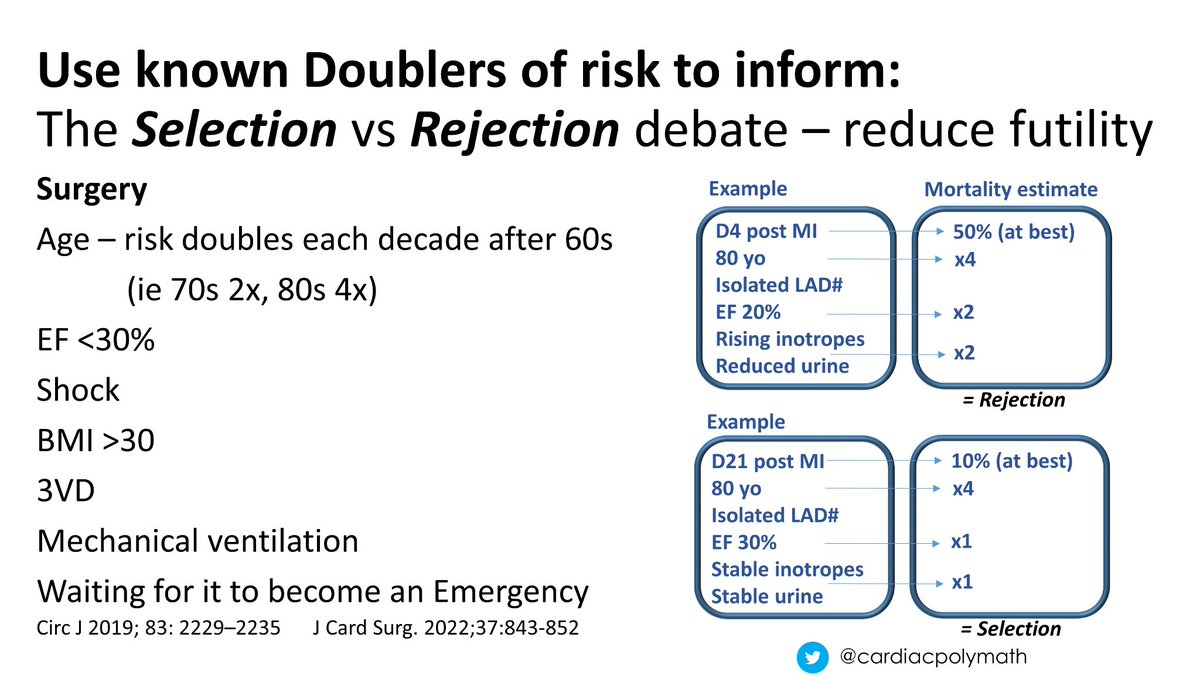
You need to make use of what is known
National surgical registry 🇬🇧&🇯🇵 identify factors that double adverse outcomes
In addition timing data ⬆️ sets a ballpark outcome for the event
You can only double a 50:50 risk so many times before it becomes a futile effort
12/
National surgical registry 🇬🇧&🇯🇵 identify factors that double adverse outcomes
In addition timing data ⬆️ sets a ballpark outcome for the event
You can only double a 50:50 risk so many times before it becomes a futile effort
12/
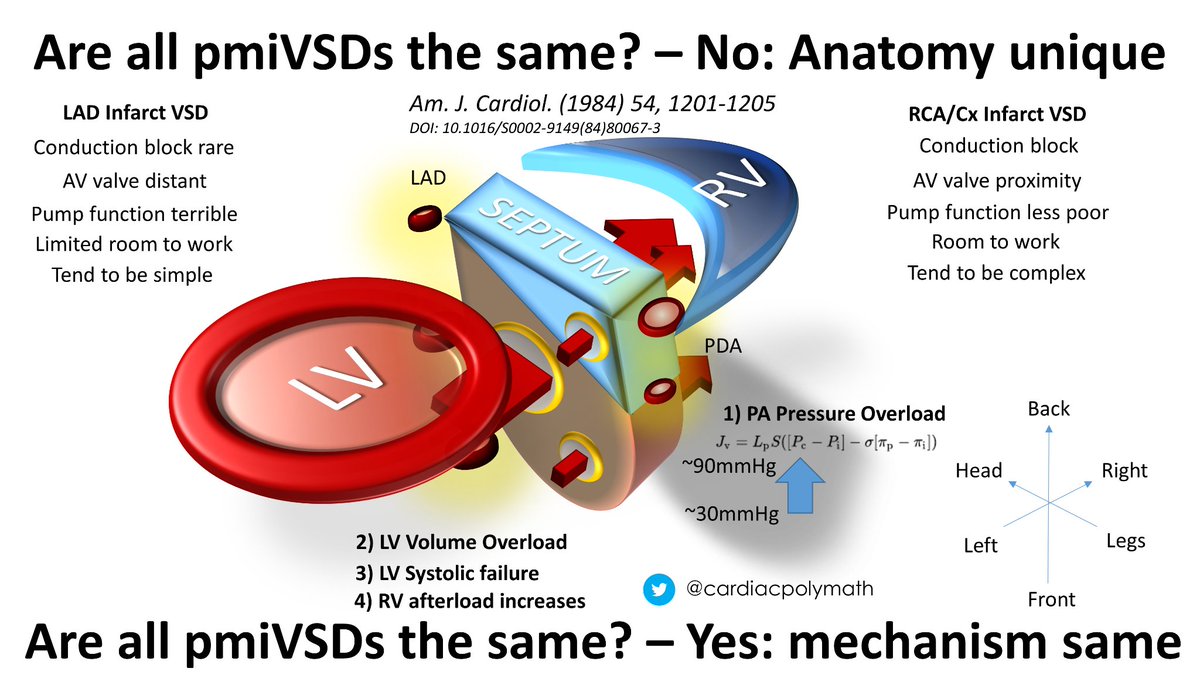
Patient anatomy is important - MI-VSDs are not the same
PDA occlusions (posterior 1/3 of basal septum) tend to be close to the AV valve sub-apparatus & complex entrance -> exit
LAD MI-VSD can run close to the apical myocardium or be too large for devices
LV impairment etc
13/
PDA occlusions (posterior 1/3 of basal septum) tend to be close to the AV valve sub-apparatus & complex entrance -> exit
LAD MI-VSD can run close to the apical myocardium or be too large for devices
LV impairment etc
13/
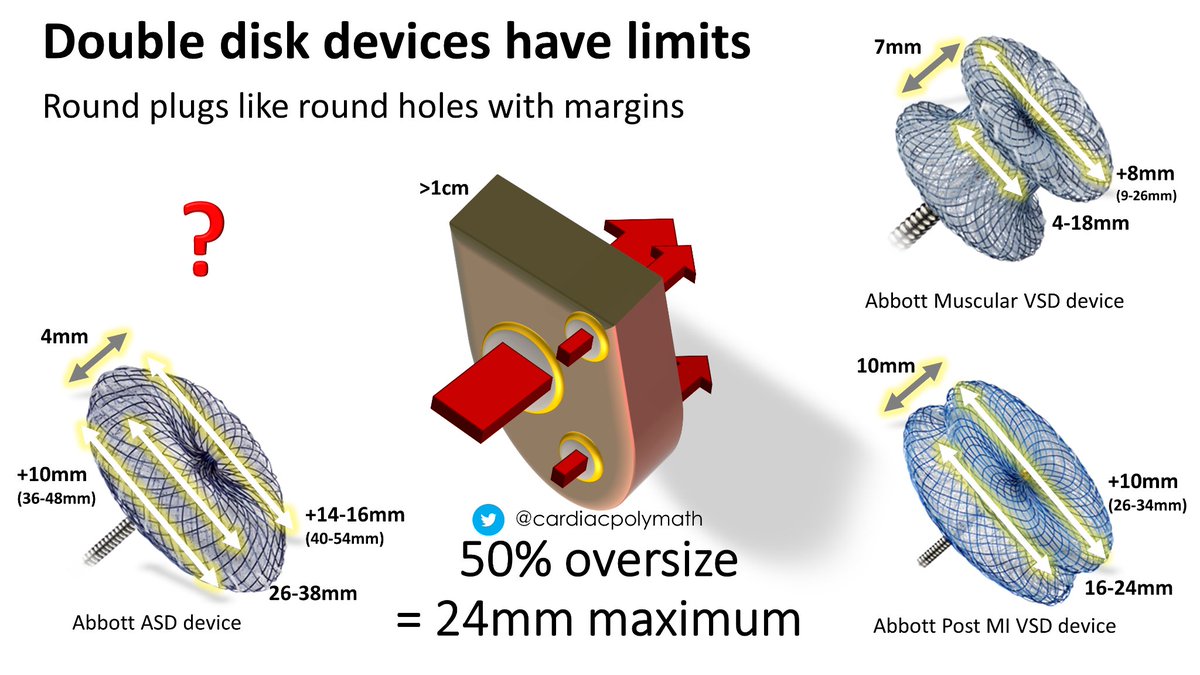
We use a standard array of double disc devices - they are ⭕ - & like ⭕ holes, with neat margins
There's a 50% oversize rule to sizing because tissue necrosis is often ongoing (even then the reintervention rate is >20%)
Sometimes MI-VSDs are too large or complex for plugs
14/
There's a 50% oversize rule to sizing because tissue necrosis is often ongoing (even then the reintervention rate is >20%)
Sometimes MI-VSDs are too large or complex for plugs
14/
What then?
Surgery or a hybrid approach like @AdamGreenbaumMD BASSINET to use devices anchored with sutures through the myocardium agnostic to the VSD tract
I have not seen/heard of many centers offering this, but the article interest continues to grow - so one to watch?
15/
Surgery or a hybrid approach like @AdamGreenbaumMD BASSINET to use devices anchored with sutures through the myocardium agnostic to the VSD tract
I have not seen/heard of many centers offering this, but the article interest continues to grow - so one to watch?
15/

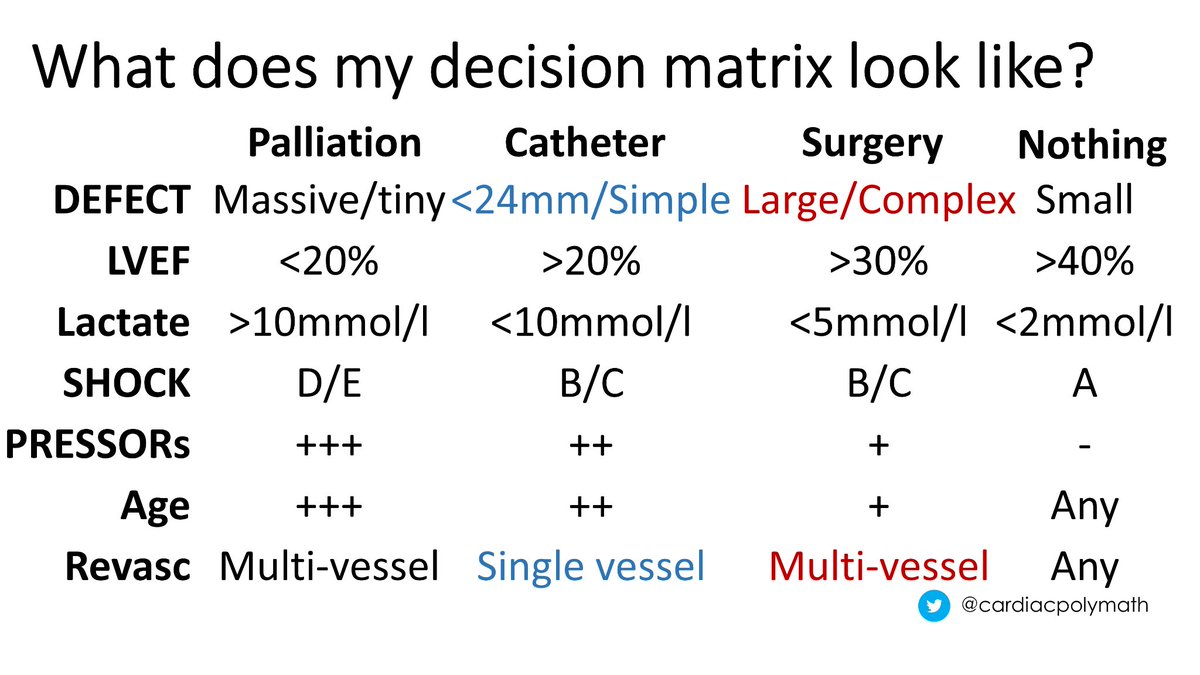
So putting all that together this is more-or-less how I think about this patient group
The extremes are easy to define
There will be some patients better served, but too sick for, surgery - they may/may not have a device option
Other patients may do better with a device
16/
The extremes are easy to define
There will be some patients better served, but too sick for, surgery - they may/may not have a device option
Other patients may do better with a device
16/
But this is just my opinion, & serious data is both lacking/unlikely to appear
The difficulty of waiting too long, or not waiting long enough combined with the low MI-VSD numbers in any centre makes trials hard, even if mortality halves with treatment
Device "HOW TO” follows⬇️
The difficulty of waiting too long, or not waiting long enough combined with the low MI-VSD numbers in any centre makes trials hard, even if mortality halves with treatment
Device "HOW TO” follows⬇️
The basic steps
Access
RCA infarcts do well with IVC/Aortic
LAD infarcts are better with SVC/Aortic
18/
Access
RCA infarcts do well with IVC/Aortic
LAD infarcts are better with SVC/Aortic
18/

Basic steps
Read the captions underneath the clip
19/
Read the captions underneath the clip
19/

Tips on MI-VSD ventriculography
20/
20/

Tips on AV rail formation
21/
21/

Tips on stiff wire insertion
Kissing catheter technique to minimise cheese-wiring
How deep to push the delivery catheter
Device navigation within the delivery system
& Deployment
22/
Kissing catheter technique to minimise cheese-wiring
How deep to push the delivery catheter
Device navigation within the delivery system
& Deployment
22/

One day I hoped to be able to fix these problems with material that restores contractility - for now that dream is on pause
END/
END/

Loading suggestions...