

💥Smith 𝘦𝘵 𝘢𝘭. reported draining a world record of 41 𝗹𝗶𝘁𝗿𝗲𝘀 of ascitic fluid in a single paracentesis session of a patient with decompensated cirrhosis.
How much Albumin would be needed in this case to prevent post paracentesis circulatory dysfunction ? 🧵 Read on👇
A 🧵 on important points to consider while performing Large Volume Paracentesis (LVP)
𝘏𝘰𝘸 𝘮𝘶𝘤𝘩 𝘢𝘭𝘣𝘶𝘮𝘪𝘯 𝘪𝘴 𝘵𝘰 𝘣𝘦 𝘪𝘯𝘧𝘶𝘴𝘦𝘥 𝘥𝘶𝘳𝘪𝘯𝘨 𝘱𝘦𝘳𝘧𝘰𝘳𝘮𝘪𝘯𝘨 𝘓𝘝𝘗❓️
𝘞𝘩𝘢𝘵 𝘪𝘴 𝘵𝘩𝘦 𝘮𝘢𝘹𝘪𝘮𝘶𝘮 𝘢𝘮𝘰𝘶𝘯𝘵 𝘰𝘧 𝘢𝘴𝘤𝘪𝘵𝘪𝘤 𝘧𝘭𝘶𝘪𝘥 𝘵𝘩𝘢𝘵 𝘤𝘢𝘯 𝘣𝘦 𝘥𝘳𝘢𝘪𝘯𝘦𝘥❓️
🛑Large Volume Paracentesis(LVP)
is arbitrarily defined as a paracentesis with >5 L of ascitic fluid drained.
In patients undergoing LVP, the use of albumin is crucial to prevent a further reduction of effective arterial blood volume, which may precipitate postparacentesis circulatory dysfunction (PPCD).
The clinical manifestations of PPCD include renal impairment, including HRS, dilutional hyponatremia, hepatic encephalopathy and death.
Albumin infusion is particularly important if more than 5 L of ascites are removed to prevent the development of PPCD.
Paracenteses of a smaller volume(<5L) are not associated with significant hemodynamic changes and albumin infusion may not be required.
Although there has not been a dose‐response study on albumin use with LVP, the administration of 6‐8 g of albumin per liter of ascites removed has been recommended.
💥For example, after the fifth liter, approximately 40 g of albumin should be infused, and after 8 L removal, the amount of albumin given should be approximately 64 g.
It has been held that there is no limit for the amount of ascites that can be removed in a single session, provided an appropriate amount of albumin is administered.
However, the risk of PPCD increases with >8 L of fluid evacuated in one single session.
A study showed that by limiting the LVP volume to <8 L per session and providing a higher than recommended dose of albumin (9.0 ± 2.5 g per liter of ascites removed), renal function and survival may be better preserved over a mean period of 2 years despite the development of PPCD in 40% of patients.
In patients with hemodynamic instability (systolic blood pressure <90 mm Hg), hyponatremia (serum sodium <130 mmol/L), and/or the presence of AKI, albumin infusion should be strongly considered for paracentesis of a smaller volume.
LVP is a safe procedure even in the presence of coagulopathy. In a study that included patients with an international normalized ratio of >1.5 and a platelet count of <50 × 109/L, only 1% of patients experienced minimal cutaneous bleeding after LVP.
Therefore, elevated prothrombin time or thrombocytopenia is not a contraindication for paracentesis, nor is transfusion of clotting factors or platelets recommended.
Possible exceptions may include patients with disseminated intravascular coagulation or uremia with thrombocytopenia.
1/3 👇 𝘾𝙤𝙣𝙩.
#MedTwitter #MedEd #MedX
How much Albumin would be needed in this case to prevent post paracentesis circulatory dysfunction ? 🧵 Read on👇
A 🧵 on important points to consider while performing Large Volume Paracentesis (LVP)
𝘏𝘰𝘸 𝘮𝘶𝘤𝘩 𝘢𝘭𝘣𝘶𝘮𝘪𝘯 𝘪𝘴 𝘵𝘰 𝘣𝘦 𝘪𝘯𝘧𝘶𝘴𝘦𝘥 𝘥𝘶𝘳𝘪𝘯𝘨 𝘱𝘦𝘳𝘧𝘰𝘳𝘮𝘪𝘯𝘨 𝘓𝘝𝘗❓️
𝘞𝘩𝘢𝘵 𝘪𝘴 𝘵𝘩𝘦 𝘮𝘢𝘹𝘪𝘮𝘶𝘮 𝘢𝘮𝘰𝘶𝘯𝘵 𝘰𝘧 𝘢𝘴𝘤𝘪𝘵𝘪𝘤 𝘧𝘭𝘶𝘪𝘥 𝘵𝘩𝘢𝘵 𝘤𝘢𝘯 𝘣𝘦 𝘥𝘳𝘢𝘪𝘯𝘦𝘥❓️
🛑Large Volume Paracentesis(LVP)
is arbitrarily defined as a paracentesis with >5 L of ascitic fluid drained.
In patients undergoing LVP, the use of albumin is crucial to prevent a further reduction of effective arterial blood volume, which may precipitate postparacentesis circulatory dysfunction (PPCD).
The clinical manifestations of PPCD include renal impairment, including HRS, dilutional hyponatremia, hepatic encephalopathy and death.
Albumin infusion is particularly important if more than 5 L of ascites are removed to prevent the development of PPCD.
Paracenteses of a smaller volume(<5L) are not associated with significant hemodynamic changes and albumin infusion may not be required.
Although there has not been a dose‐response study on albumin use with LVP, the administration of 6‐8 g of albumin per liter of ascites removed has been recommended.
💥For example, after the fifth liter, approximately 40 g of albumin should be infused, and after 8 L removal, the amount of albumin given should be approximately 64 g.
It has been held that there is no limit for the amount of ascites that can be removed in a single session, provided an appropriate amount of albumin is administered.
However, the risk of PPCD increases with >8 L of fluid evacuated in one single session.
A study showed that by limiting the LVP volume to <8 L per session and providing a higher than recommended dose of albumin (9.0 ± 2.5 g per liter of ascites removed), renal function and survival may be better preserved over a mean period of 2 years despite the development of PPCD in 40% of patients.
In patients with hemodynamic instability (systolic blood pressure <90 mm Hg), hyponatremia (serum sodium <130 mmol/L), and/or the presence of AKI, albumin infusion should be strongly considered for paracentesis of a smaller volume.
LVP is a safe procedure even in the presence of coagulopathy. In a study that included patients with an international normalized ratio of >1.5 and a platelet count of <50 × 109/L, only 1% of patients experienced minimal cutaneous bleeding after LVP.
Therefore, elevated prothrombin time or thrombocytopenia is not a contraindication for paracentesis, nor is transfusion of clotting factors or platelets recommended.
Possible exceptions may include patients with disseminated intravascular coagulation or uremia with thrombocytopenia.
1/3 👇 𝘾𝙤𝙣𝙩.
#MedTwitter #MedEd #MedX

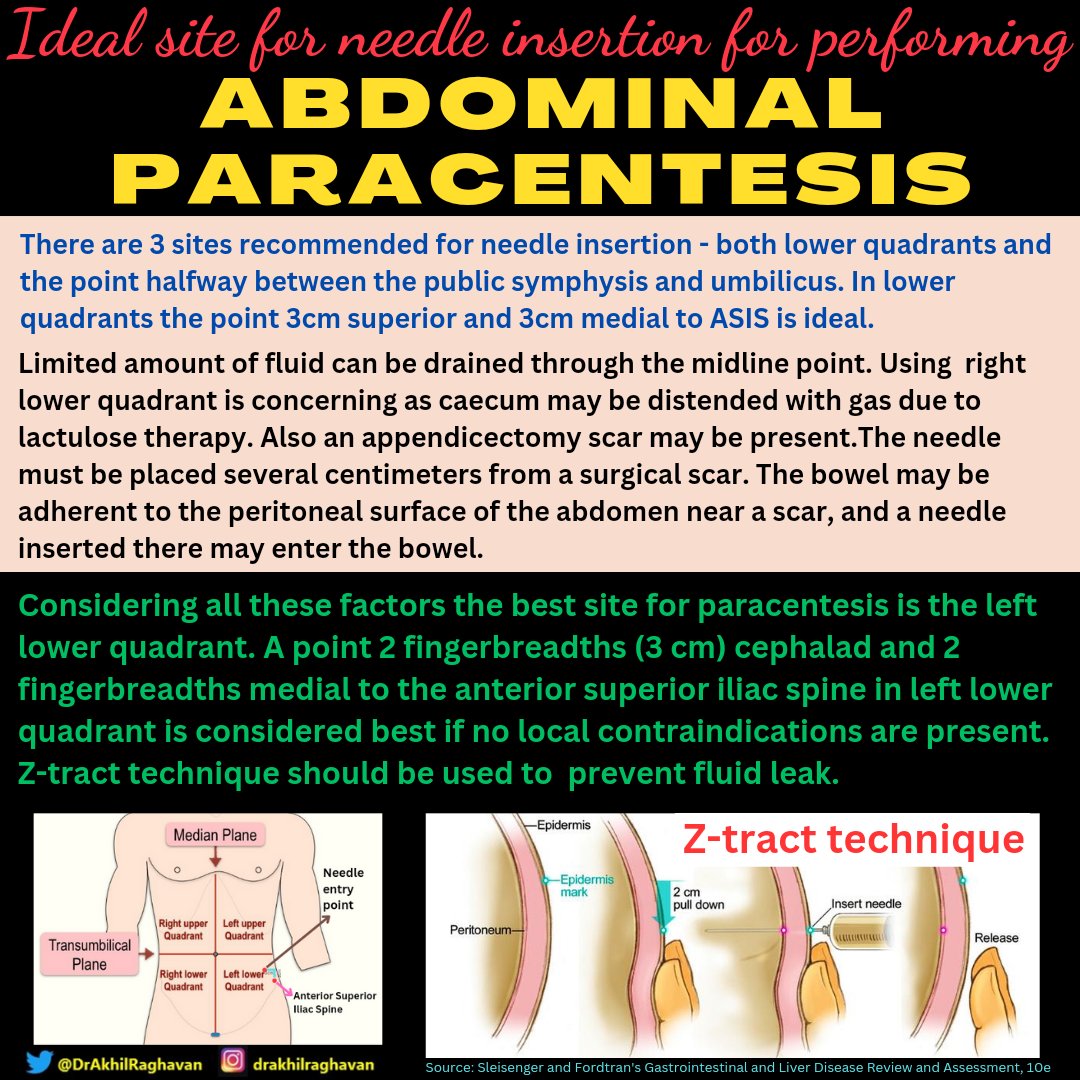
💥Ideal site for needle insertion in abdominal paracentesis
Large Volume Paracentesis 👇

Sources
1.Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and
Hepatorenal Syndrome: 2021 AASLD
journals.lww.com
2. Smith G, Barnard G. Massive volume paracentesis (up to 41 liters) for the outpatient management of ascites. J Clin Gastroenterol 1997; 25:402-3.
3. Sleisenger and Fordtran's Gastrointestinal and Liver Disease Review and Assessment 10th Edition
1.Diagnosis, Evaluation, and Management of Ascites, Spontaneous Bacterial Peritonitis and
Hepatorenal Syndrome: 2021 AASLD
journals.lww.com
2. Smith G, Barnard G. Massive volume paracentesis (up to 41 liters) for the outpatient management of ascites. J Clin Gastroenterol 1997; 25:402-3.
3. Sleisenger and Fordtran's Gastrointestinal and Liver Disease Review and Assessment 10th Edition
Loading suggestions...