

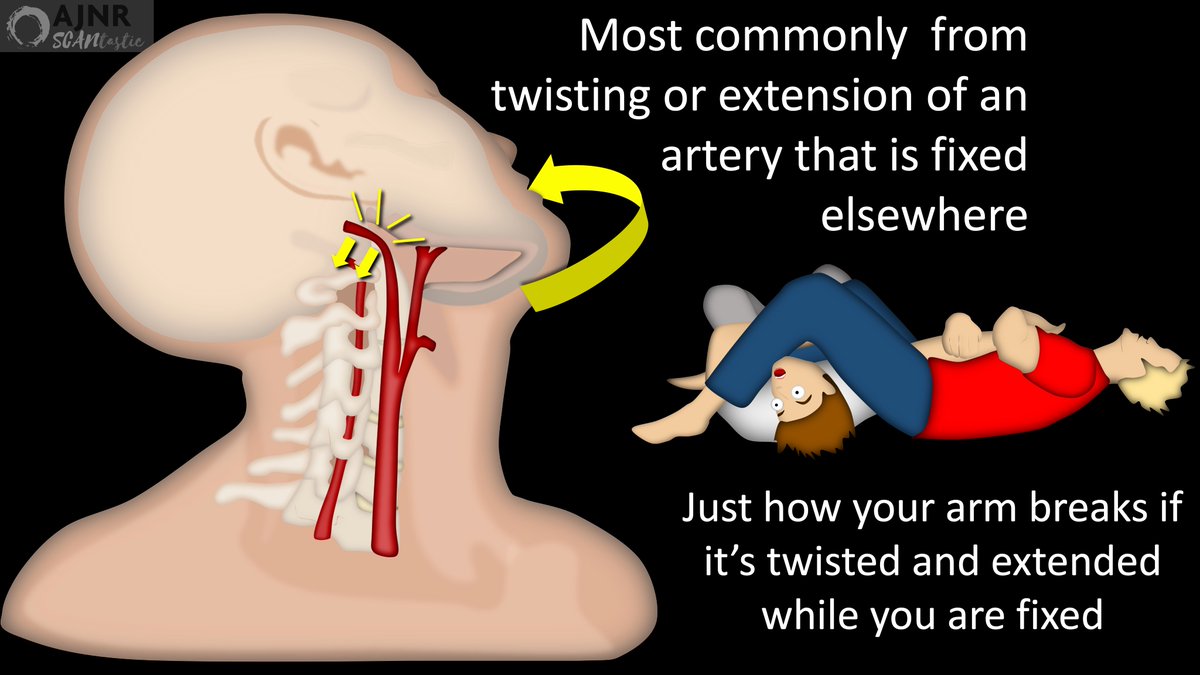
2/Vessel injury can be from direct penetration, but most commonly is from head/neck movement during trauma causing vessel stretching/twisting while the rest of the vessel is fixed.
Just like how your arm breaks if it’s twisted or pulled while the rest of you is fixed!
Just like how your arm breaks if it’s twisted or pulled while the rest of you is fixed!
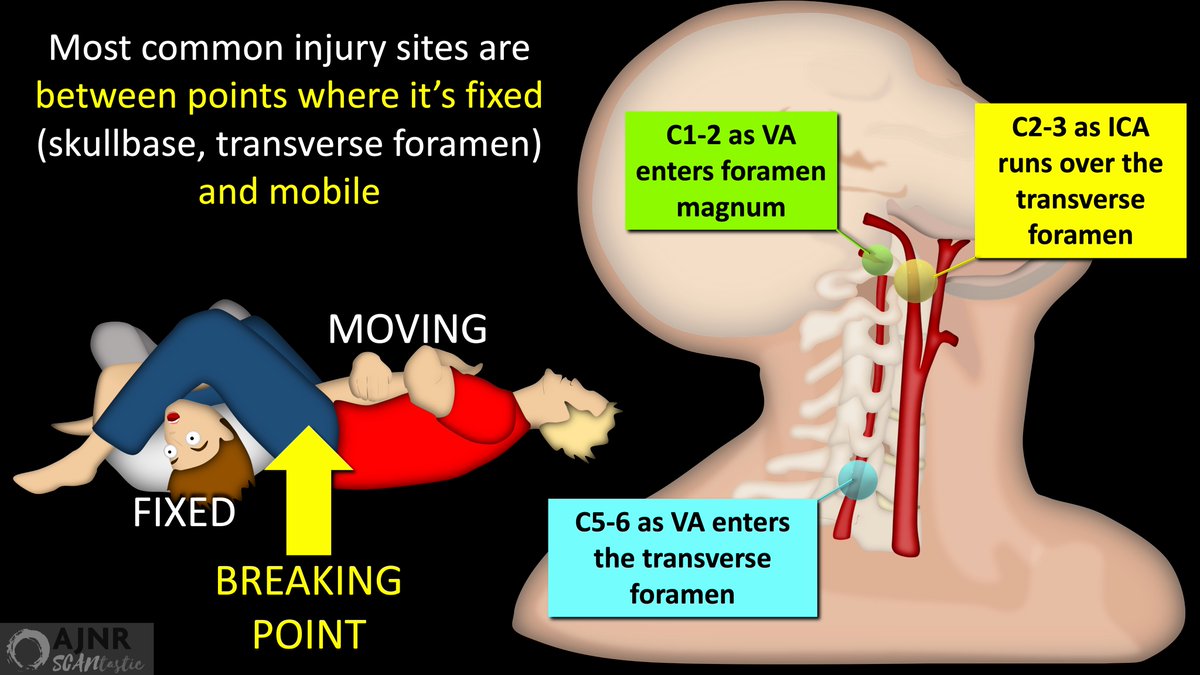
3/As a result, the most common sites of injury occur at a junction between where the vessel is mobile & where it is fixed (skullbase, transverse foramen).
At C2-3, the carotid runs over the transverse foramen of C2, essentially fixing it at this point as well.
At C2-3, the carotid runs over the transverse foramen of C2, essentially fixing it at this point as well.
4/We used to think blunt cerebrovascular injury (BCVI) was uncommon (<1%).
But that's because we only looked for it after the patient became symptomatic, typically after a stroke had occurred.
But that's because we only looked for it after the patient became symptomatic, typically after a stroke had occurred.
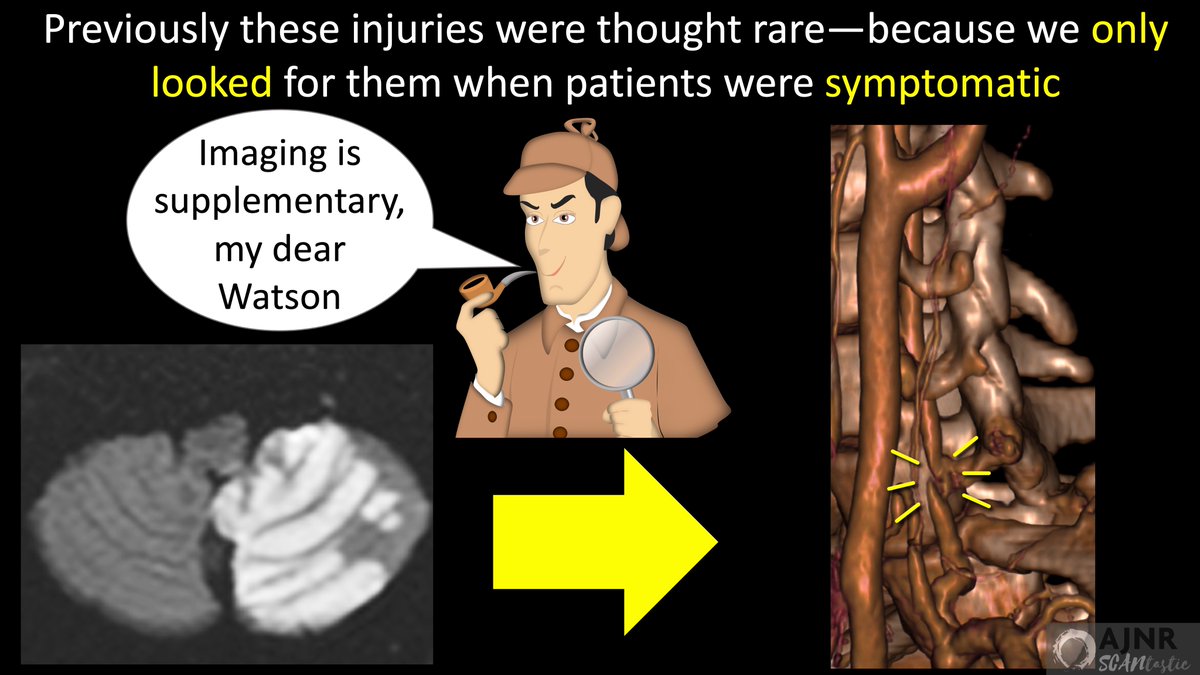
5/But as we started screening, we found it’s much more common, ranging from 2-10%, depending on population.
It just shows that any pathology can appear rare–because you won’t see it if you are not looking for it!
It just shows that any pathology can appear rare–because you won’t see it if you are not looking for it!
6/Screening is important b/c if BCVI is caught early, strokes can be prevented
But if it’s missed, mortality rates from the infarcts range from 25-40%.
It’s like your kids—PREVENTING a tantrum is huge, bc once a tantrum starts, it is difficult to control & has high morbidity!!
But if it’s missed, mortality rates from the infarcts range from 25-40%.
It’s like your kids—PREVENTING a tantrum is huge, bc once a tantrum starts, it is difficult to control & has high morbidity!!
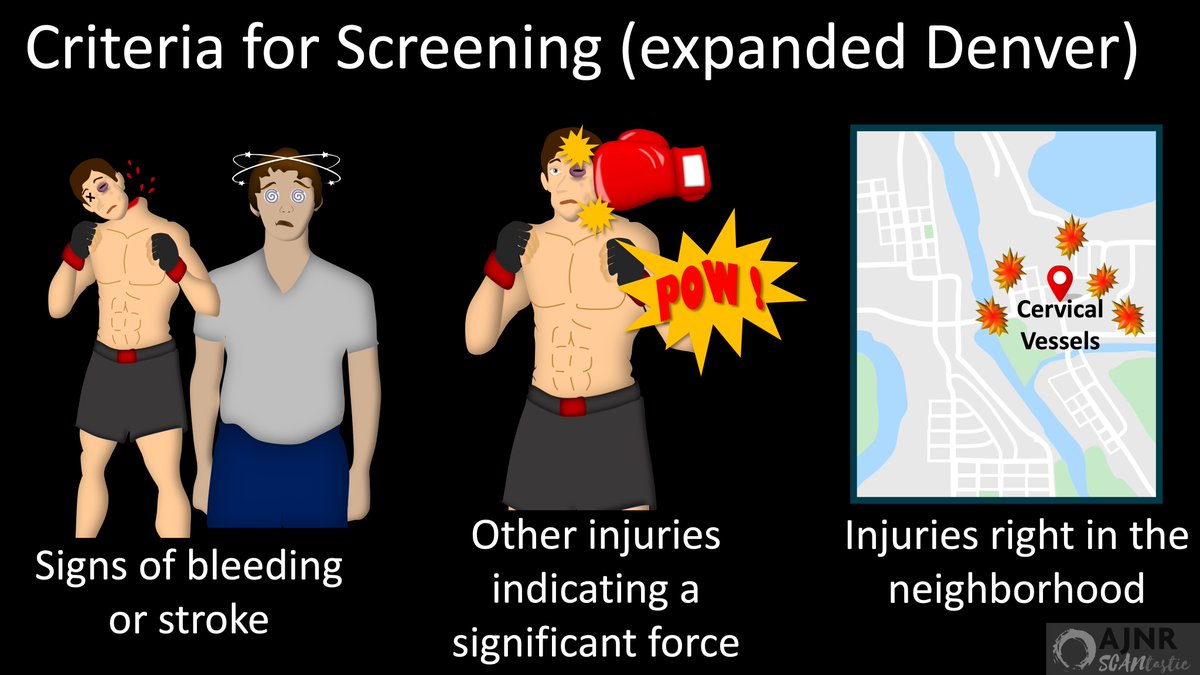
7/Expanded Denver criteria suggest who to screen. List is LONG, but can be grouped into the following categories:
(1) Clinical signs of bleeding/stroke
(2) Other injuries indicating significant force (ie LeFort fx)
(3) Injuries in the neighborhood (Cspine fx, seat belt sign)
(1) Clinical signs of bleeding/stroke
(2) Other injuries indicating significant force (ie LeFort fx)
(3) Injuries in the neighborhood (Cspine fx, seat belt sign)
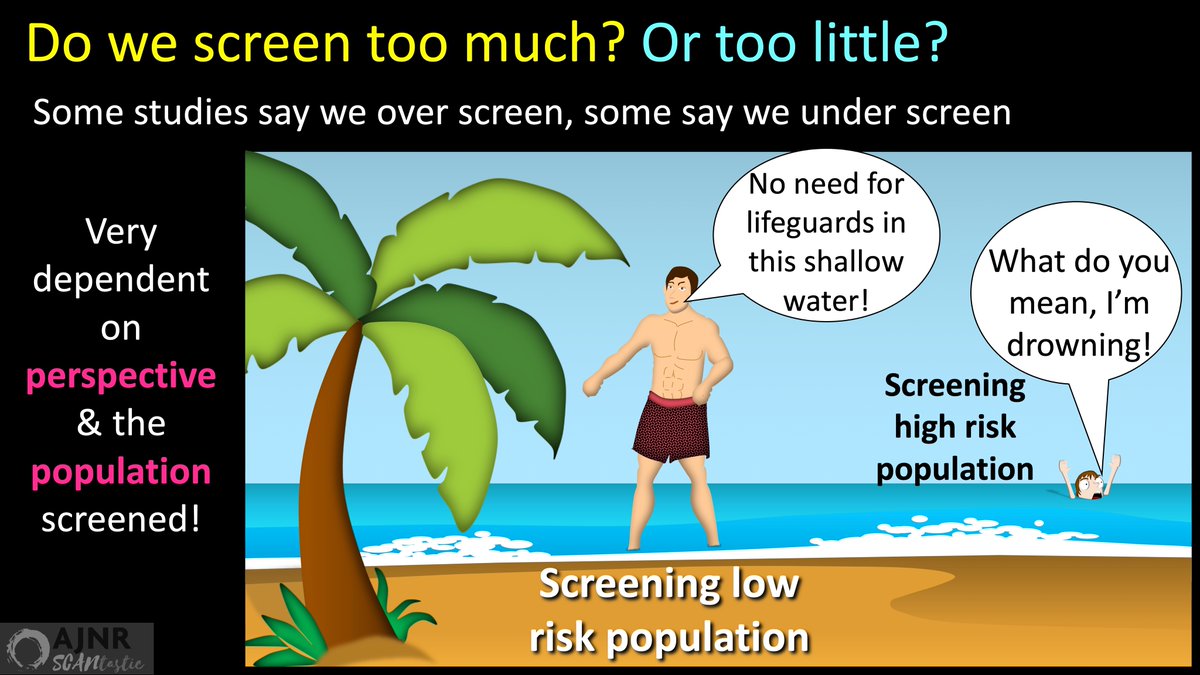
8/Some studies show the Denver criteria result in over screening & some show under screening
This just shows that the results depend heavily on the population you are screening.
Just like whether you think the ocean is deep depends on where you stand in it.
This just shows that the results depend heavily on the population you are screening.
Just like whether you think the ocean is deep depends on where you stand in it.
9/Setting thresholds for screening is like setting speed limits
You want to set them low enough so everyone is safe—car accidents have lots of morbidity
But you don’t want them too low that you end up capturing people not in danger & causing traffic jams & unnecessary citations
You want to set them low enough so everyone is safe—car accidents have lots of morbidity
But you don’t want them too low that you end up capturing people not in danger & causing traffic jams & unnecessary citations
10/In this month's @theAJNR, Hiatt et al. looked at trauma pts screened w/CTA for BCVI
They looked at what would have happened if they had NOT scanned:
-Pts not meeting expanded Denver
-& low risk mechanisms
Few BCVI would be missed & many unneeded scans could be avoided
They looked at what would have happened if they had NOT scanned:
-Pts not meeting expanded Denver
-& low risk mechanisms
Few BCVI would be missed & many unneeded scans could be avoided

11/But this only tells us about the population they screened.
No one knows what may have been missed in pts who didn’t get CTA.
Remember–you don’t know what you miss in those you don’t image!
This is especially true in BCVI, where if we look harder, we find more
No one knows what may have been missed in pts who didn’t get CTA.
Remember–you don’t know what you miss in those you don’t image!
This is especially true in BCVI, where if we look harder, we find more
12/What to do?
Being too selective in screening where a miss causes severe morbidity is like being stingy w/anesthesia
Both have risks & costs & require extra labor
But the overwhelming benefit means you should always generously err on the side of too much use than too little!
Being too selective in screening where a miss causes severe morbidity is like being stingy w/anesthesia
Both have risks & costs & require extra labor
But the overwhelming benefit means you should always generously err on the side of too much use than too little!
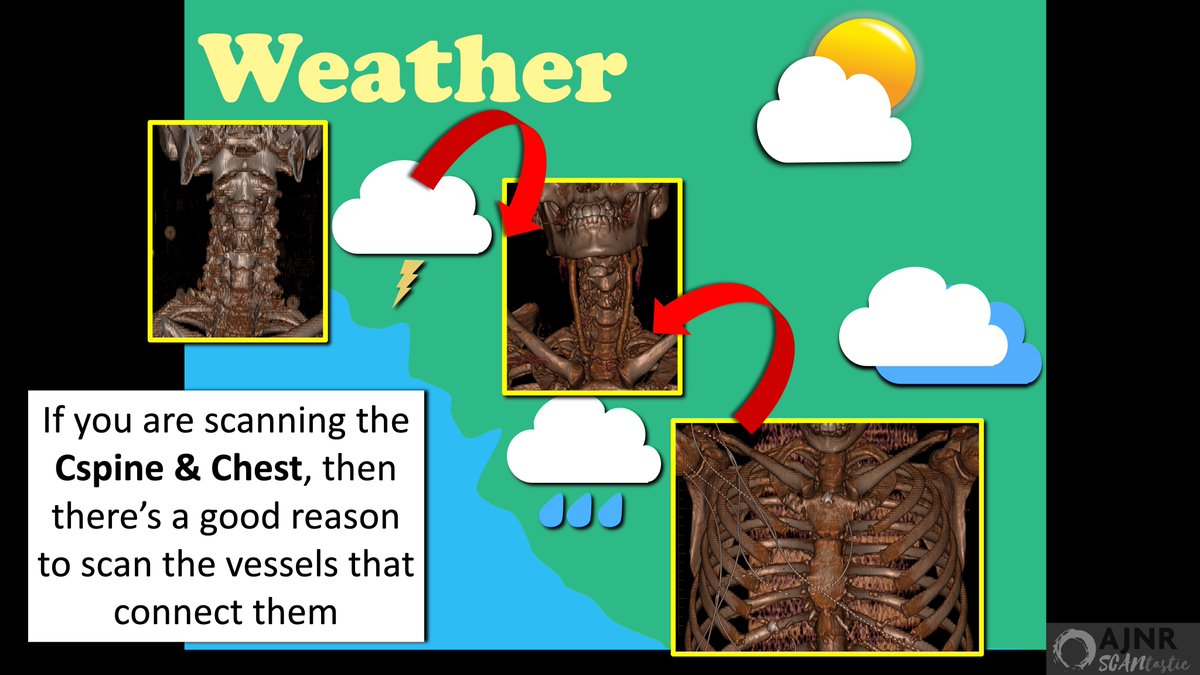
13/A recent study suggested extending screening to all who get a CT Cspine & CT chest
It’s like the weather
If you're standing on a piece of land connecting two regions both expected to get rain, you should probably have an umbrella
(Harper, Trauma Surg Acute Care Open. 2022)
It’s like the weather
If you're standing on a piece of land connecting two regions both expected to get rain, you should probably have an umbrella
(Harper, Trauma Surg Acute Care Open. 2022)

14/Similarly, if you are concerned for possible injury to the Cspine or Chest then you should probably be concerned about injury to the vessels connecting the 2!
This screening protocol resulted in a 5x increase in BCVI detected compared to the period before the protocol.
This screening protocol resulted in a 5x increase in BCVI detected compared to the period before the protocol.

Loading suggestions...