

1/7
I sent a poll an hour ago:
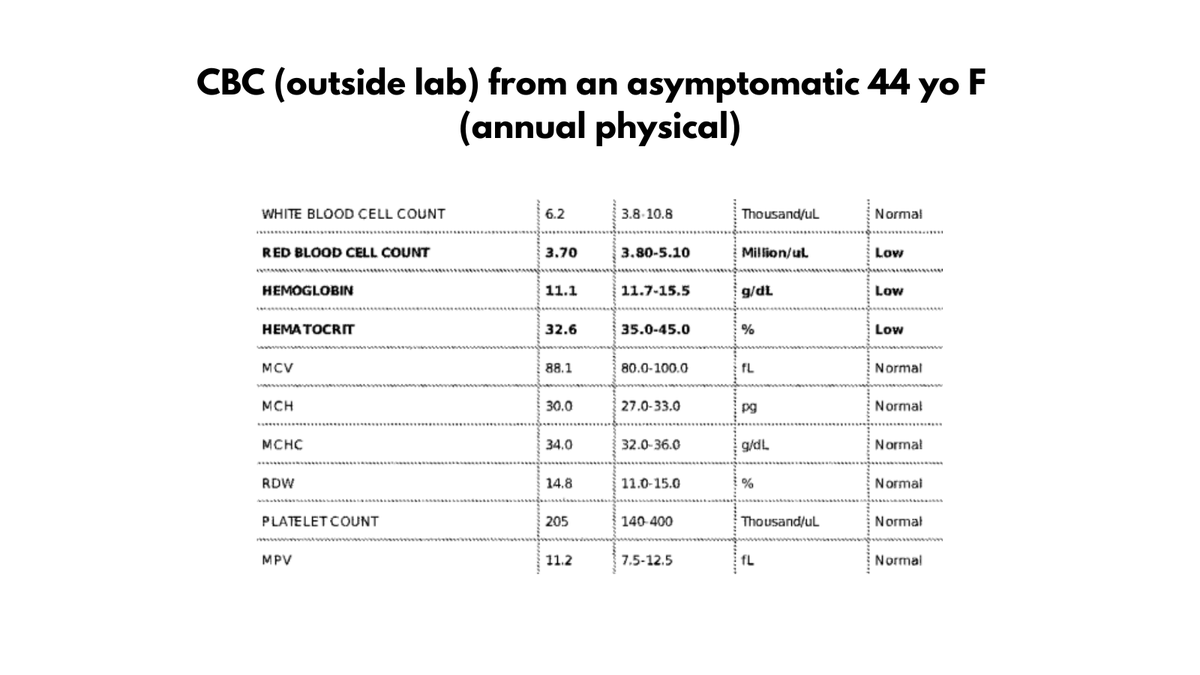
You see a young F patient with incidental finding of normocytic anemia. You get JUST ONE test 😉 to make the diagnosis. What would you choose?
CRP
TSH
Retic count
Ferritin
... already over 370 votes, with retic count and ferritin tied for 1st!
I sent a poll an hour ago:
You see a young F patient with incidental finding of normocytic anemia. You get JUST ONE test 😉 to make the diagnosis. What would you choose?
CRP
TSH
Retic count
Ferritin
... already over 370 votes, with retic count and ferritin tied for 1st!
2/7
CRP 5.5%
TSH 16.5%
Retic count 39.6%
Ferritin 38.6%
This is obviously an artificial situation. I gave no history (though I mentioned the patient was female, young and asymptomatic ["incidental finding"]), and asked you to choose just one lab.
CRP 5.5%
TSH 16.5%
Retic count 39.6%
Ferritin 38.6%
This is obviously an artificial situation. I gave no history (though I mentioned the patient was female, young and asymptomatic ["incidental finding"]), and asked you to choose just one lab.
3/7
There is no right answer. If you were a betting person, you might choose ferritin since the prevalence of iron deficiency anemia in F adults of reproductive age is 5% in the US and up tp 30% are normocytic. Thus, the pretest probability of IDA in this case is unrivaled.
There is no right answer. If you were a betting person, you might choose ferritin since the prevalence of iron deficiency anemia in F adults of reproductive age is 5% in the US and up tp 30% are normocytic. Thus, the pretest probability of IDA in this case is unrivaled.
4/7
But if you were a methodical, algorithm-minded physician, your first impulse might be to check the reticulocyte count, which is the traditional first branch point in the work up of normocytic anemia.
But if you were a methodical, algorithm-minded physician, your first impulse might be to check the reticulocyte count, which is the traditional first branch point in the work up of normocytic anemia.

5/7
What are the chances of it being elevated? Well, she's asymptomatic so unlikely to be an acute bleed. That leaves hemolysis, which is also pretty uncommon in an asymptomatic woman of this age.
What are the chances of it being elevated? Well, she's asymptomatic so unlikely to be an acute bleed. That leaves hemolysis, which is also pretty uncommon in an asymptomatic woman of this age.
6/7
As it turns out, I saw this case yesterday and her PCP had in fact checked her retic count. It was elevated. Her haptoglobin was undetectable and her LDH/bilirubin elevated.
Past CBCs was normal, and DAT is pending. But, the database is most c/w AIHA.
As it turns out, I saw this case yesterday and her PCP had in fact checked her retic count. It was elevated. Her haptoglobin was undetectable and her LDH/bilirubin elevated.
Past CBCs was normal, and DAT is pending. But, the database is most c/w AIHA.
7/7
The important message here is:
DO NOT FORGET TO CHECK THE RETIC COUNT IN YOUR ANEMIC PATIENT!!
The important message here is:
DO NOT FORGET TO CHECK THE RETIC COUNT IN YOUR ANEMIC PATIENT!!
Loading suggestions...