

#msk #musculoskeletal #Radiology #MSK #orthopedics #orthotwitter
Here a case of lower extremity pain
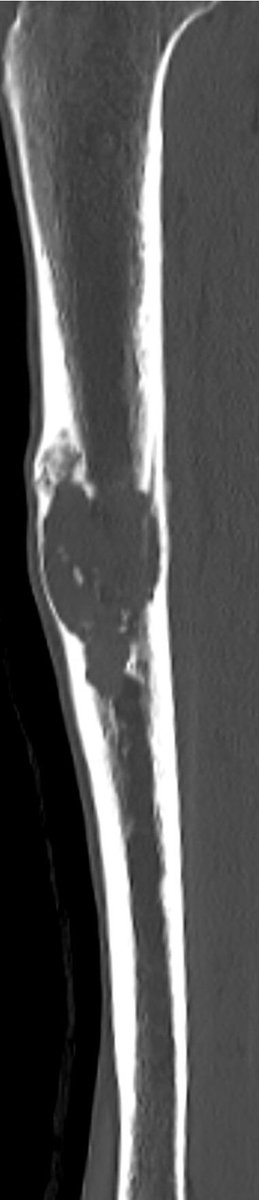
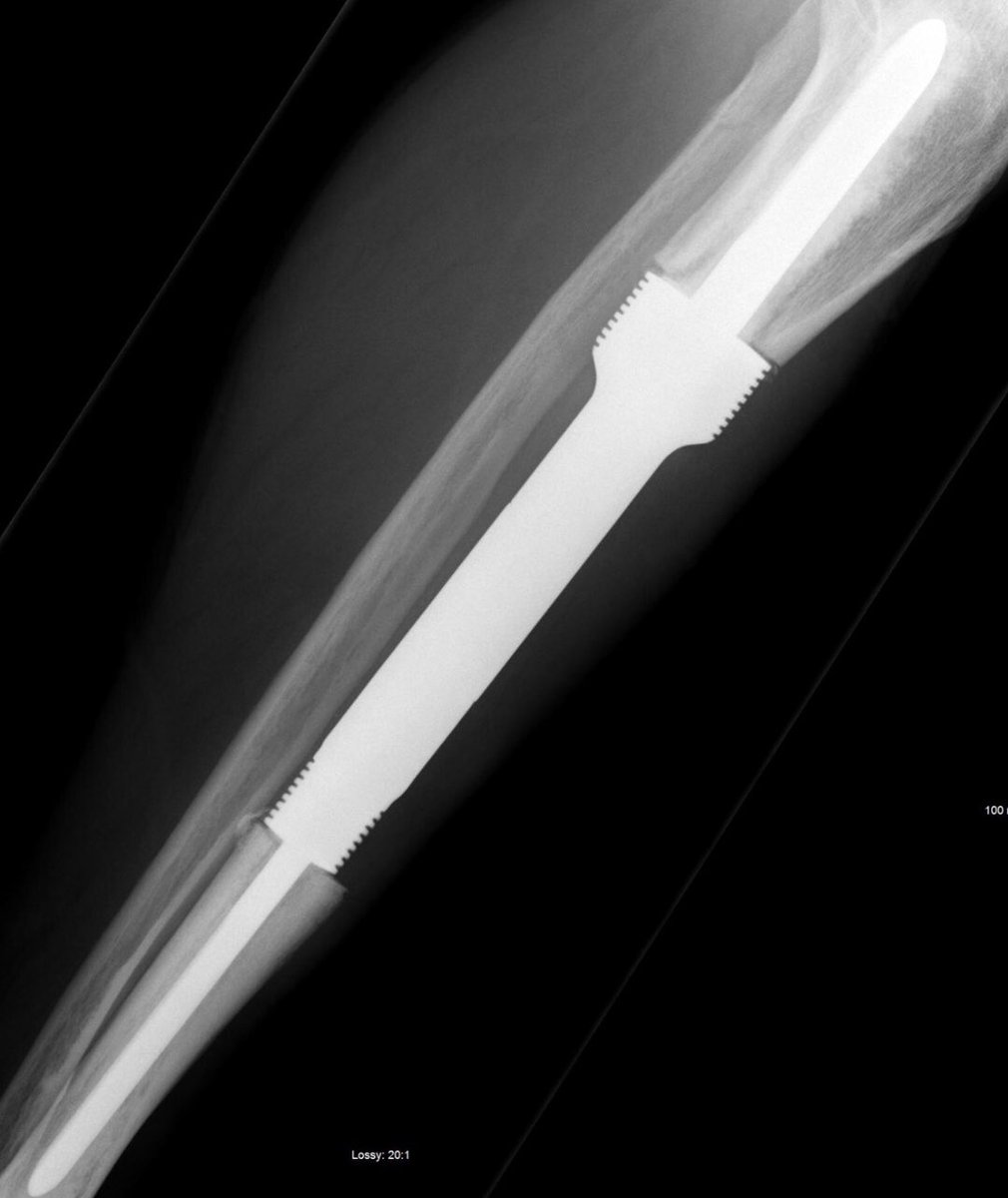
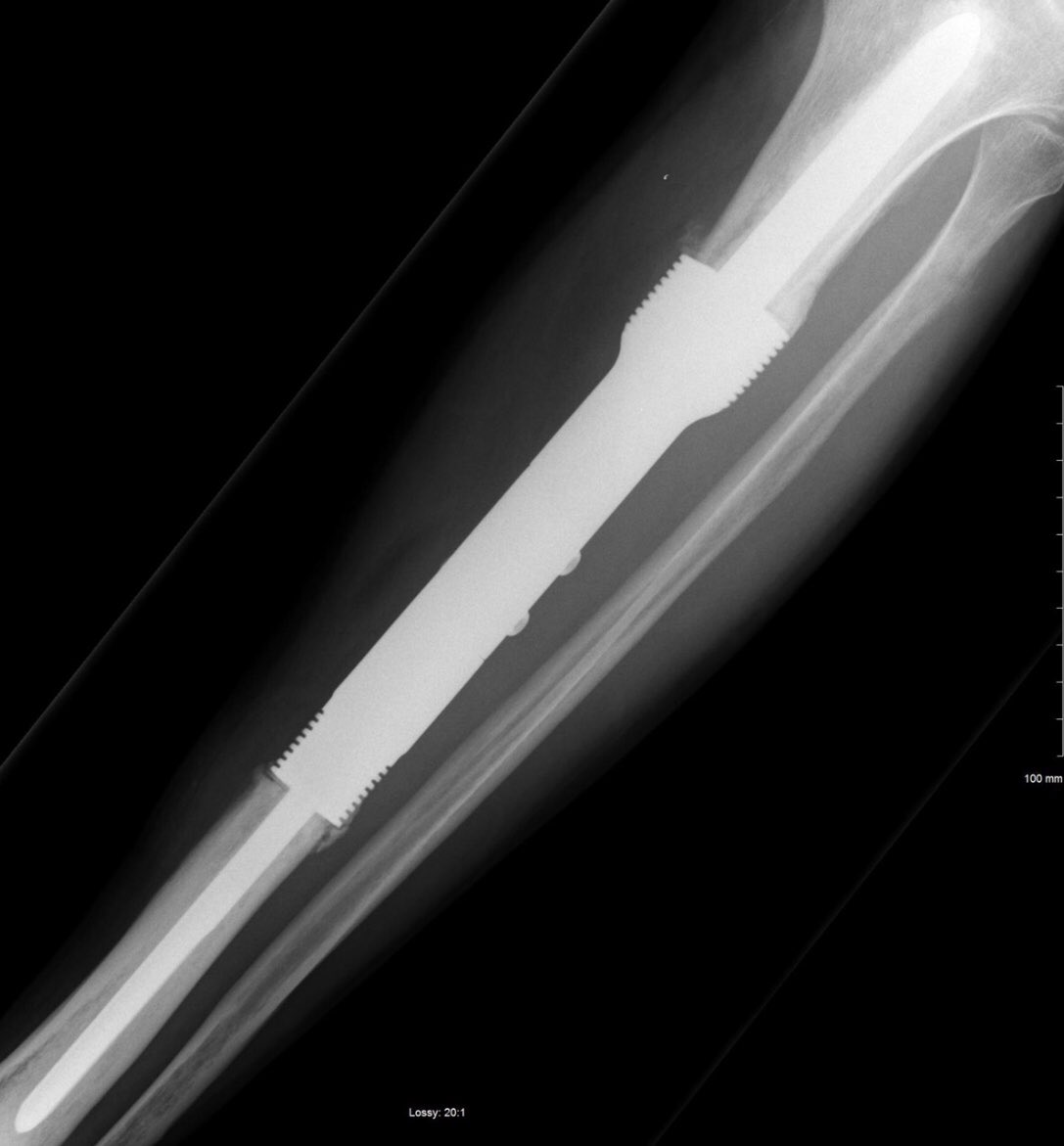
X ray of the tibia
Here a case of lower extremity pain
X ray of the tibia



The case is Adamantinoma
(AD) is a very rare, low-grade malignant neoplasm, accounting for <1% primary malignant bone tumours. It shows epithelial differentiation and occurs almost exclusively in the tibia (80-90% of cases) and fibula (ipsilateral fibular involvement in 10%
(AD) is a very rare, low-grade malignant neoplasm, accounting for <1% primary malignant bone tumours. It shows epithelial differentiation and occurs almost exclusively in the tibia (80-90% of cases) and fibula (ipsilateral fibular involvement in 10%
Initially described by Fischer et al in 1913, this lesion was named adamantinoma because of histological similarity to adamantinoma of the jaw (now called odontogenic ameloblastoma).
It is essentially a biphasic tumour with diverse histological patterns. In its classical form, AD tends to occur in the 3rd – 4th decade of life, with a wide age range (3-86 years).
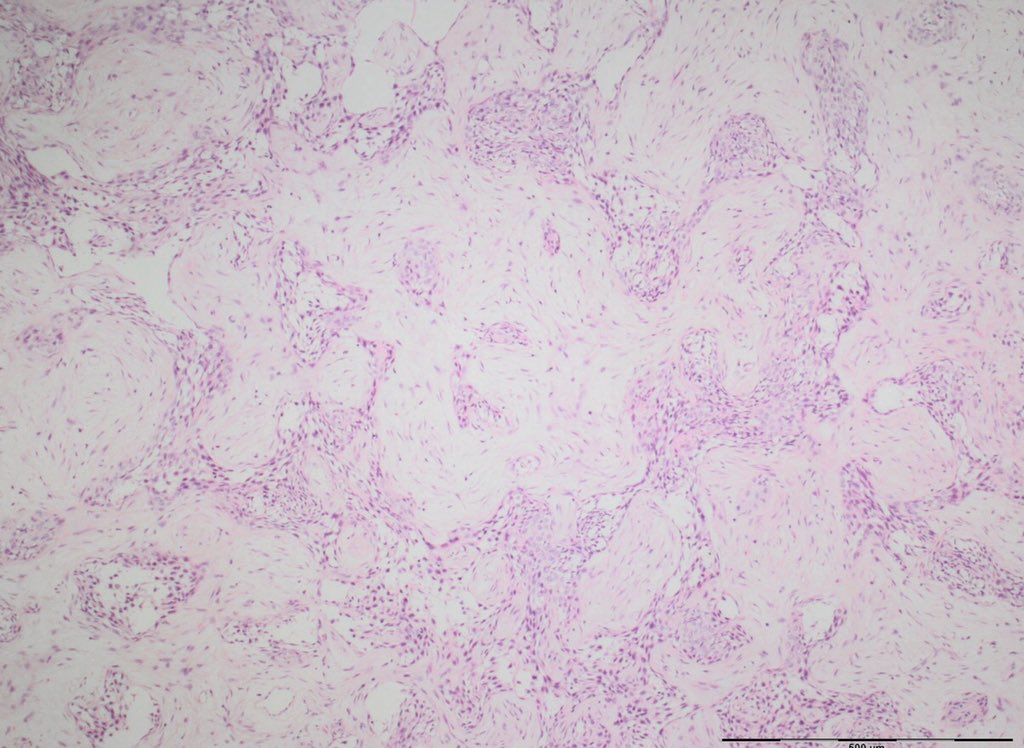
A subset of adamantinomas involves predominantly tibial cortex and contains areas resembling osteofibrous dysplasia (see case 60), within which are small nests of epithelial cells.
Tumours in this subset are classified by the majority of bone pathologists as osteofibrous dysplasia-like adamantinoma (OFD-LA, see case 62). The relationship of classic AD to osteofibrous dysplasia (OFD)
, a rare benign tumour that is typically found in the same bones, is controversial and has been the subject of speculation amongst bone tumour specialists for some time.
AD presents as tibial swelling/deformity, with or without pain. The history is usually long. There is frequently a history of trauma (60% of subjects in one large series had had a previous significant traumatic episode).
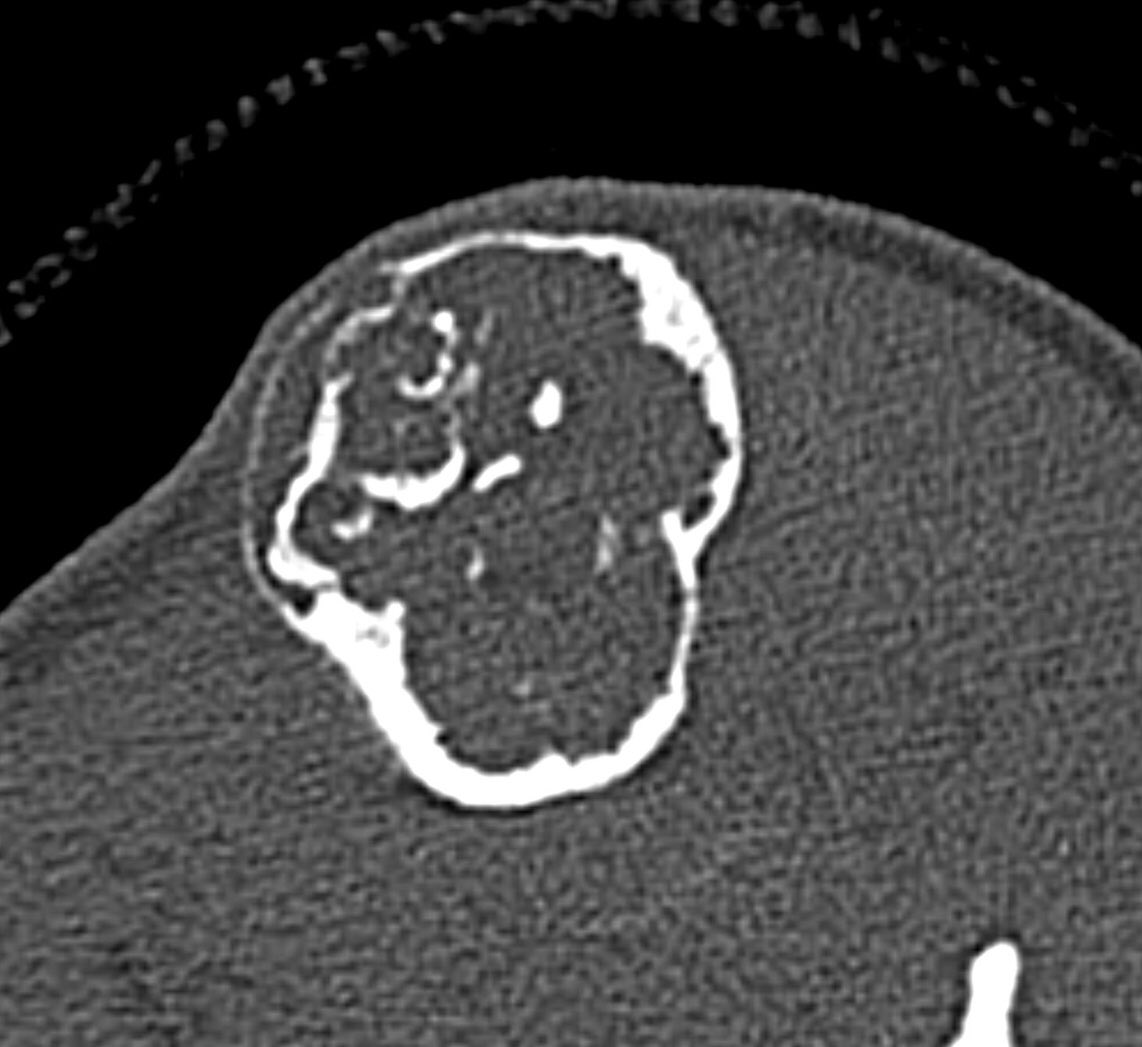
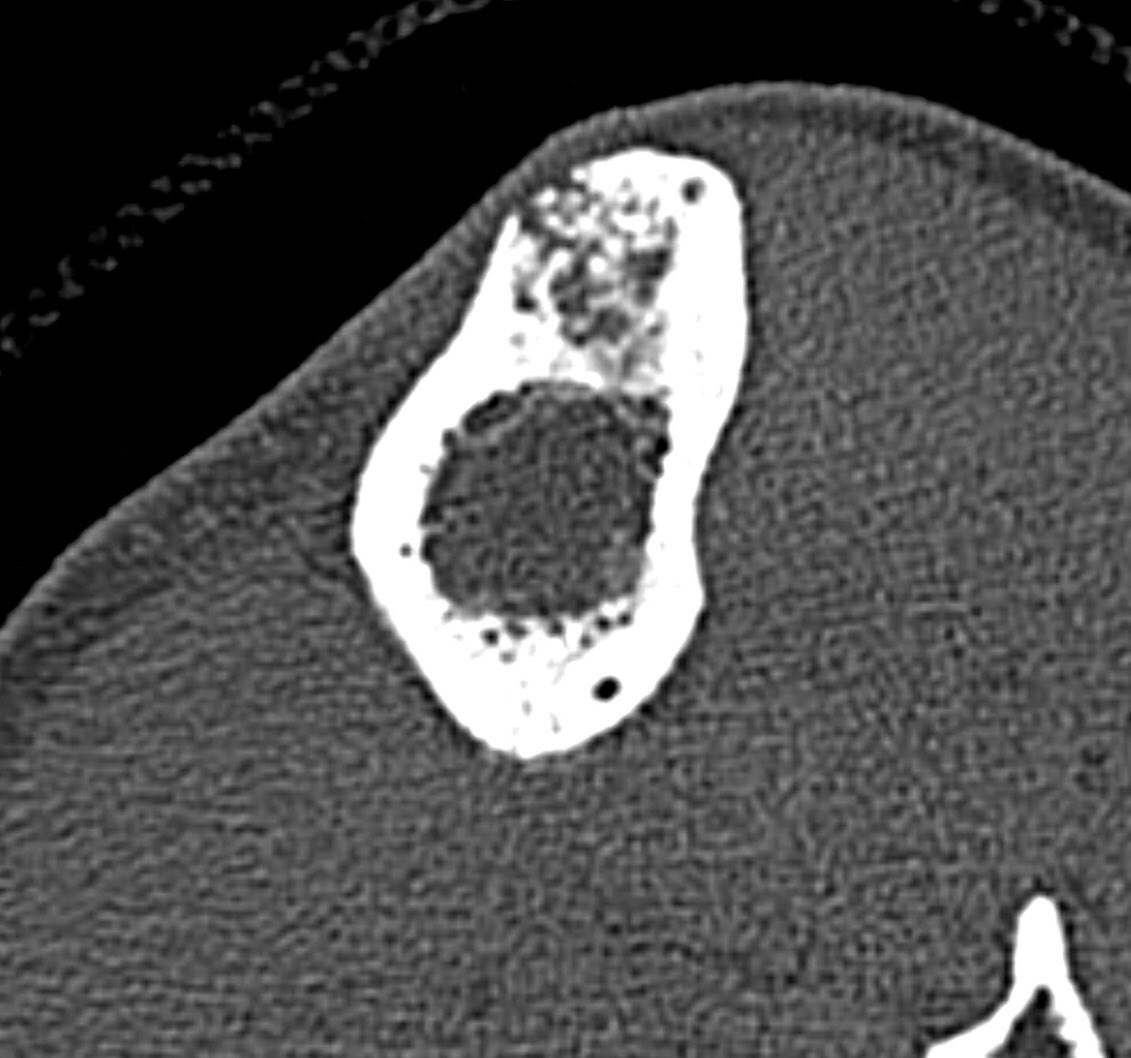
A single destructive lesion or multifocal tumour,may be identified, affecting cortex and often extending to the medulla,most commonly in the mid-tibial shaft.The lesion is typically eccentric and may cause mild bone expansion,endosteal scalloping and eventually destroy the cortex
AD typically appears multilocular and trabeculated, with intervening and surrounding sclerosis. A distinct periosteal reaction is unusual. An extra-osseous mass and pathological fracture may be seen
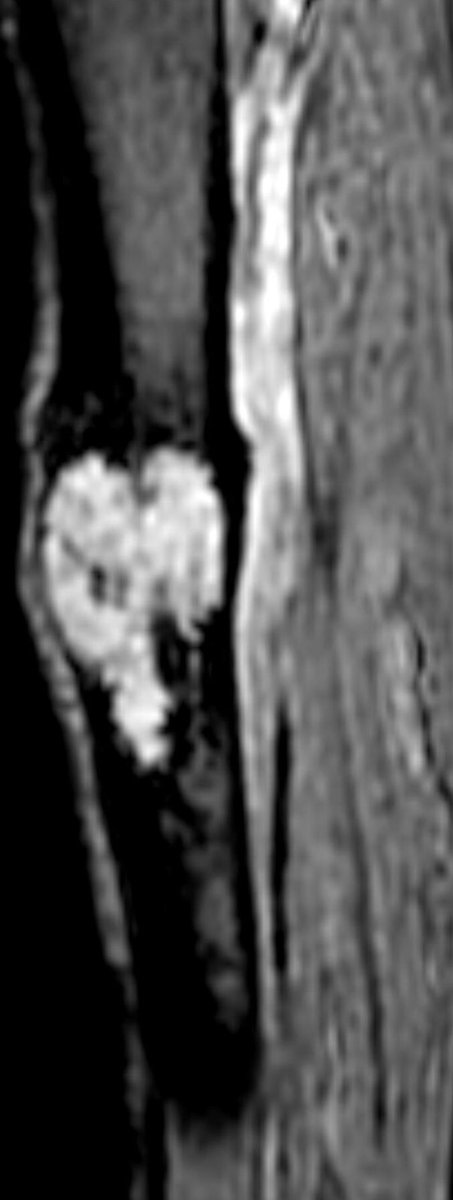
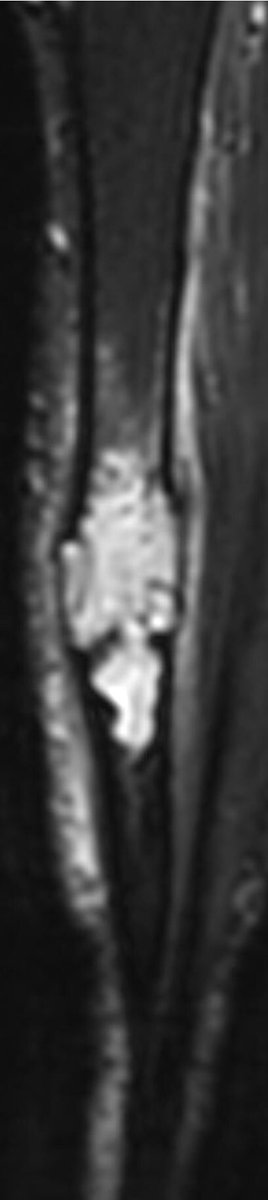
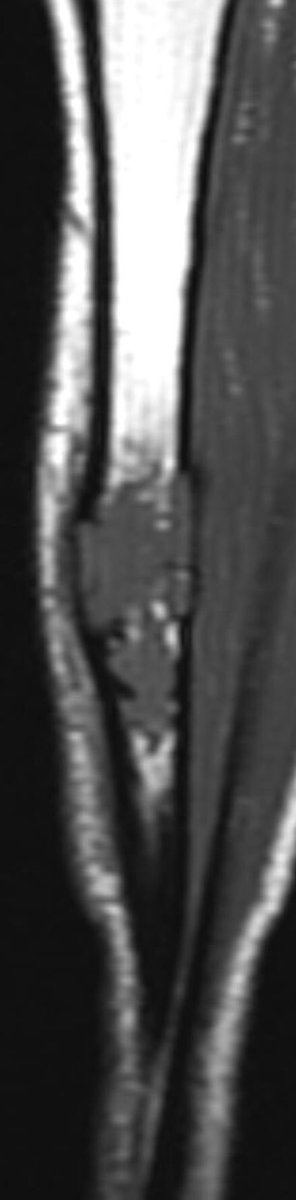
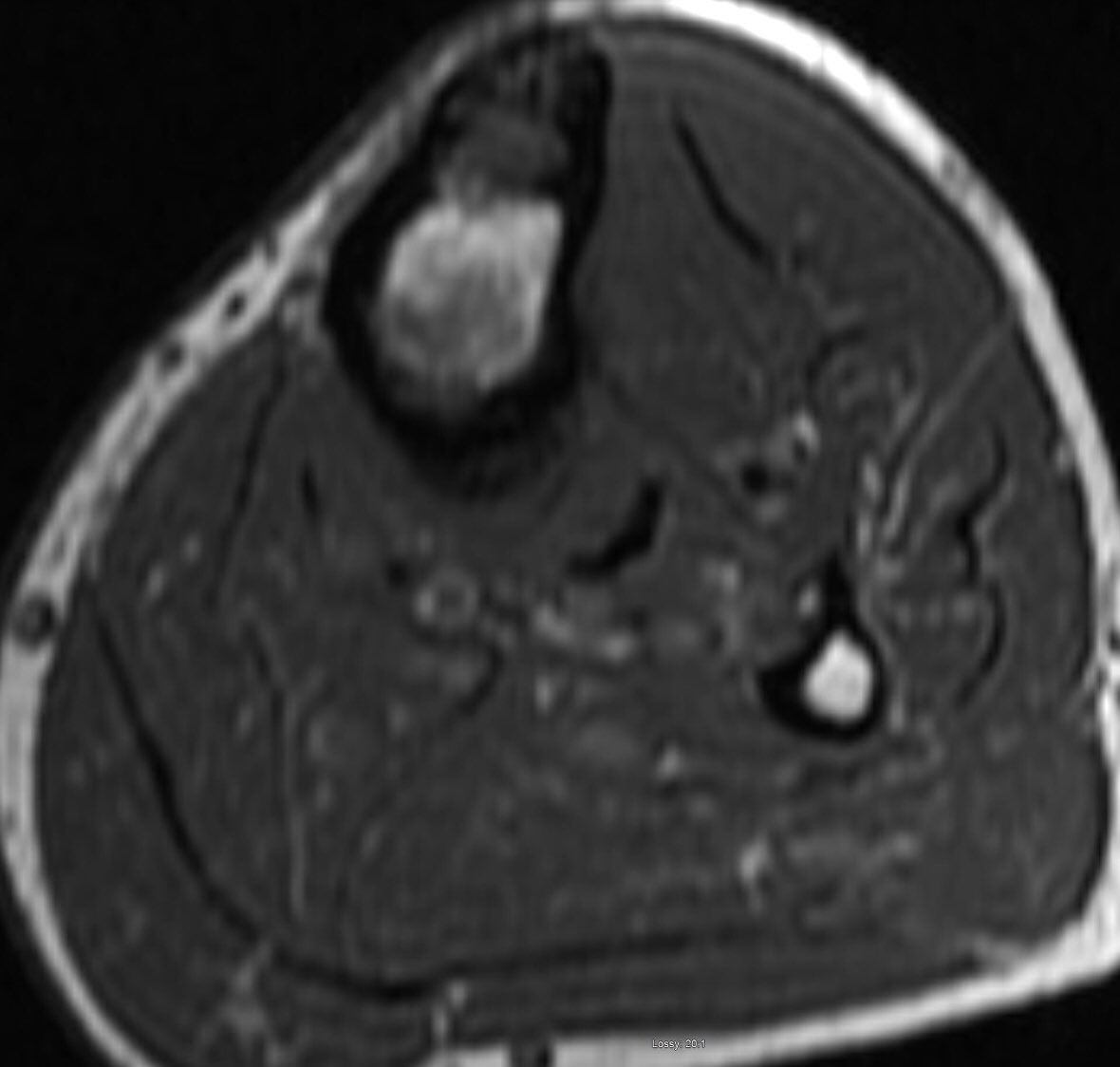
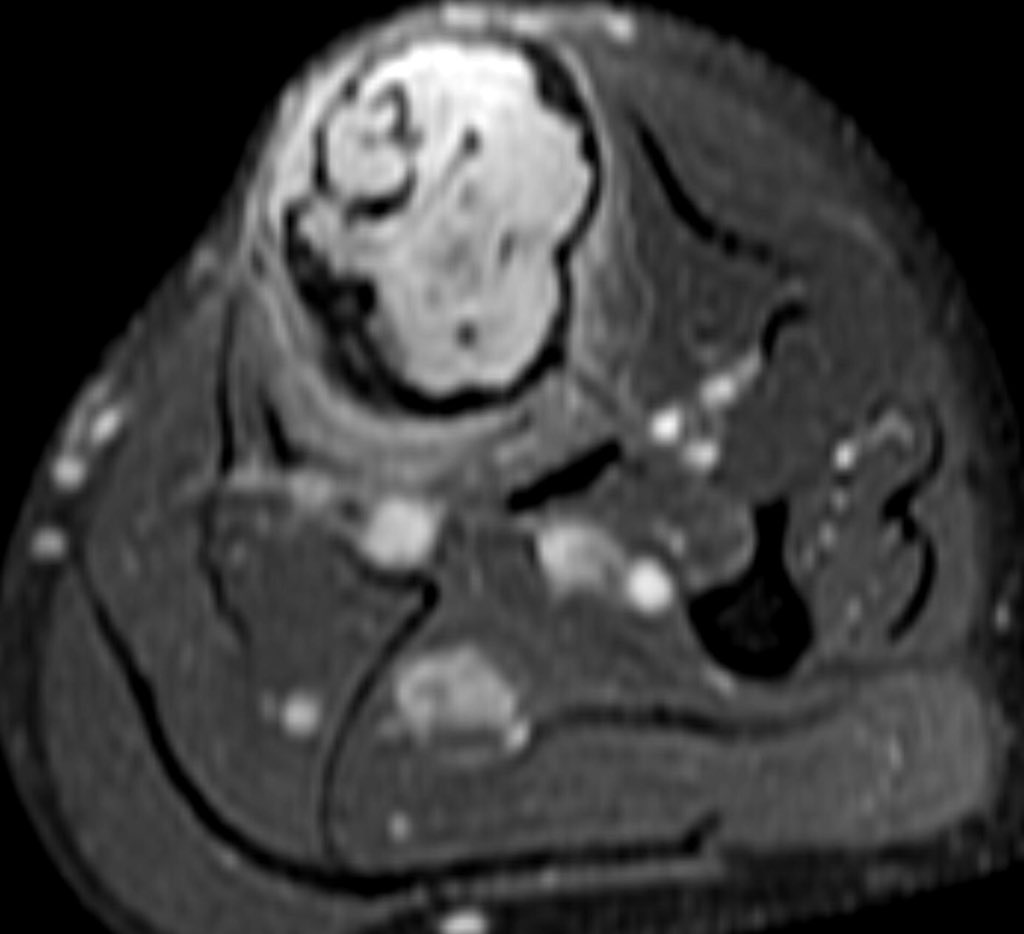
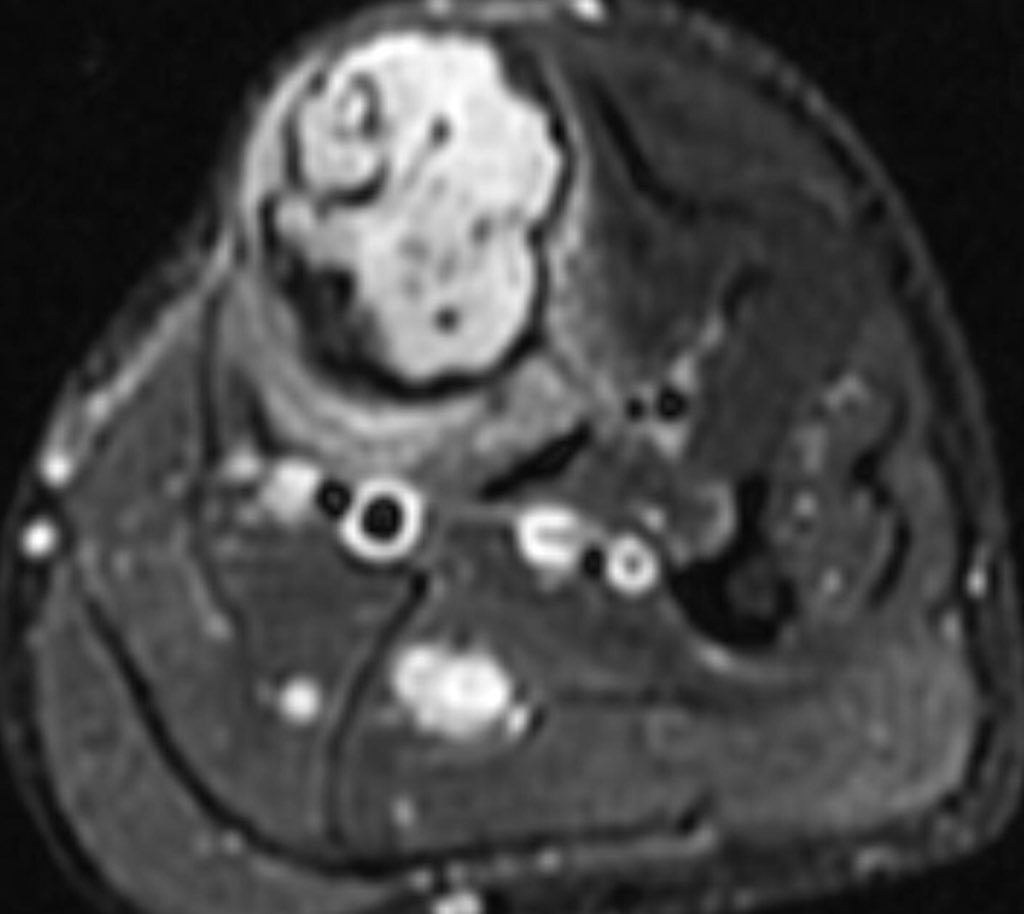
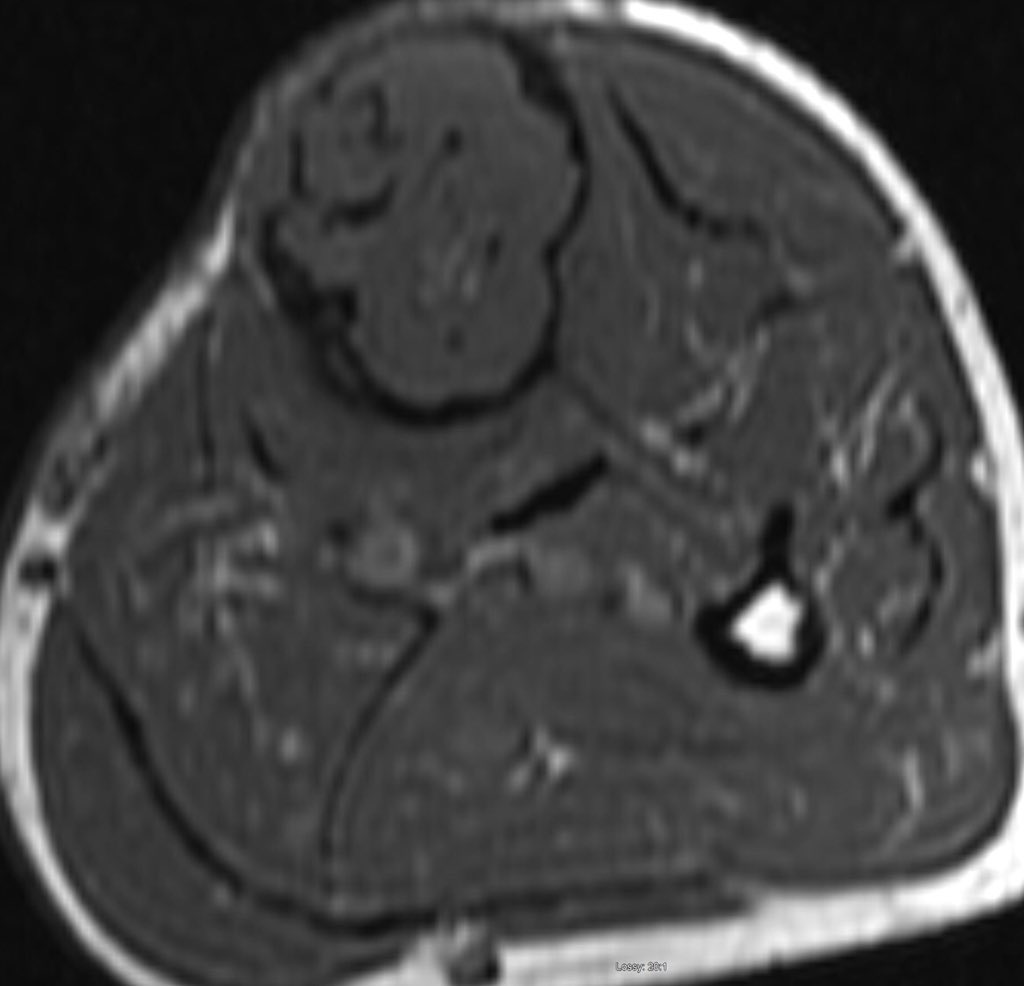
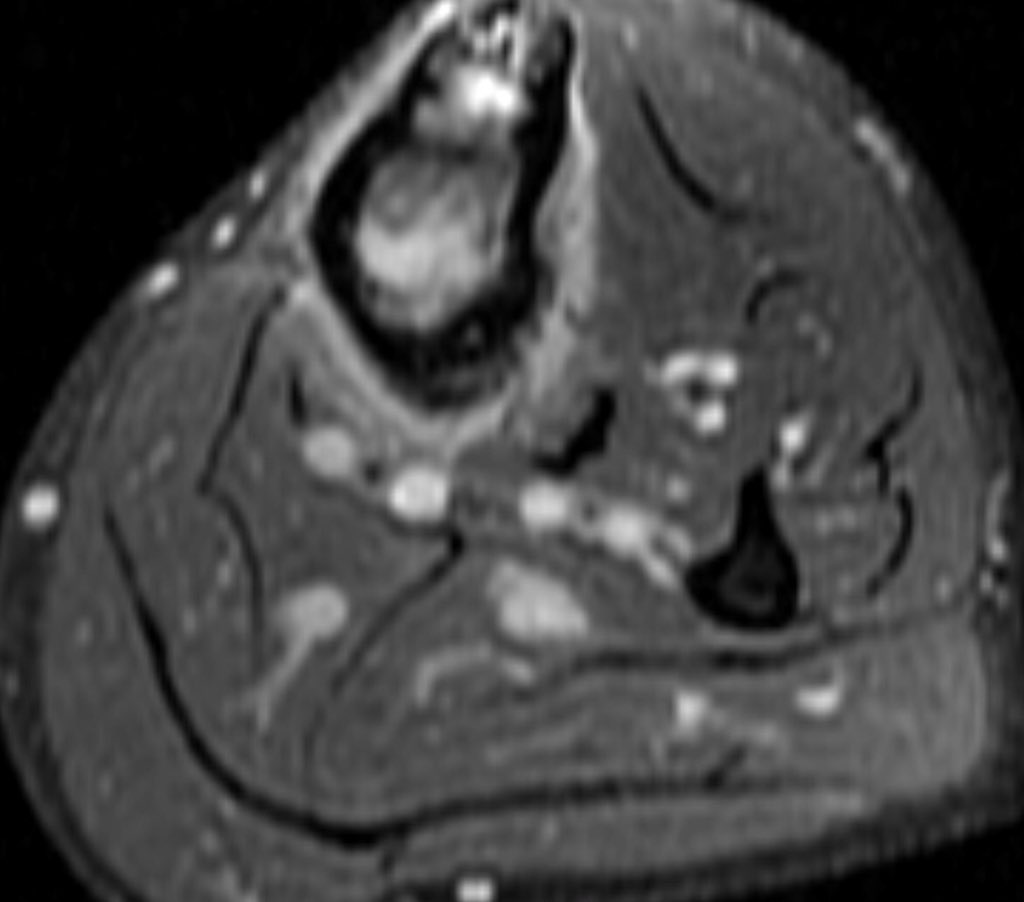
MRI is mandatory for accurate local staging (intramedullary extent, multifocal tibial and fibular disease and extra-osseous extension) and surgical planning. AD is typically isointense / mildly hyperintense to muscle on T1 weighted images
similar to fat on fast spin-echo T2 and hyperintense on inversion recovery and fluid-sensitive fat saturated sequences. The tumour enhances intensely and homogeneously.
The tumour in the current case appeared to have arisen in the anterior cortex, extending inferiorly into both cortex and medulla, as a single focus of disease. The trabeculated appearance on radiographs appears to reflect the unusual extension of tumour through tibial cortex.
, with preservation of vertical ridges of cortical bone, surrounded by tumour, adjacent to areas of marked cortical thinning. Oedema-like hyperintensity on the bone surface suggests imminent fracture
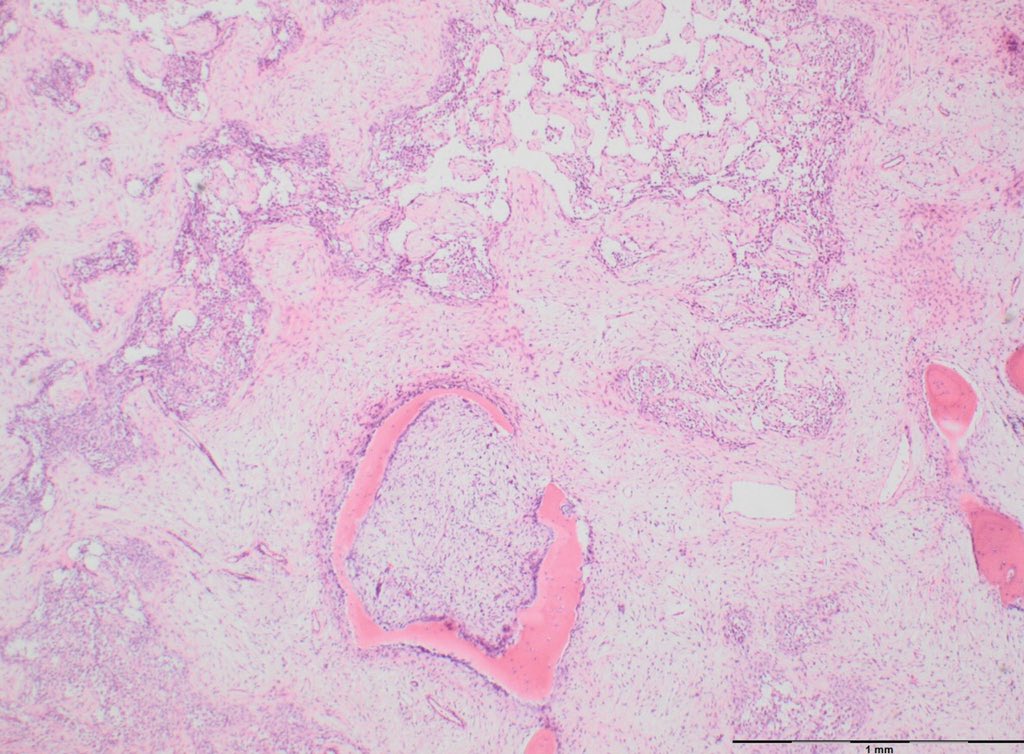
Macroscopically, these are multilobular, fleshy tumours that can be multifocal or involve a single area in the medullary canal. Cortical breach and soft tissue extension may be present.
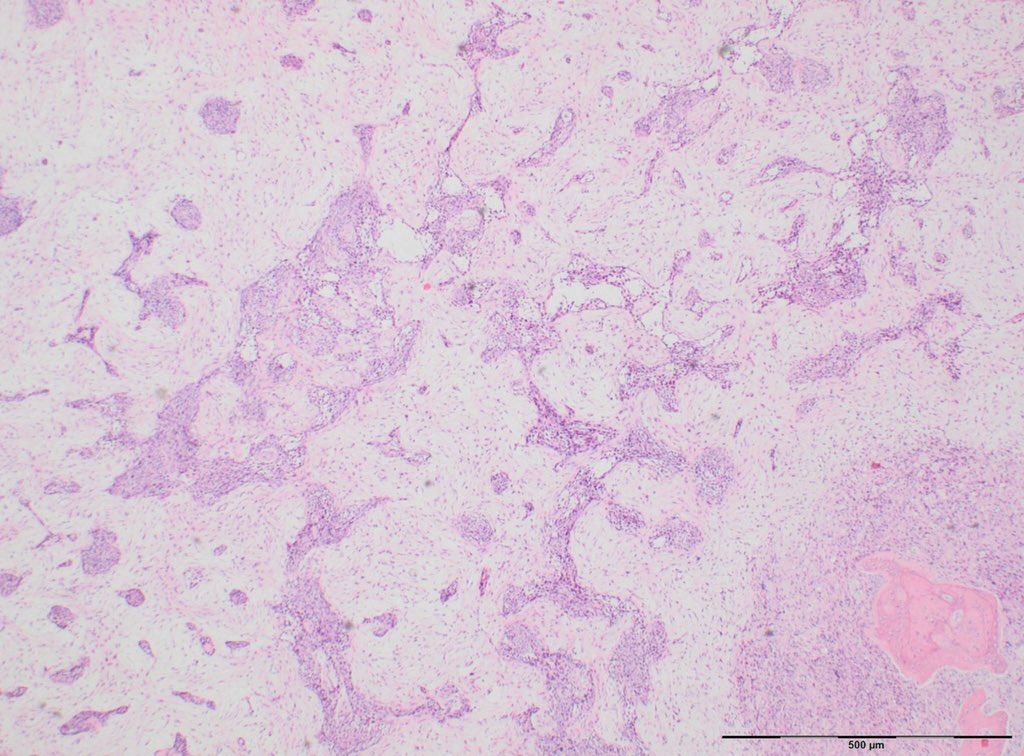
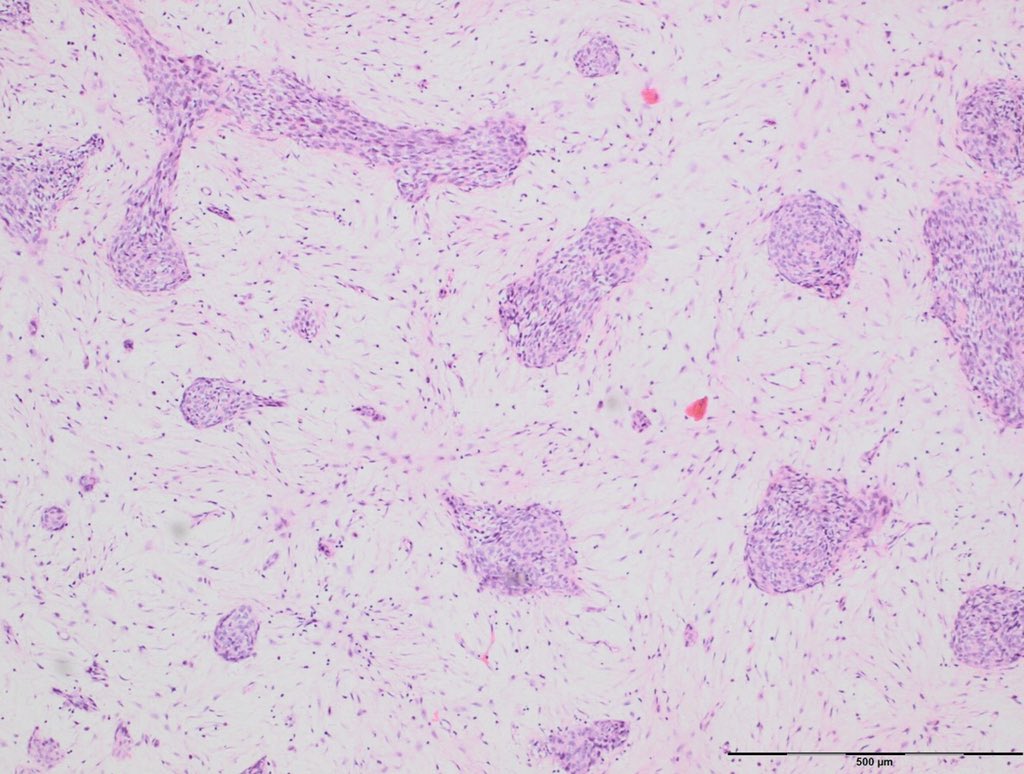
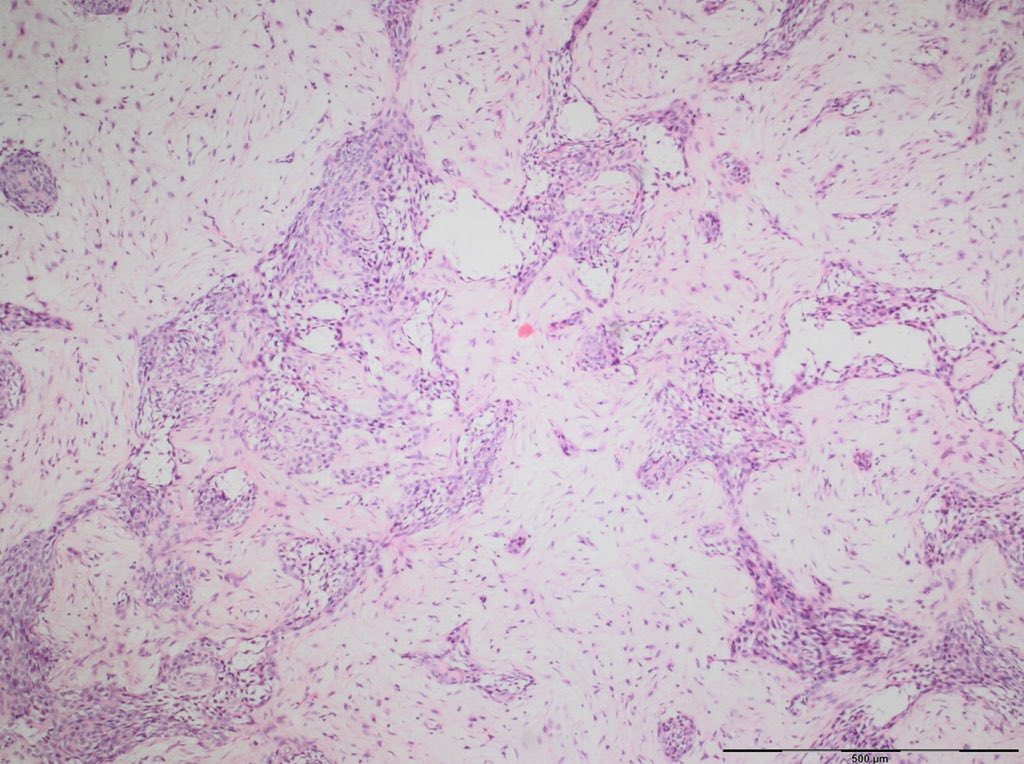
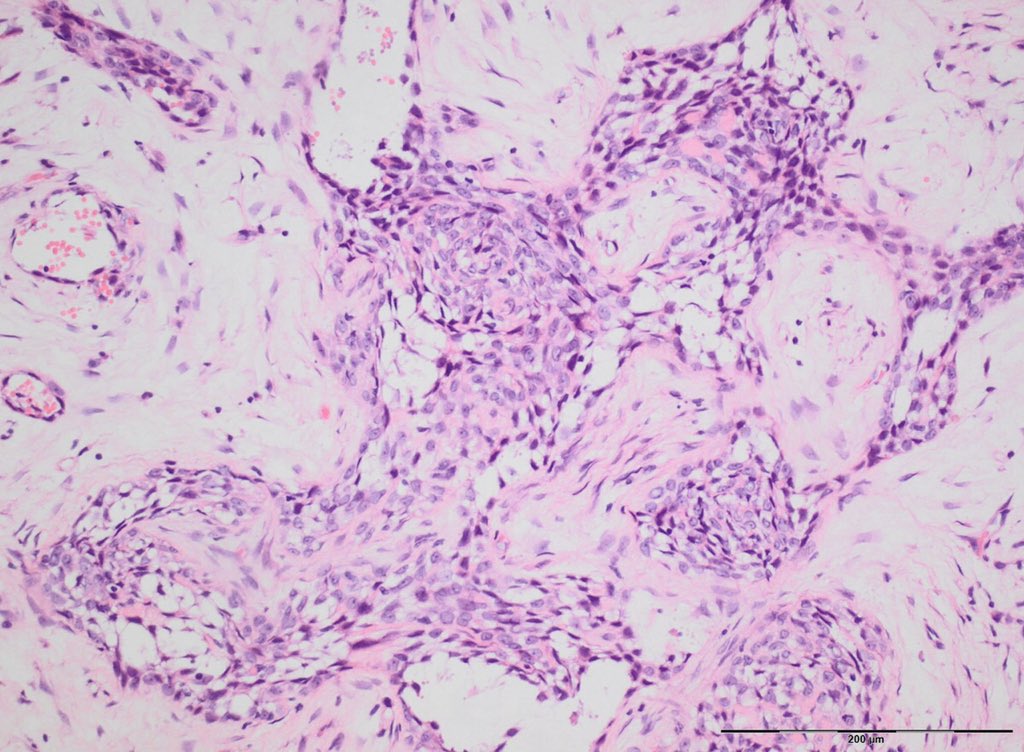
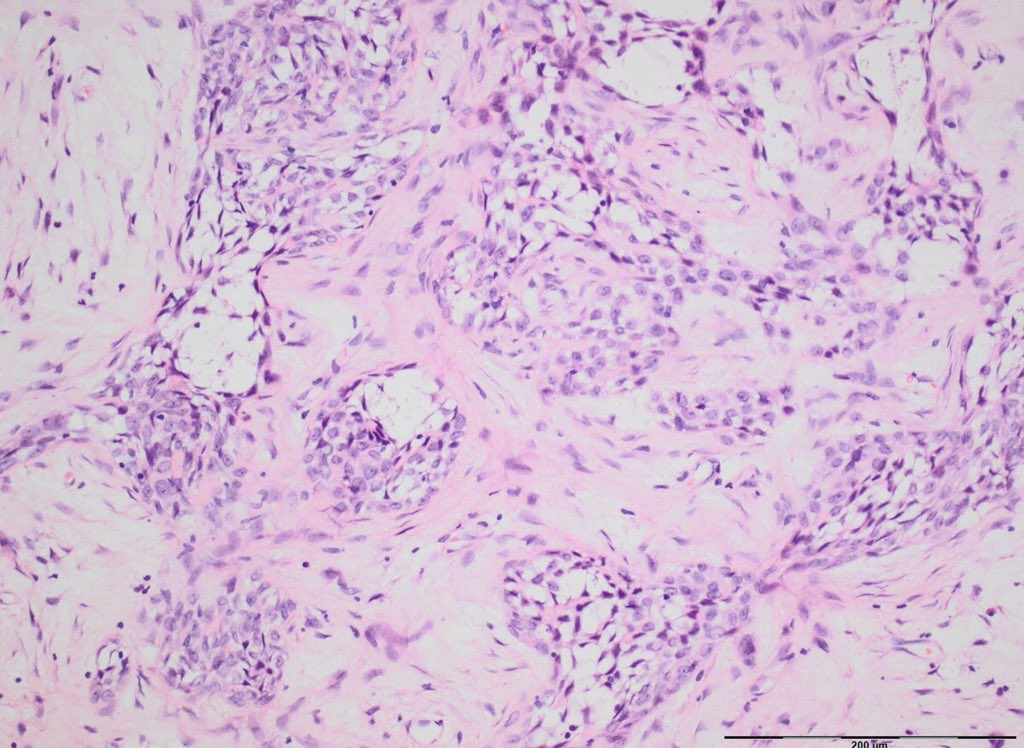
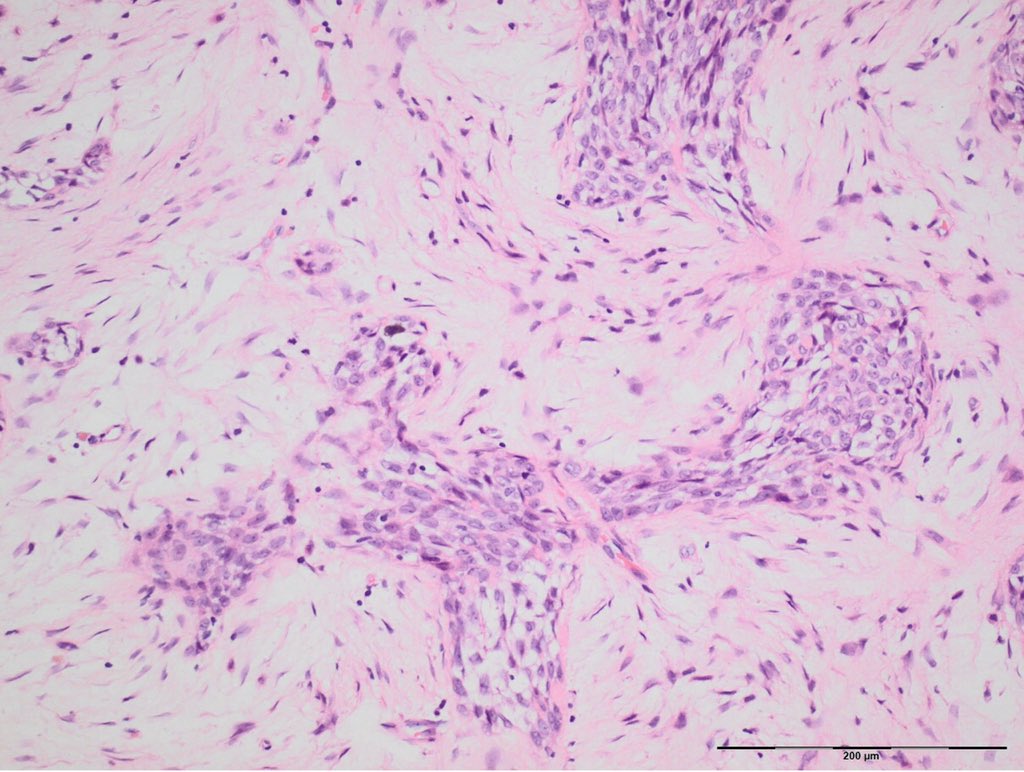
Histologically, these tumours show a biphasic pattern with epithelial or spindle cells in nests or aggregates, embedded in a paucicellular fibrous stroma.
Mitotic activity is usually low. The epithelioid component shows varied histological appearances, described as basaloid, squamous, tubular or spindle cell. The so-called differentiated / osteofibrous dysplasia-like AD
Adamantinoma may recur locally and metastasise in up to 25% cases, usually to the lungs. The treatment of choice is usually wide excision of the segment involved.
Loading suggestions...