

Hello 😍😍💕
Friends of my way♥️♥️😍
Today we are talking about Common surgical sinus & fistula👌
Friends of my way♥️♥️😍
Today we are talking about Common surgical sinus & fistula👌
📍The first
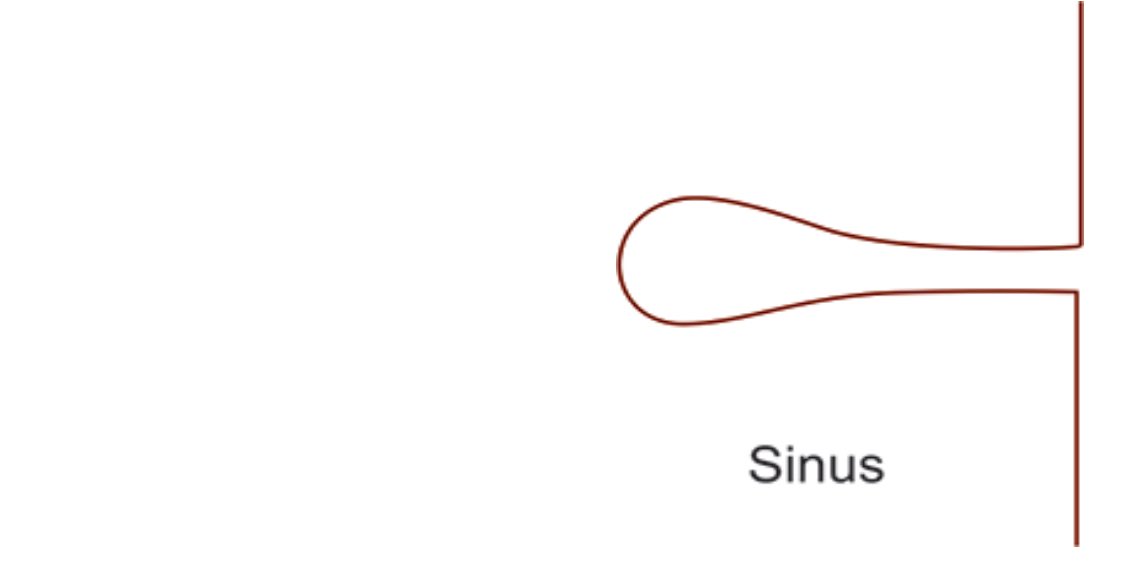
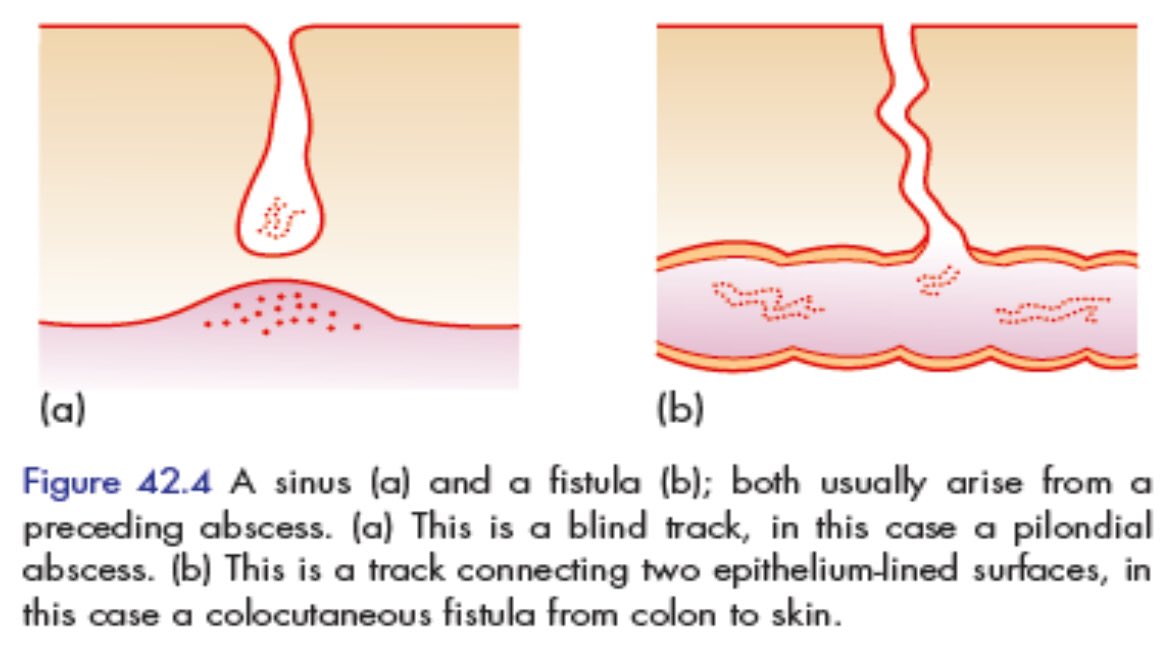
1️⃣ Sinus means “hollow”
• It is blind-ending tract that:
1-Connects a cavity lined with granulation tissue
>> often an abscess cavity
2-With an epithelial surface.
1️⃣ Sinus means “hollow”
• It is blind-ending tract that:
1-Connects a cavity lined with granulation tissue
>> often an abscess cavity
2-With an epithelial surface.
⚜️Etiology of sinus:
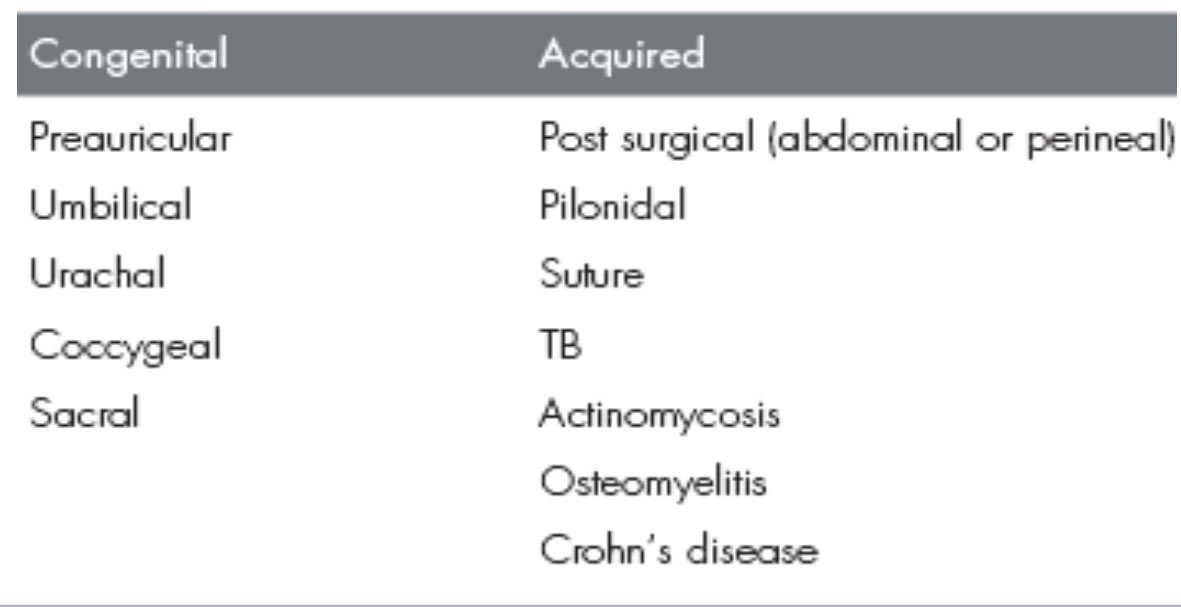
💠Congenital or acquired.
⚜️Congenital sinuses:
Arise from the remnants of embryonic ducts that persist instead of being obliterated & involute during embryonic development.
E. g:- Pre-auricular sinus.
💠Congenital or acquired.
⚜️Congenital sinuses:
Arise from the remnants of embryonic ducts that persist instead of being obliterated & involute during embryonic development.
E. g:- Pre-auricular sinus.

⚜️Acquired sinuses.
Occur as a result of the presence of:
💠A retained foreign body (for example suture material).
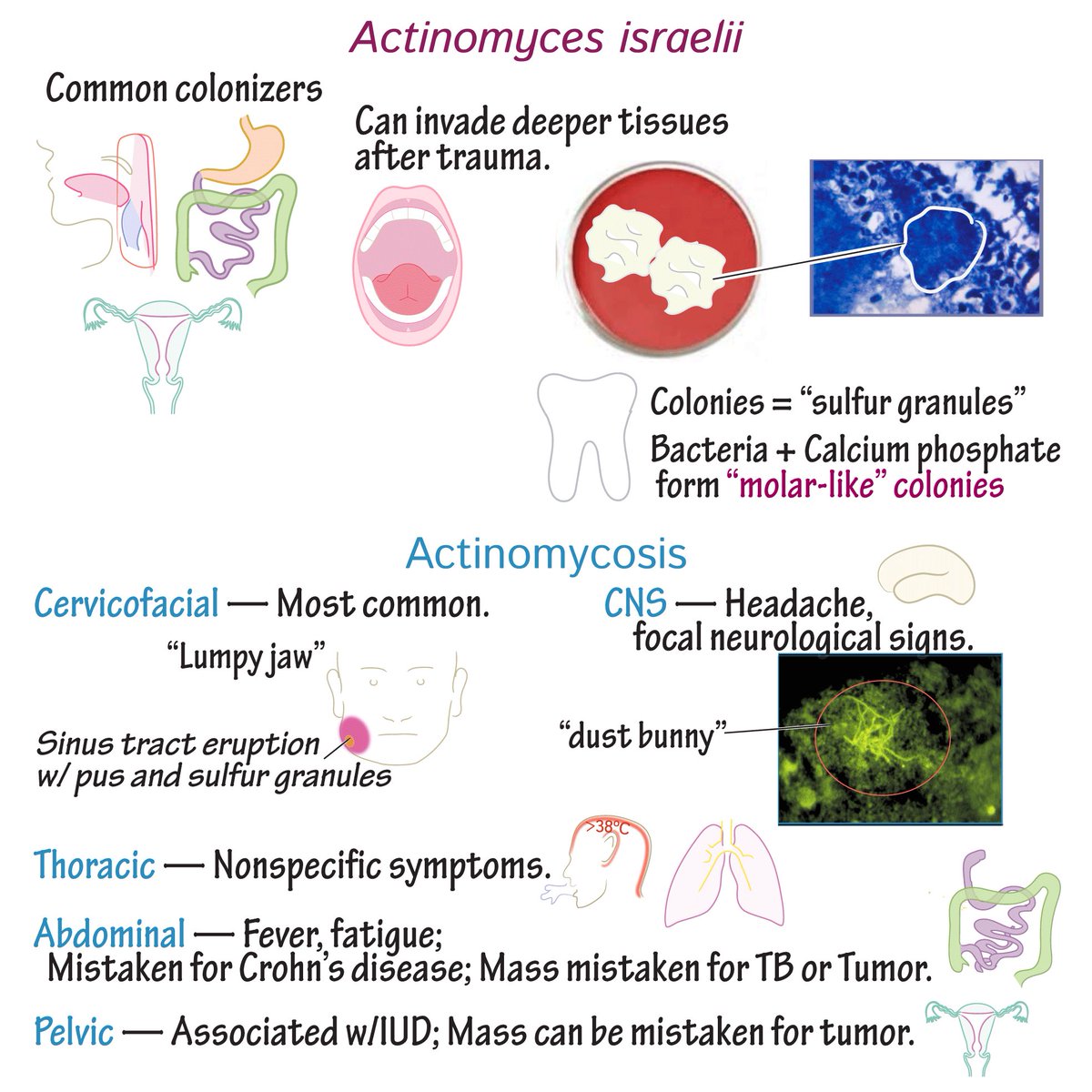
💠Specific chronic infection (for example (TB) or actinomycosis)
💠Pilonidal sinus.(very important)
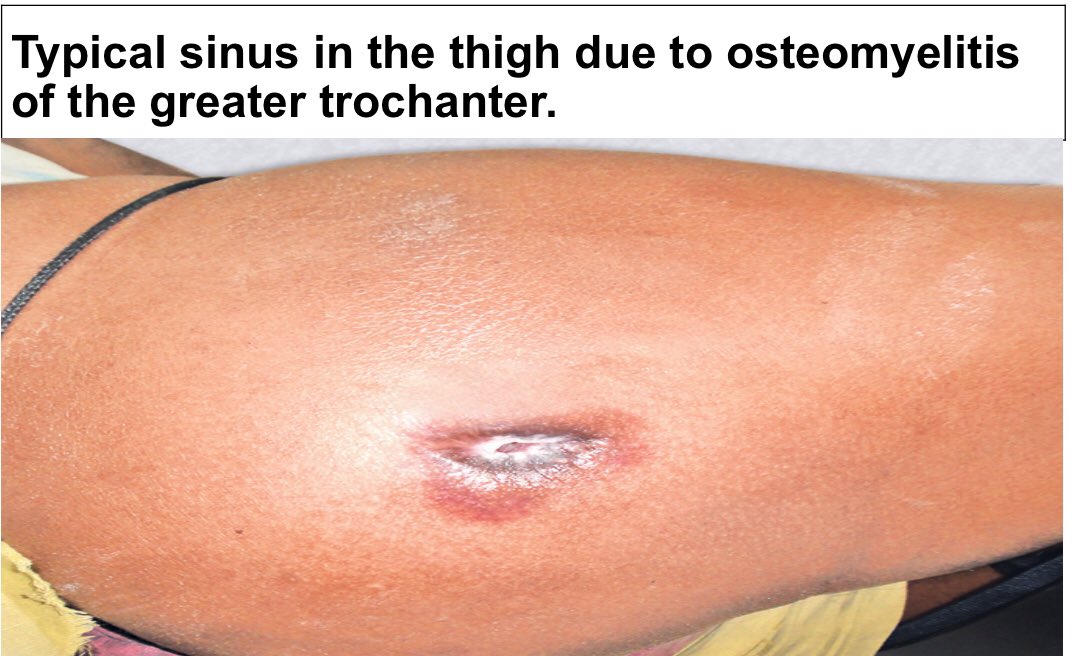
💠Chronic osteomyelitis.
Occur as a result of the presence of:
💠A retained foreign body (for example suture material).
💠Specific chronic infection (for example (TB) or actinomycosis)
💠Pilonidal sinus.(very important)
💠Chronic osteomyelitis.
📍The second
2️⃣ Fistula
• abnormal communication between two epithelium lined surfaces.
⚜️This communication or tract may be lined by:
1.Granulation tissue. or
2.Epithelialized in chronic cases
2️⃣ Fistula
• abnormal communication between two epithelium lined surfaces.
⚜️This communication or tract may be lined by:
1.Granulation tissue. or
2.Epithelialized in chronic cases
⚜️It’s an abnormal communication between:
●The lumen of one viscus to another.
or
●The body surface.
or
●The vessels.
Fistula means “flute” or “a pipe or tube.”
●The lumen of one viscus to another.
or
●The body surface.
or
●The vessels.
Fistula means “flute” or “a pipe or tube.”
⚜️Etiology of fistula
💠According to etiology
Congenital & acquired.
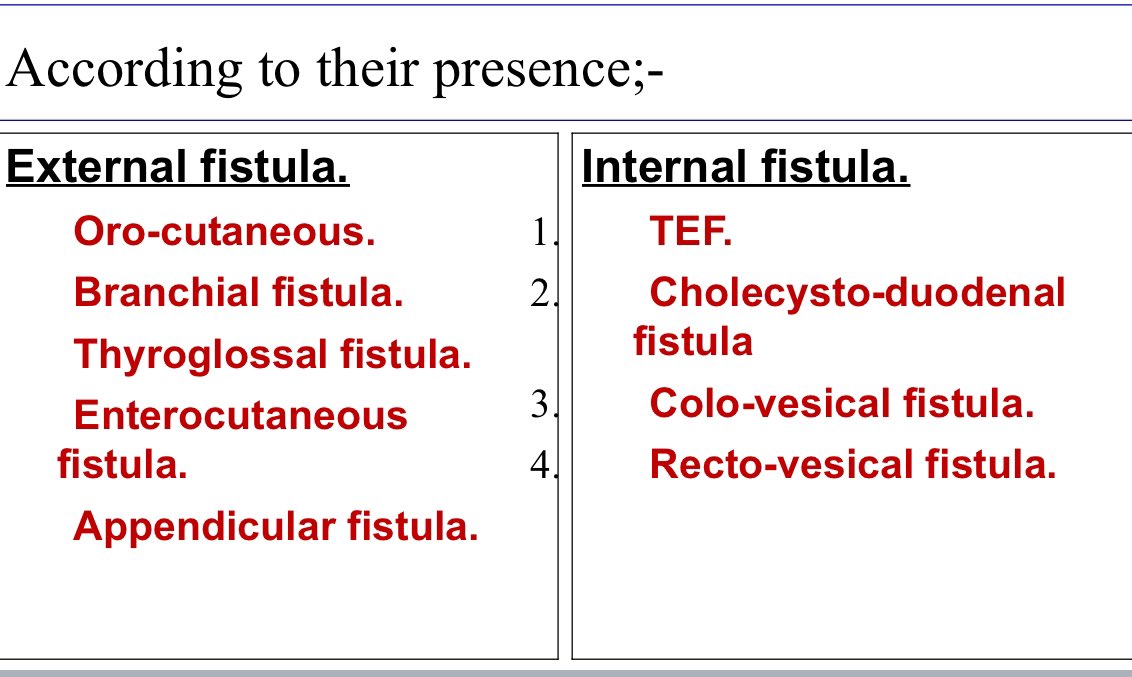
💠According to their presence:
⚜️External fistula & Internal fistula. See later.
📍Congenital:
•Branchial fistula.
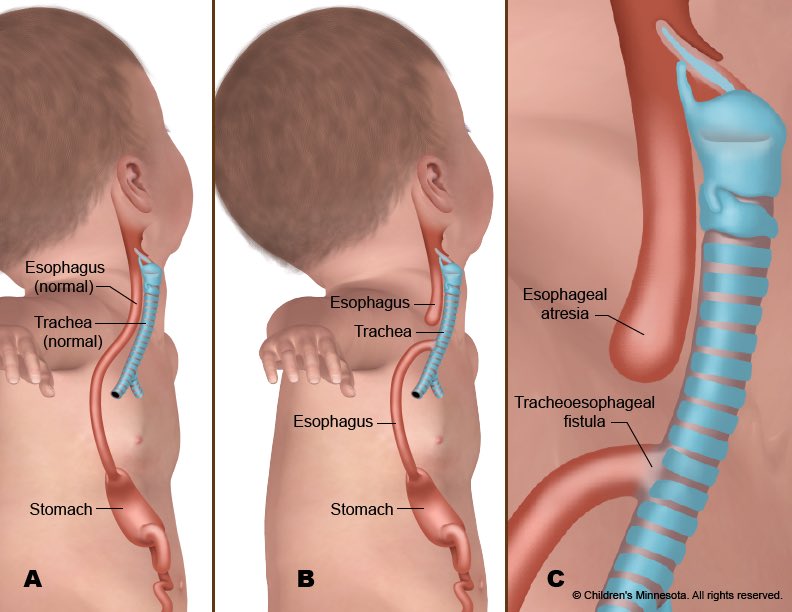
•Tracheoesophageal fistula (TEF).
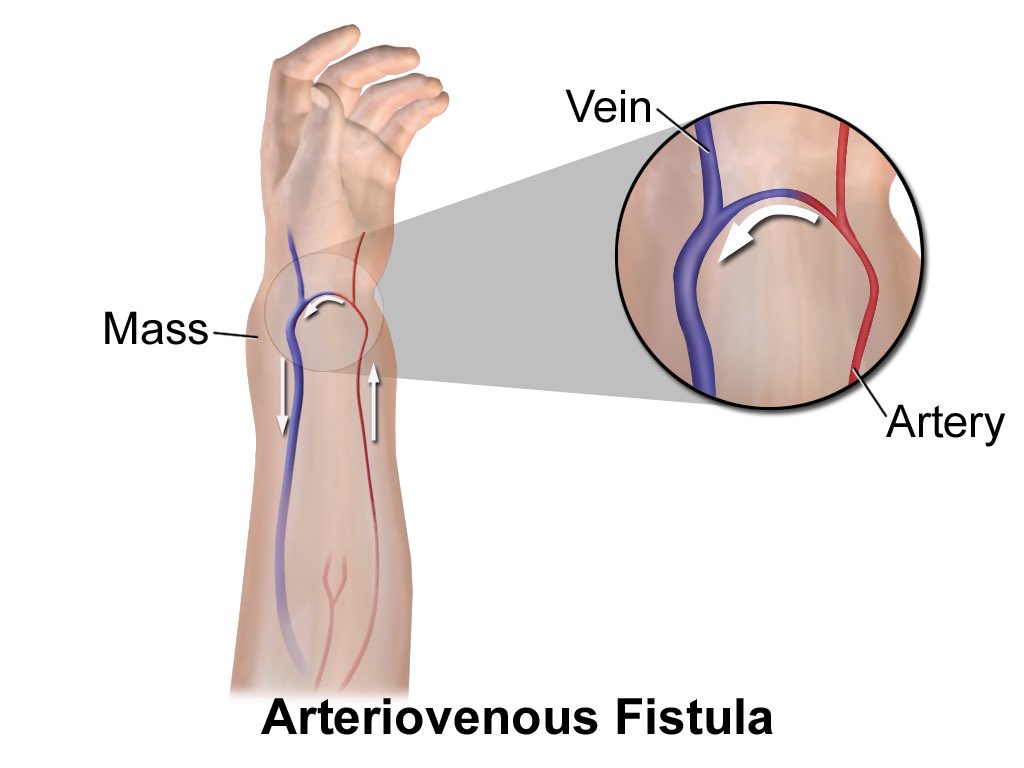
•Congenital A-V fistula.
•Umbilical fistula.
💠According to etiology
Congenital & acquired.
💠According to their presence:
⚜️External fistula & Internal fistula. See later.
📍Congenital:
•Branchial fistula.
•Tracheoesophageal fistula (TEF).
•Congenital A-V fistula.
•Umbilical fistula.
📍Acquired:
1️⃣Traumatic or iatrogenic following:
•Surgery
•Intestinal fistulas
•Enterocutaneous.
•Postop. anastomotic complications.
•A-V fistula
•Instrumental delivery
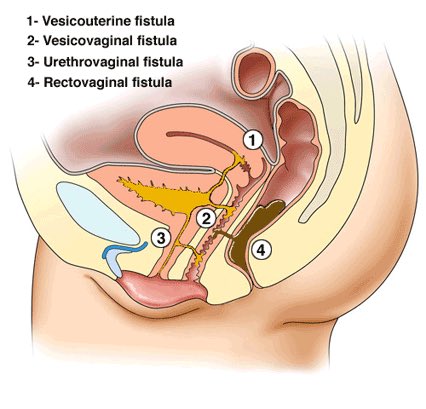
•Vesico-vaginal fistula.
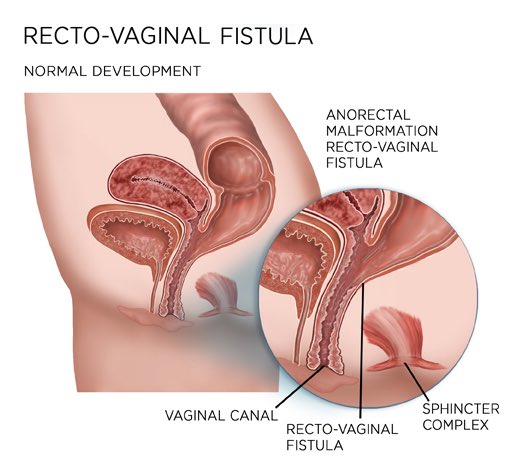
•Recto-vaginal fistula.
•Uretero-vaginal fistula.
1️⃣Traumatic or iatrogenic following:
•Surgery
•Intestinal fistulas
•Enterocutaneous.
•Postop. anastomotic complications.
•A-V fistula
•Instrumental delivery
•Vesico-vaginal fistula.
•Recto-vaginal fistula.
•Uretero-vaginal fistula.
2️⃣ Inflammatory:
•Intestinal action-mycosis.
•Tuberculosis.
•Crohn’s disease.
3️⃣Malignancy:
•Recto-vesical fistulas as in CA rectum.
•Vesico-uterine fistulas as in CA uterus.
•Intestinal action-mycosis.
•Tuberculosis.
•Crohn’s disease.
3️⃣Malignancy:
•Recto-vesical fistulas as in CA rectum.
•Vesico-uterine fistulas as in CA uterus.
📍C\P of sinus & fistula:
⚜️Sinus may be single or multiple.
⚜️Discharge from the opening .
⚜️No floor.
⚜️Edge → raised indurated.
⚜️Base → indurated & non-mobile.
⚜️Often granulation tissue over the sinus opening
🛑Induration is a feature of all chronic fistulas except > T.B
⚜️Sinus may be single or multiple.
⚜️Discharge from the opening .
⚜️No floor.
⚜️Edge → raised indurated.
⚜️Base → indurated & non-mobile.
⚜️Often granulation tissue over the sinus opening
🛑Induration is a feature of all chronic fistulas except > T.B
⚜️Surrounding skin may be:
•Erythematous > in inflammatory.
•Bluish in > tuberculosis.
•Excoriated in > fecal fistula.
•Pigmented in > chronic sinuses/fistulas.
•Erythematous > in inflammatory.
•Bluish in > tuberculosis.
•Excoriated in > fecal fistula.
•Pigmented in > chronic sinuses/fistulas.
⚜️Discharge typical of the cause will be evident which will be obvious after applying pressure over surrounding area.
⚜️Thickening of the bone underneath on palpation if sinus is adherent to bone or if there is osteomyelitis.
⚜️Enlargement of regional (LNs).
⚜️Thickening of the bone underneath on palpation if sinus is adherent to bone or if there is osteomyelitis.
⚜️Enlargement of regional (LNs).
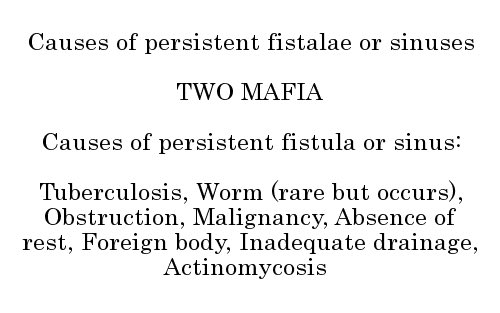
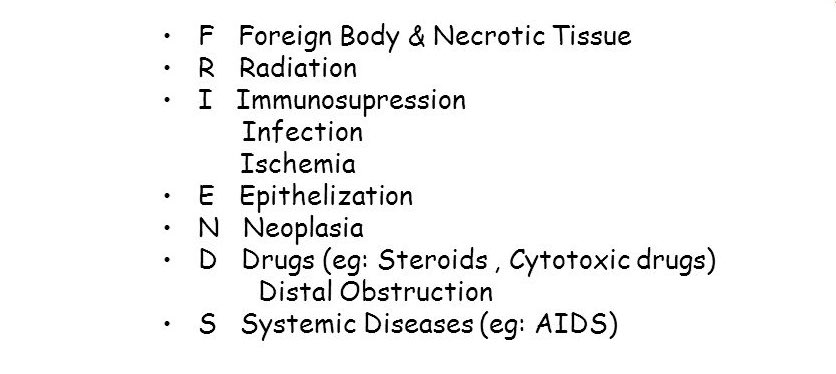
💠Causes of persistence of a sinus or fistula:
🔖(TWO MAFIA)
🔖(FRIENDS)
🔖(TWO MAFIA)
🔖(FRIENDS)
💠Most important point:
The most common cause of sinus in neck is T.B
⚜️Commonly it’s tuberculous lymphadenitis.
⚜️It shows yellowish cheesy discharge with bluish margin.
⚜️Usually tuberculous sinus/ulcer do not show any induration.
The most common cause of sinus in neck is T.B
⚜️Commonly it’s tuberculous lymphadenitis.
⚜️It shows yellowish cheesy discharge with bluish margin.
⚜️Usually tuberculous sinus/ulcer do not show any induration.
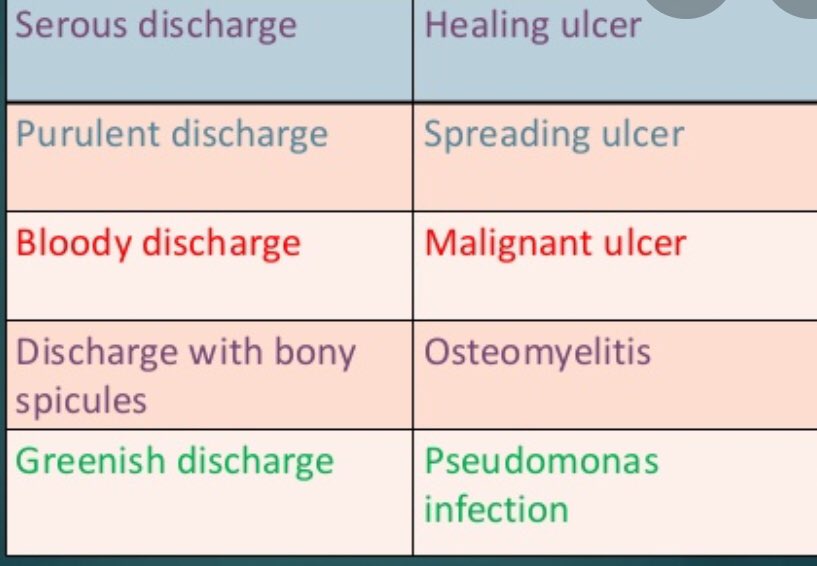
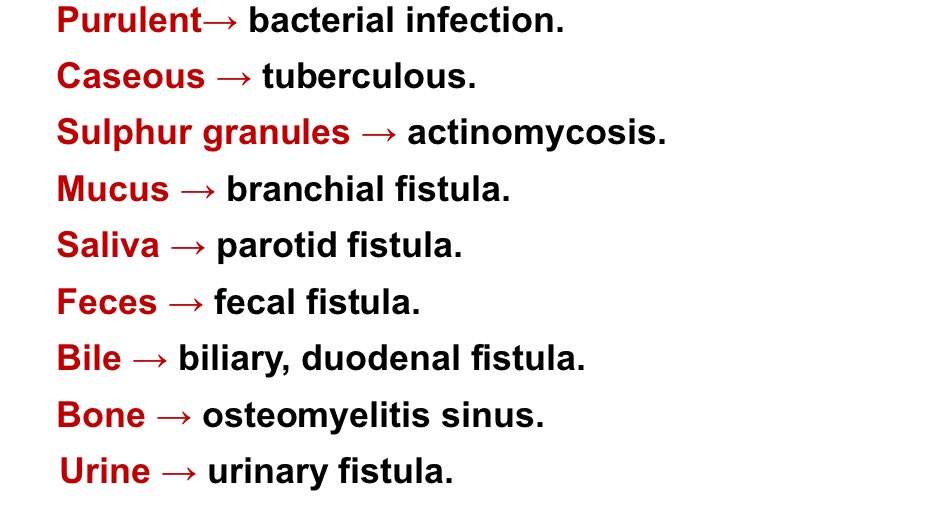
📍Different discharges in a sinus/fistula
💠Investigations🔬
1.Fistulograrm / Sinusogram using
2.Discharge for C/S, cytology, staining.
3.Biopsy from the edge for TB & malignancy.
4.X-ray of the part.
5.MRI (most reliable) of the part.
6.ESR.
7.CT Sinusogram.
1.Fistulograrm / Sinusogram using
2.Discharge for C/S, cytology, staining.
3.Biopsy from the edge for TB & malignancy.
4.X-ray of the part.
5.MRI (most reliable) of the part.
6.ESR.
7.CT Sinusogram.
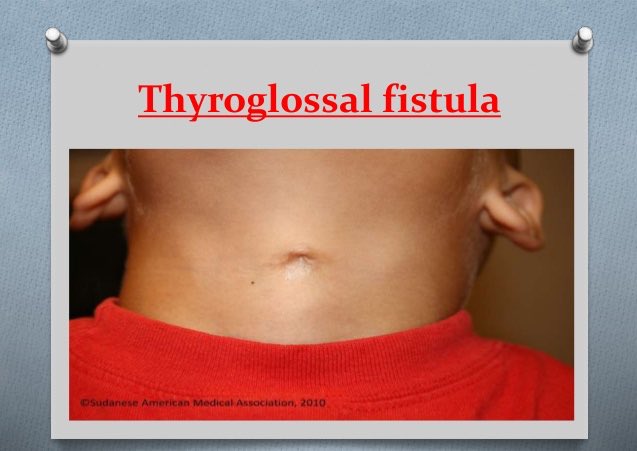
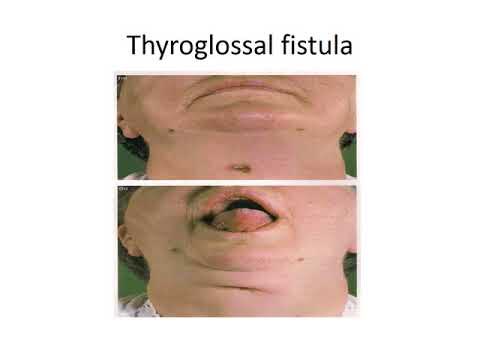
💡Thyroglossal fistula💡
⚜️Causes of Thyroglossal fistula:
🛑Never congenital term. It's acquired lesion
1️⃣Infection or incision of pre-excisting cyst. Or
2️⃣Inadequate removal of the cyst.
🛑Never congenital term. It's acquired lesion
1️⃣Infection or incision of pre-excisting cyst. Or
2️⃣Inadequate removal of the cyst.
⚜️Characters:
1️⃣A tinny opening at the midline of the neck. Supra or infra-hyoid. 10% to LT. side
2️⃣Chronic cases may show “Hood sign”
3️⃣Lined by columnar epithelium discharging: Serous, mucoid, mucopurulent
4️⃣Mobility: Moves with deglutition & protrusion of tongue.
1️⃣A tinny opening at the midline of the neck. Supra or infra-hyoid. 10% to LT. side
2️⃣Chronic cases may show “Hood sign”
3️⃣Lined by columnar epithelium discharging: Serous, mucoid, mucopurulent
4️⃣Mobility: Moves with deglutition & protrusion of tongue.
5️⃣Attachment: Fibrous band connecting it to base of tongue → persistent traction on skin of fistula → inverted inward → crescent in shape.

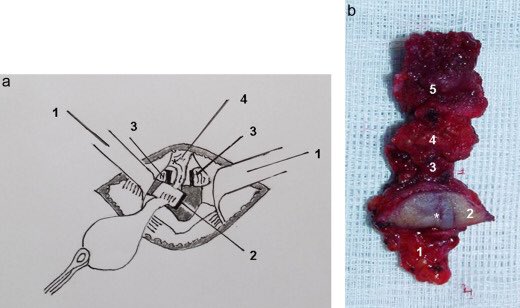
📍Treatment:
💠(Sistruk’s operation)
Multiple transverse incisions to dissect & follow up tract.
Excision of mid portion of hyoid bone:
The fistulous tract has an intimate relation to back of center of hyoid bone. So, removal of central part is mandatory to avoid recurrence.
💠(Sistruk’s operation)
Multiple transverse incisions to dissect & follow up tract.
Excision of mid portion of hyoid bone:
The fistulous tract has an intimate relation to back of center of hyoid bone. So, removal of central part is mandatory to avoid recurrence.
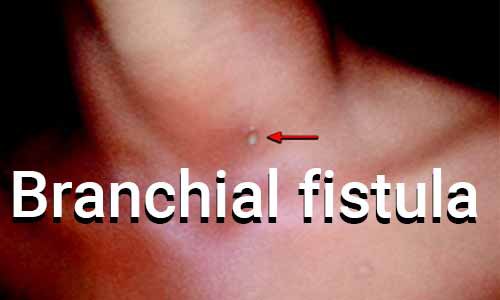
💡Branchial fistula💡
💠Types:
1️⃣Congenital type.
⚜️Due to failure of fusion of the 2nd branchial cleft with the 5th branchial cleft.
⚜️The fistula lies at the anterior border of lower 1/3 of sternomastoid muscles.
💠Types:
1️⃣Congenital type.
⚜️Due to failure of fusion of the 2nd branchial cleft with the 5th branchial cleft.
⚜️The fistula lies at the anterior border of lower 1/3 of sternomastoid muscles.
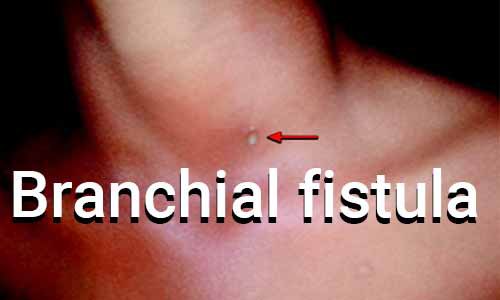

2️⃣Acquired type.
⚜️Due to infection or incision of branchial cyst.
⚜️The fistula is present at upper 1/3 of neck along anterior border of sternomastoid muscle.
📍Treatment.
Complete excision
⚜️Due to infection or incision of branchial cyst.
⚜️The fistula is present at upper 1/3 of neck along anterior border of sternomastoid muscle.
📍Treatment.
Complete excision

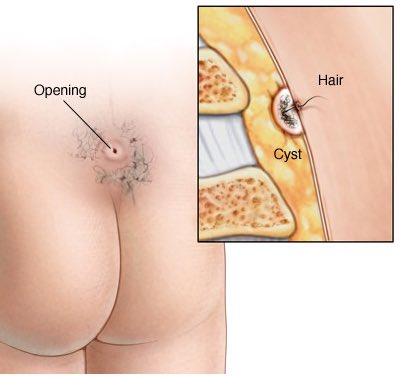
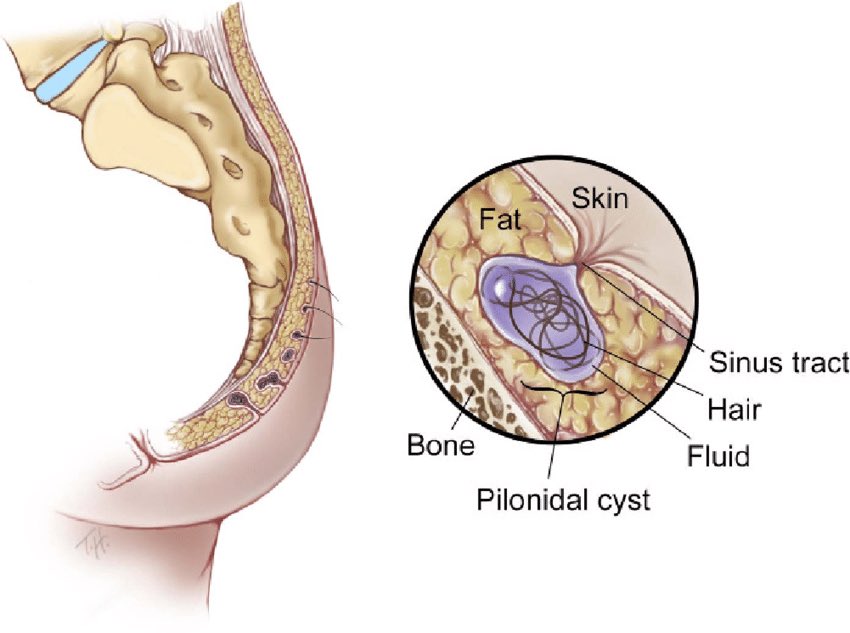
💡Pilonidal sinus💡
💠A hair containing sinus or abscess.
💠These are short tracts leading from an opening in the skin near the top of the buttocks or natal cleft overlying sacrum.
💠The tract is lined with granulation tissue and can get filled with hair debris and bacteria
💠A hair containing sinus or abscess.
💠These are short tracts leading from an opening in the skin near the top of the buttocks or natal cleft overlying sacrum.
💠The tract is lined with granulation tissue and can get filled with hair debris and bacteria

⚜️Etiology:
Unclear, but It is thought that implantation of hair occurs in susceptible areas which sets up a foreign body reaction.
1️⃣Congenital theory: Infection of pre-existing dermoid cyst.
Unclear, but It is thought that implantation of hair occurs in susceptible areas which sets up a foreign body reaction.
1️⃣Congenital theory: Infection of pre-existing dermoid cyst.
2️⃣Acquired (more accepted):
Penetration of skin by short stout hairs, proofed by→
💠Common in hirsute individuals.
💠Extremely rare in children.
💠May occur at hairy other sites e.g. axilla, web of fingers in barbers.
💠Wall is lined by granulation tissue
Penetration of skin by short stout hairs, proofed by→
💠Common in hirsute individuals.
💠Extremely rare in children.
💠May occur at hairy other sites e.g. axilla, web of fingers in barbers.
💠Wall is lined by granulation tissue
📍 Risk factors:
💡Pilonidal sinuses are more common in males
💡Poor hygiene.
💡Obesity.
💡Hairdressers.
💡There is no genetic link save for preponderance towards body hair.
💡Pilonidal sinuses are more common in males
💡Poor hygiene.
💡Obesity.
💡Hairdressers.
💡There is no genetic link save for preponderance towards body hair.
📍Clinical features.
They are typically asymptomatic as sinus lies over the back. When they become infected, they form abscesses.
They are typically asymptomatic as sinus lies over the back. When they become infected, they form abscesses.
📍Treatment
💠Abscess
ncision & drainage.
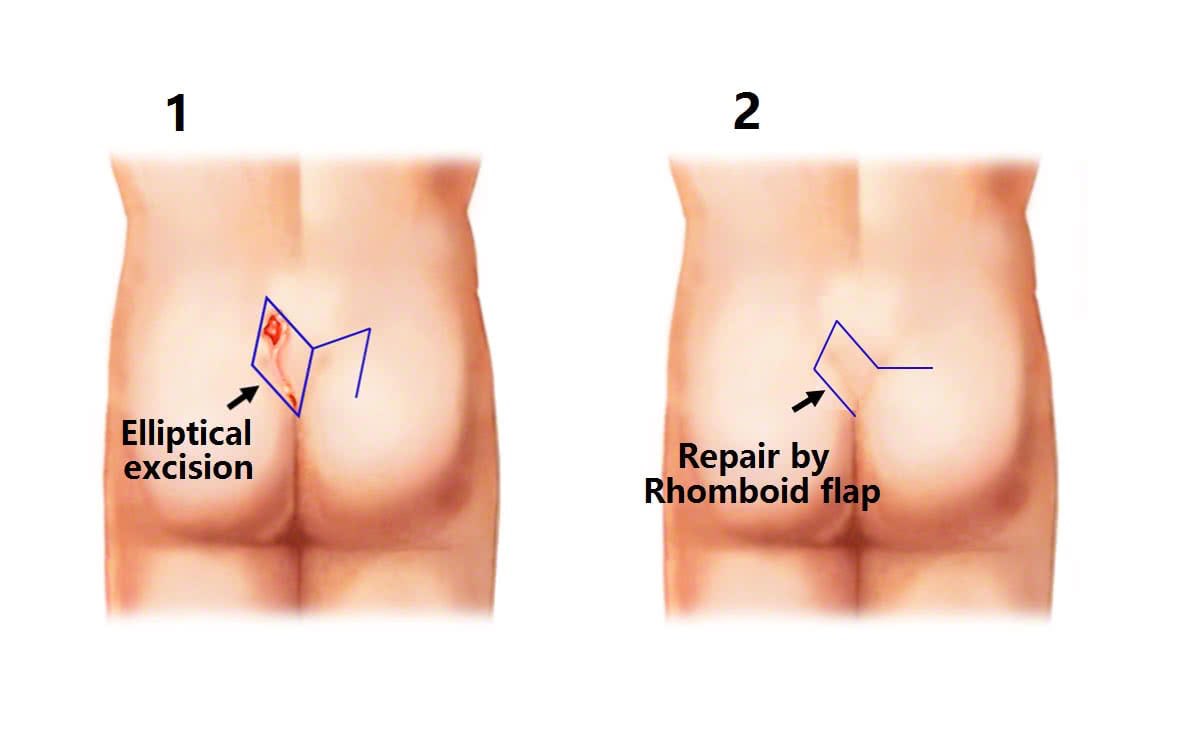
💠 Sinus: 4 Options
1️⃣Excision and The defect is closed by primary sutures
OR
2️⃣Excision. Wound is left opened to heal by granulation tissue
OR
💠Abscess
ncision & drainage.
💠 Sinus: 4 Options
1️⃣Excision and The defect is closed by primary sutures
OR
2️⃣Excision. Wound is left opened to heal by granulation tissue
OR
3️⃣Excision & use of rotational tissue flap.
4️⃣ Marsupialization
4️⃣ Marsupialization

References:🔎
•Bailey & Love's of Surgery
•Surgical Recall
•SRB's Manual of Surgery
✅DONE By: @Ahood0321
•Bailey & Love's of Surgery
•Surgical Recall
•SRB's Manual of Surgery
✅DONE By: @Ahood0321
Loading suggestions...