
Health
Podcasts
Medicine
Endocrinology
Hyperthyroidism
Graves Disease
Thyrotoxicosis
Thyroid Storm
BurchWartofsky Point Scale

Handout from our second Endocrinology episode "Episode 32: Hyperthyroidism" is now out!
📝Download it free here: #hyperthyroidism" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
🔊Episode: apple.co
#tweetorial on hyperthyroidism, Graves' disease, & interpretation of radioactive iodine uptake studies👇:
📝Download it free here: #hyperthyroidism" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
🔊Episode: apple.co
#tweetorial on hyperthyroidism, Graves' disease, & interpretation of radioactive iodine uptake studies👇:
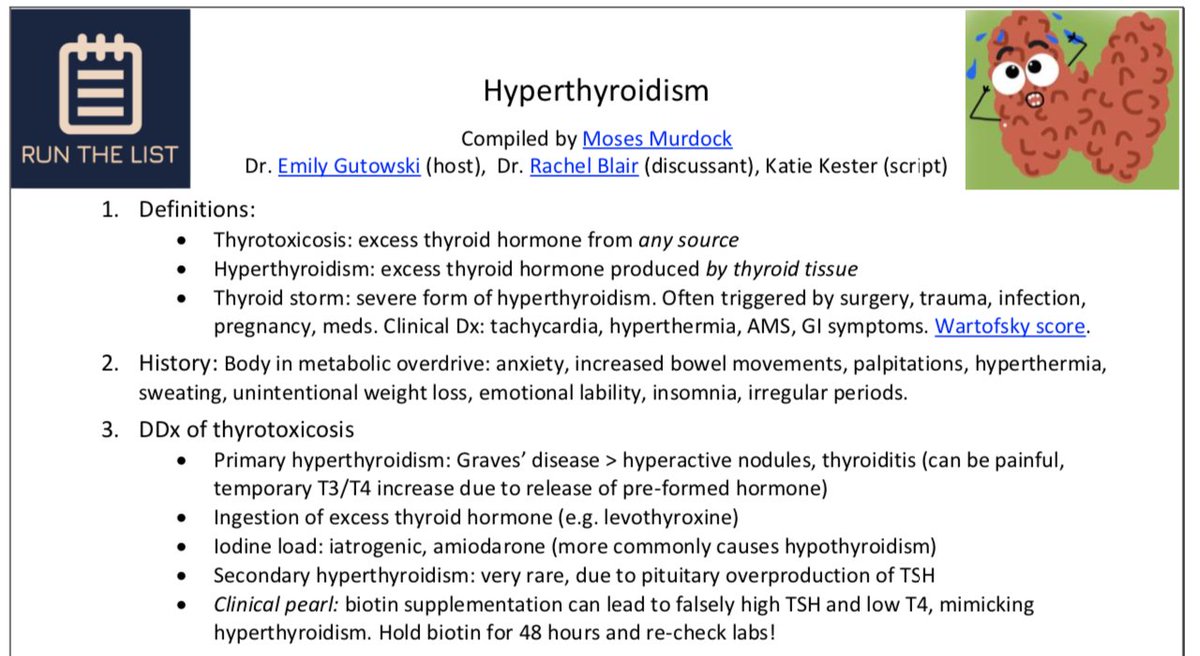

Let's recap:
1⃣Thyrotoxicosis is an☂️ term that refers to excess thyroid hormone from *any* source
2⃣Hyperthyroidism refers to excess thyroid hormone produced by the *thyroid* gland
3⃣Thyroid storm is a *severe* form of hyperthyroidism w/ particular triggers (e.g. surgery)
1⃣Thyrotoxicosis is an☂️ term that refers to excess thyroid hormone from *any* source
2⃣Hyperthyroidism refers to excess thyroid hormone produced by the *thyroid* gland
3⃣Thyroid storm is a *severe* form of hyperthyroidism w/ particular triggers (e.g. surgery)

Thyroid storm carries a significant mortality risk & is considered an endocrine emergency, often requiring ICU admission🚨!
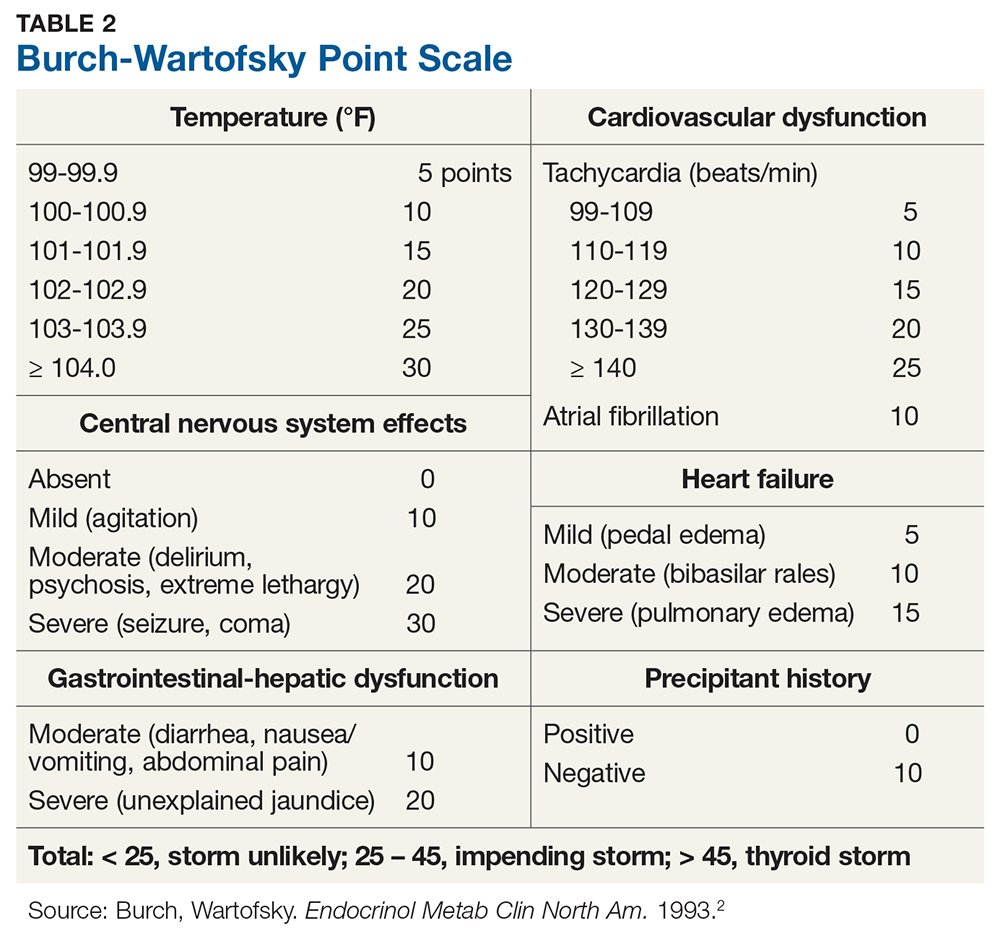
✏️Burch-Wartofsky Point Scale (BWPS) can be used to assess the severity of thyroid storm🌪️
<25 = 🌪️ unlikely
25-45 = impending 🌪️
>45 = thyroid 🌪️!
[1]
✏️Burch-Wartofsky Point Scale (BWPS) can be used to assess the severity of thyroid storm🌪️
<25 = 🌪️ unlikely
25-45 = impending 🌪️
>45 = thyroid 🌪️!
[1]
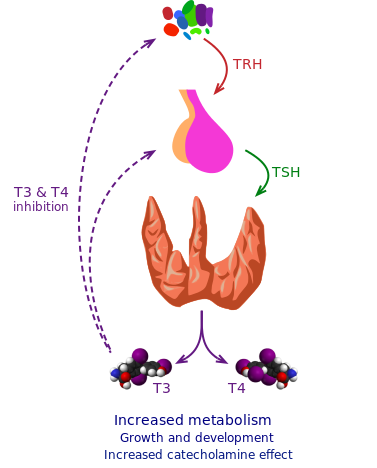
Last week, we learned from @RachelBlairMD that a TSH & subsequent free T4 were diagnostically helpful labs for hypothyroidism dx
w/ hyperthyroidism, Dr. Blair taught us that TSH, free T4, *and* total T3 are useful first-line tests to evaluate a patient w/ hyperthyroidism 🩺
[2]
w/ hyperthyroidism, Dr. Blair taught us that TSH, free T4, *and* total T3 are useful first-line tests to evaluate a patient w/ hyperthyroidism 🩺
[2]
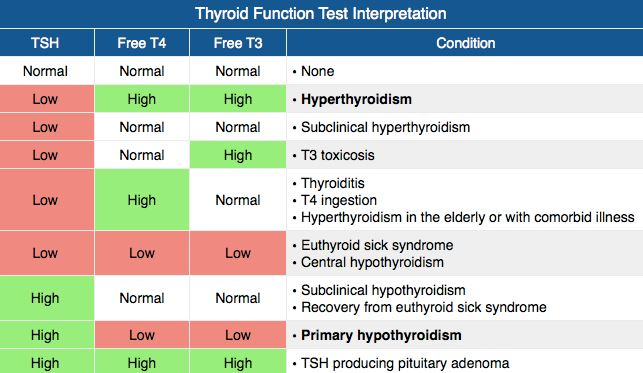
How can we use these labs to make the diagnosis of hyperthyroidism? We would expect:
-TSH to be⬇️*
-Free T4 to be⬆️**
-Total T3 to be⬆️
* "appropriately low" w/ primary hyperthyroidism
** free T4 can be normal in a subset of pts, so it's important to also check total T3!
[3]
-TSH to be⬇️*
-Free T4 to be⬆️**
-Total T3 to be⬆️
* "appropriately low" w/ primary hyperthyroidism
** free T4 can be normal in a subset of pts, so it's important to also check total T3!
[3]
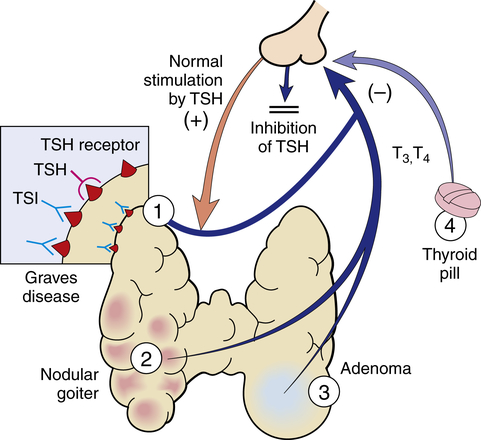
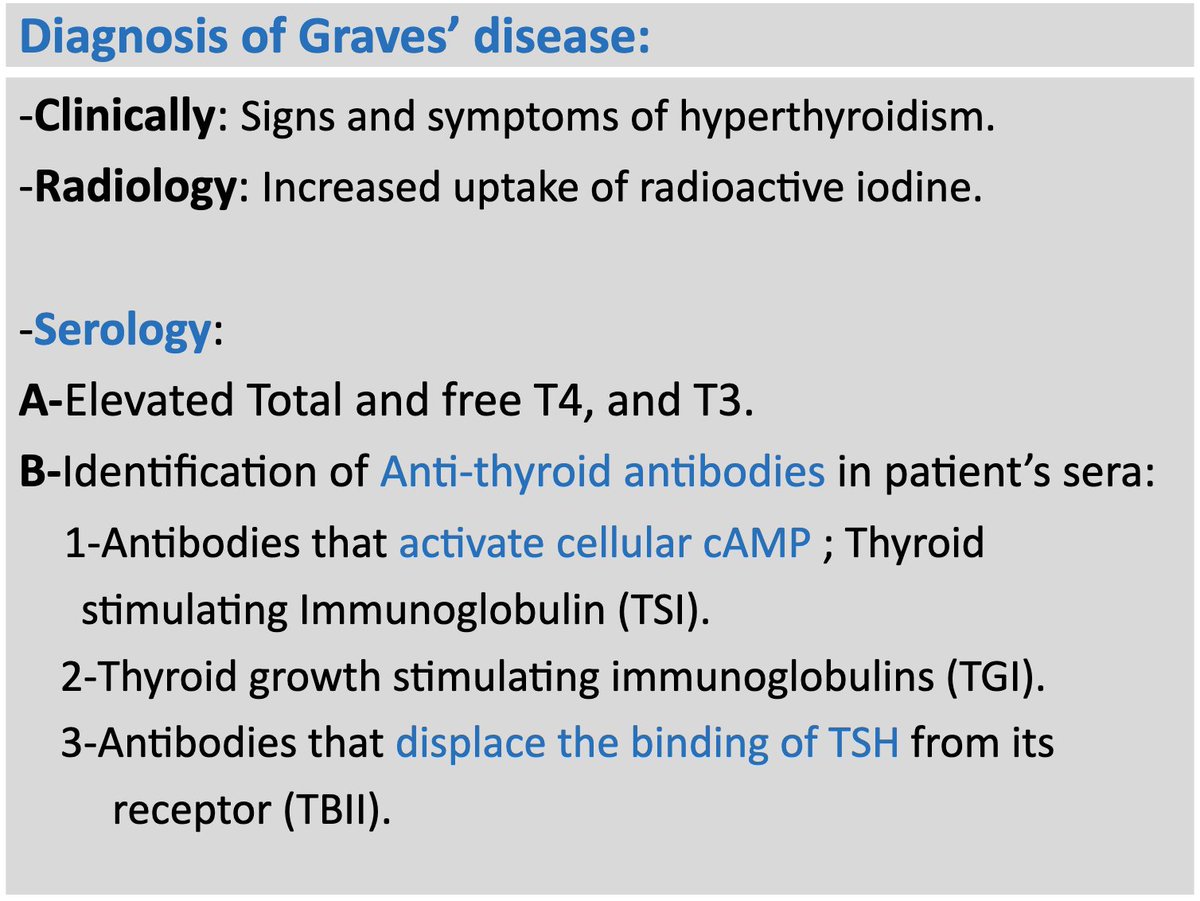
Now that we understand how to diagnose hyperthyroidism based on labs, what about the dx of Graves' disease?
*Graves' disease is a form of hyperthyroidism that results from thyroid-stimulating immunoglobulins (autoantibodies) that ⬆️ thyroid gland activity
*not Grave's 🪦!
[4]
*Graves' disease is a form of hyperthyroidism that results from thyroid-stimulating immunoglobulins (autoantibodies) that ⬆️ thyroid gland activity
*not Grave's 🪦!
[4]
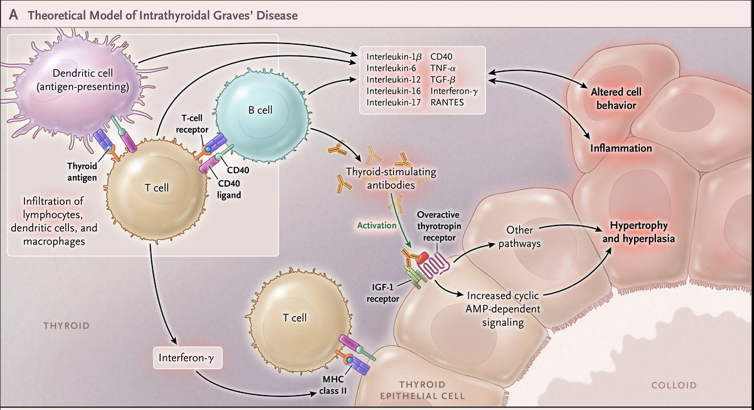
1⃣Graves' disease = most common cause of primary hyperthyroidism (F>M, peak age = 30-50 y.o.)
2⃣Clinical presentation:
-Weight loss
-Heat intolerance
-Anxiety
-Tremor
-Palpitations
-Ophthalmopathy (eyelid retraction, lid lag, bulging eyes [proptosis, exophthalmos], erythema)
[4]
2⃣Clinical presentation:
-Weight loss
-Heat intolerance
-Anxiety
-Tremor
-Palpitations
-Ophthalmopathy (eyelid retraction, lid lag, bulging eyes [proptosis, exophthalmos], erythema)
[4]
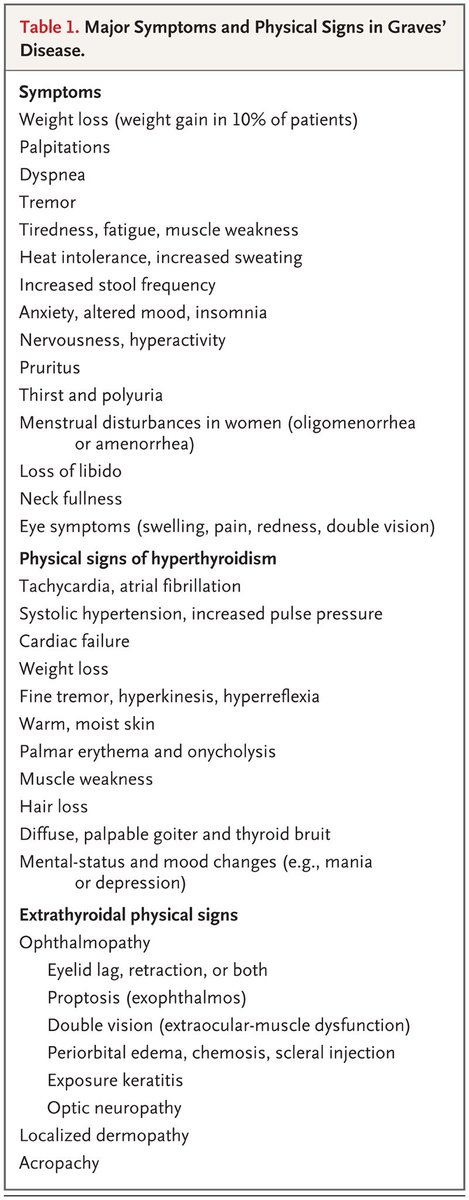
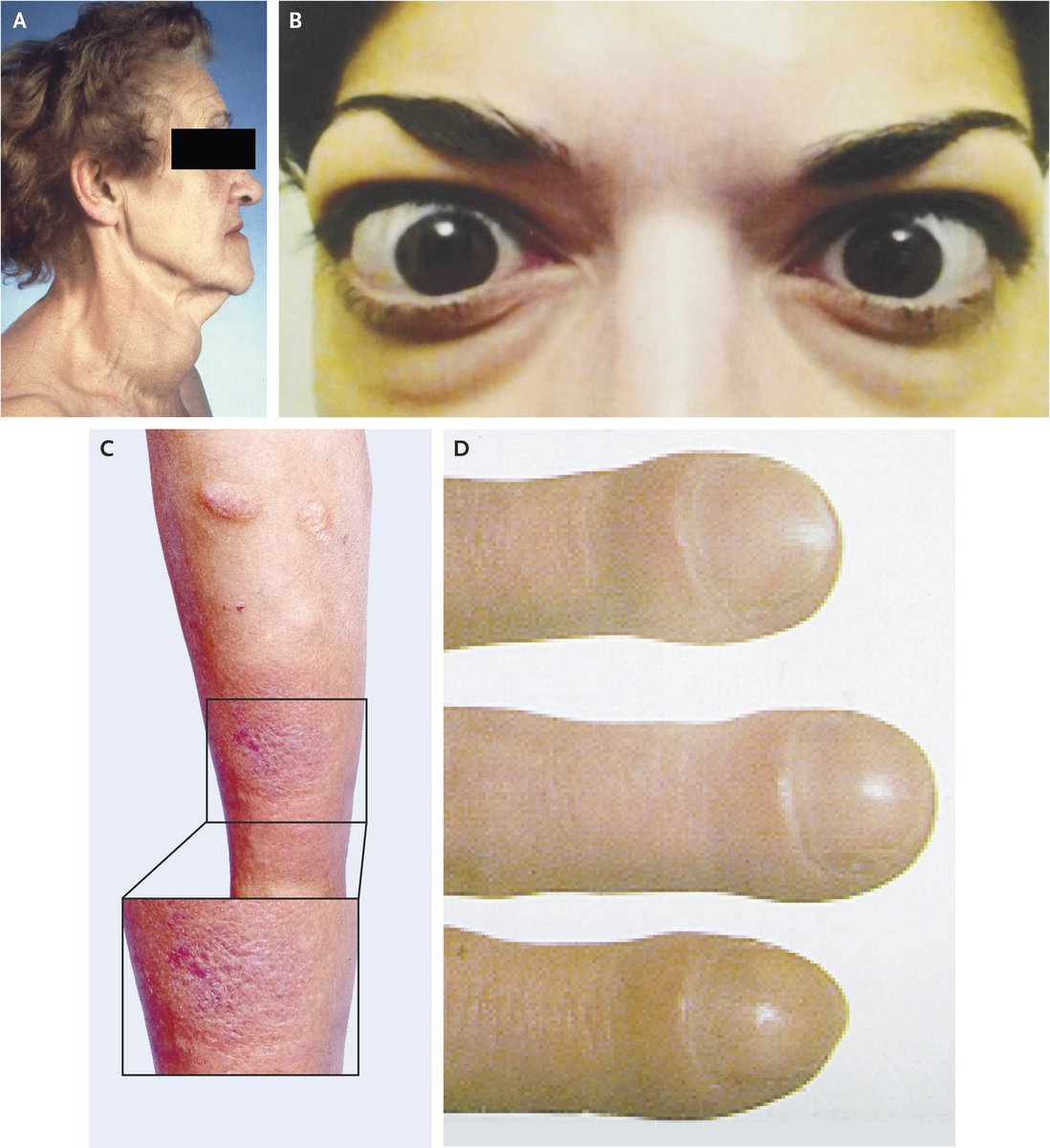
Graves' disease can show other physical signs including:
A. Diffusely enlarged, palpable thyroid gland (goiter)
B. Bilateral proptosis, periorbital edema, scleral injection
C. Pretibial dermopathy (myexdema)
D. Acropachy (dermopathy w/ hand swelling & nail clubbing)
[4, 5]
A. Diffusely enlarged, palpable thyroid gland (goiter)
B. Bilateral proptosis, periorbital edema, scleral injection
C. Pretibial dermopathy (myexdema)
D. Acropachy (dermopathy w/ hand swelling & nail clubbing)
[4, 5]


While first-line testing for Graves' disease is based on TSH (⬇️), free T4 (⬆️), & total T3 (⬆️), essential next step tests:
-Thyroid receptor autoantibodies (TRAbs): TSI & TBII
TSI = thyroid-stimulating immunoglobulin
TBII = thyrotropin-binding inhibitory immunoglobulin
[6]
-Thyroid receptor autoantibodies (TRAbs): TSI & TBII
TSI = thyroid-stimulating immunoglobulin
TBII = thyrotropin-binding inhibitory immunoglobulin
[6]
Finally, we arrive at the radioactive iodine uptake (RAIU) test. Phew!
While RAIUs used to be used more often, they can still be helpful for diagnosing different forms of hyperthyroidism
Note that RAIUs are *diagnostic*, whereas radioiodine ablations are used for *treatment*
While RAIUs used to be used more often, they can still be helpful for diagnosing different forms of hyperthyroidism
Note that RAIUs are *diagnostic*, whereas radioiodine ablations are used for *treatment*

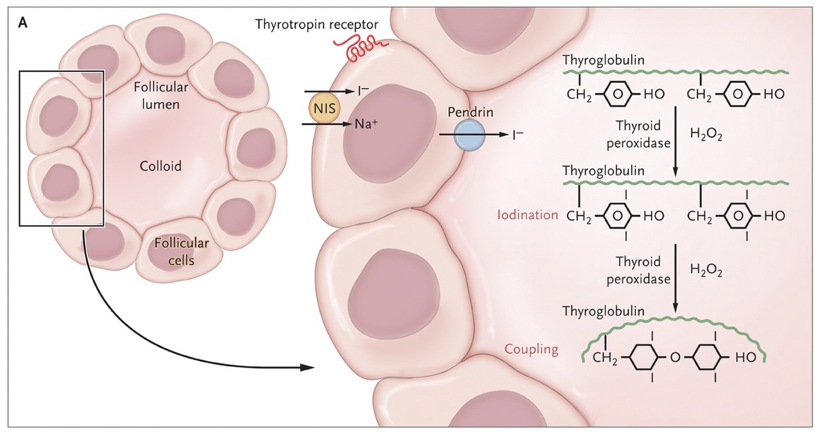
Iodine is actively transported into thyroid follicular cells by the Na-I symporter (NIS)
Radioiodine (I-123 or I-131) is taken up by the thyroid via NIS
Patients must fast for ~8 hrs prior, ingest radioiodine & then RAIU is typically read several hours (4-6 & 24) later
[7]
Radioiodine (I-123 or I-131) is taken up by the thyroid via NIS
Patients must fast for ~8 hrs prior, ingest radioiodine & then RAIU is typically read several hours (4-6 & 24) later
[7]
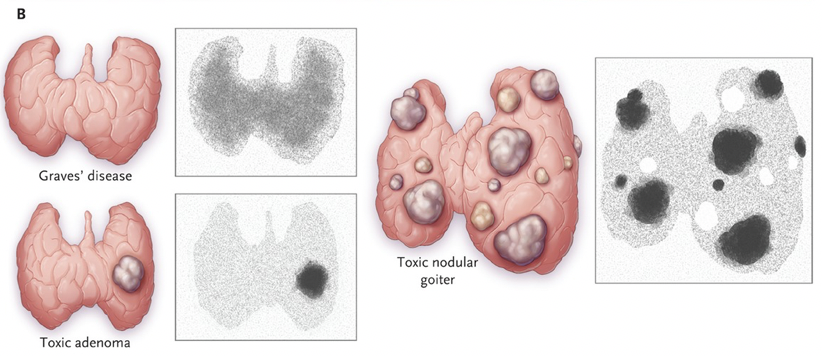
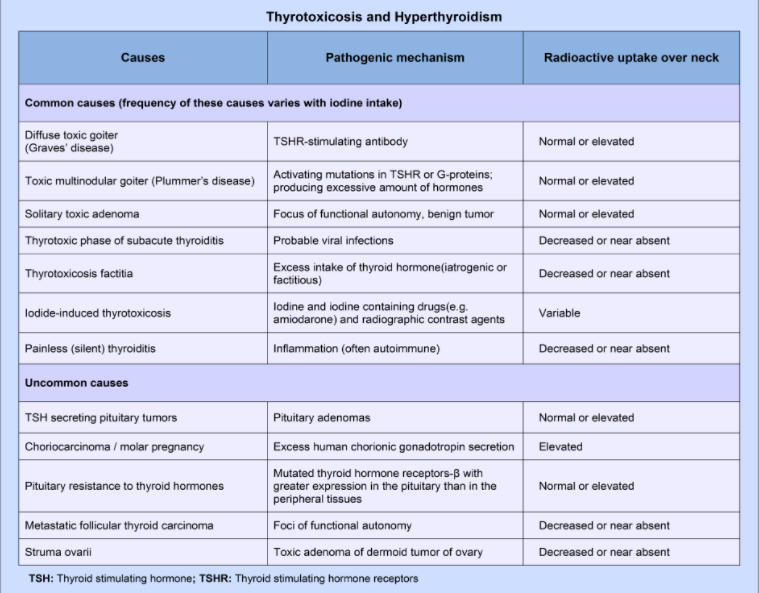
Possible RAIU outcomes:
1⃣Diffuse uptake -> Graves' disease
2⃣Diffuse nodularity -> Toxic multinodular goiter
3⃣Discrete "hot" nodule -> Solitary toxic adenoma
4⃣Low or absent -> thyrotoxic phase of subacute thyroiditis ("spilling out hormone"), *painful* thyroid
[7, 8, 9]
1⃣Diffuse uptake -> Graves' disease
2⃣Diffuse nodularity -> Toxic multinodular goiter
3⃣Discrete "hot" nodule -> Solitary toxic adenoma
4⃣Low or absent -> thyrotoxic phase of subacute thyroiditis ("spilling out hormone"), *painful* thyroid
[7, 8, 9]

I'm afraid we've reached the end of this #tweetorial!
If you want more:
-Listen to our Hyperthyroidism episode: apple.co
-Then take this NEJM practice question on hyperthyroidism management: knowledgeplus.nejm.org
-NEJM Case 10-2015: nejm.org
If you want more:
-Listen to our Hyperthyroidism episode: apple.co
-Then take this NEJM practice question on hyperthyroidism management: knowledgeplus.nejm.org
-NEJM Case 10-2015: nejm.org
Tweetorial references:
[1] mdedge.com
[2] basicmedicalkey.com
[3] wikem.org
[4] nejm.org
[5] nejm.org
[6] slideplayer.com
[7] nejm.org
[8] traumayellow.com
[9] nucradshare.com
[1] mdedge.com
[2] basicmedicalkey.com
[3] wikem.org
[4] nejm.org
[5] nejm.org
[6] slideplayer.com
[7] nejm.org
[8] traumayellow.com
[9] nucradshare.com
basicmedicalkey.com/alterations-of…
traumayellow.com/em-education/h…
nejm.org/doi/full/10.10…
mdedge.com/clinicianrevie…
nucradshare.com/Thyroid.html
nejm.org/doi/full/10.10…
Graves' Ophthalmopathy | NEJM
Review Article from The New England Journal of Medicine — Graves' Ophthalmopathy
slideplayer.com/slide/7380374/
wikem.org/wiki/Thyroid_d…
nejm.org/doi/full/10.10…
Loading suggestions...