

Handout from our Endocrinology episode, "Episode 33: Hypercalcemia" with Dr. OP Hamnvik @ohamnvik is now out!
📝Download it free here: #hypercalcemia" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
🎶Episode: apple.co
check out👇for a #tweetorial on PTH-dependent & PTH-independent causes of hyperCa
📝Download it free here: #hypercalcemia" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
🎶Episode: apple.co
check out👇for a #tweetorial on PTH-dependent & PTH-independent causes of hyperCa
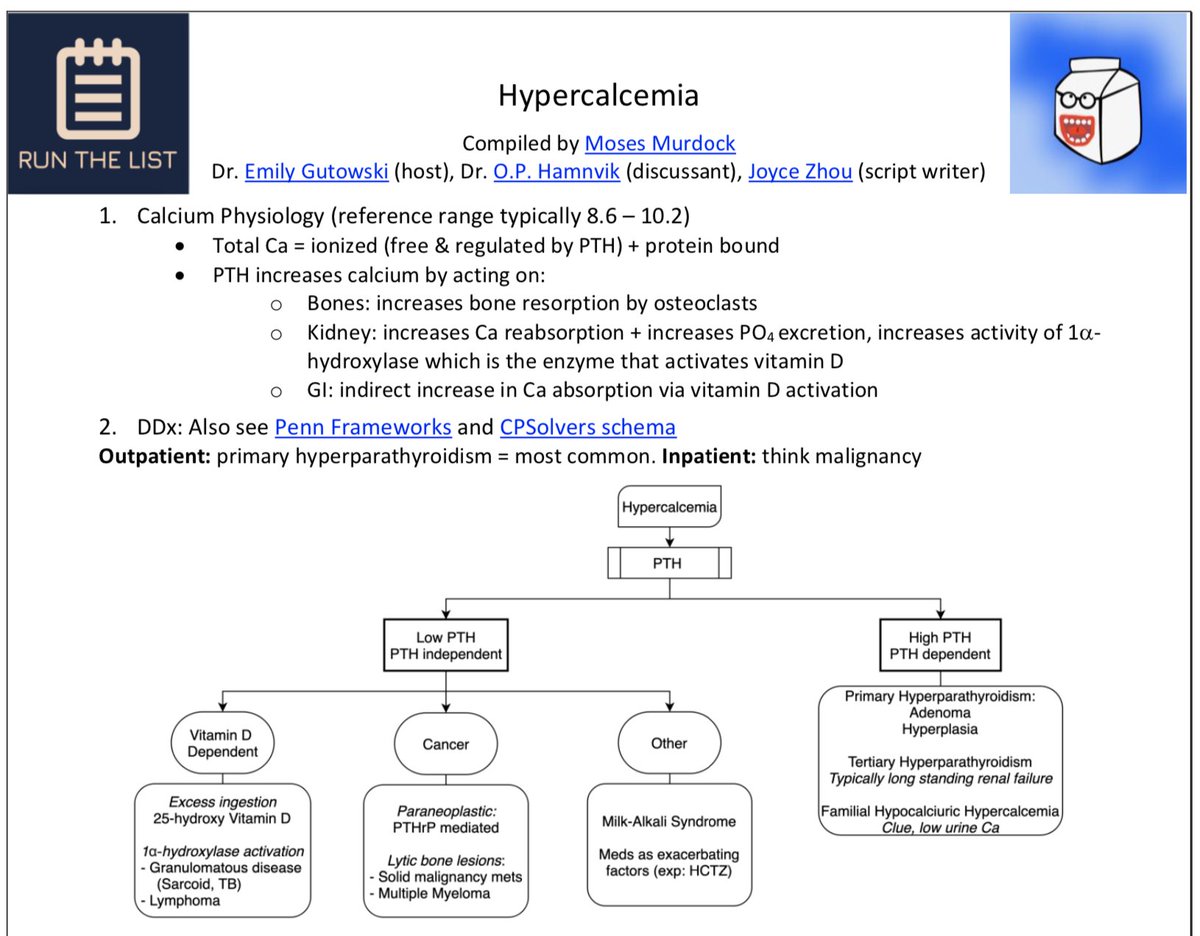
First things first, calcium is *tightly* regulated in the bloodstream (nl = 8.6 - 10.2 mg/dL)
TOTAL calcium exists mainly in two forms:
1⃣Ionized = FREE fraction
+
2⃣Bound to protein (albumin)
*note that the FREE/ionized fraction is what controls parathyroid hormone (PTH)
[1]
TOTAL calcium exists mainly in two forms:
1⃣Ionized = FREE fraction
+
2⃣Bound to protein (albumin)
*note that the FREE/ionized fraction is what controls parathyroid hormone (PTH)
[1]

Now that we know that free/ionized Ca = PTH thermostat, how is it sensed?
Parathyroid glands (which sit beside/"para" to the thyroid gland) express the Calcium-sensing receptor (CaSR) on the surface of *Chief cells*
CaSR = G-protein coupled receptor (GPCR) "calciostat"
[2,3]
Parathyroid glands (which sit beside/"para" to the thyroid gland) express the Calcium-sensing receptor (CaSR) on the surface of *Chief cells*
CaSR = G-protein coupled receptor (GPCR) "calciostat"
[2,3]



when Ca levels = ⬇️ -> PTH release ⬆️
when Ca levels = ⬆️ -> PTH release ⬇️
this is because elevated Ca is sensed by the CaSR --> suppressing release of PTH from Chief cells
(remember that Ca must be tightly regulated as it's an essential 2nd messenger intracellularly!)
[4]
when Ca levels = ⬆️ -> PTH release ⬇️
this is because elevated Ca is sensed by the CaSR --> suppressing release of PTH from Chief cells
(remember that Ca must be tightly regulated as it's an essential 2nd messenger intracellularly!)
[4]

knowing how CaSR works is *critical* to understanding calcium homeostasis & rare diseases like Familial Hypocalciuric Hypercalcemia (FHH)
FHH = autosomal dominant loss-of-function (LoF) mutation in CaSR
FHH's name tells you disease sequelae:
1⃣Hypocalciuria
2⃣Hypercalcemia
[5]
FHH = autosomal dominant loss-of-function (LoF) mutation in CaSR
FHH's name tells you disease sequelae:
1⃣Hypocalciuria
2⃣Hypercalcemia
[5]

LoF in CaSR -> ⬇️ability to sense Ca
as a result, calciostat (CaSR) is at a higher "setpoint"*
thus, ⬆️PTH ("inappropriately normal") -> ⬆️Ca via bone resorption & ⬆️Ca reabsorption via the kidney (see below) -> hypercalcemia & hypocalciuria
*really running w/ analogy here...
as a result, calciostat (CaSR) is at a higher "setpoint"*
thus, ⬆️PTH ("inappropriately normal") -> ⬆️Ca via bone resorption & ⬆️Ca reabsorption via the kidney (see below) -> hypercalcemia & hypocalciuria
*really running w/ analogy here...
PTH has several functions:
1⃣Bones: PTH binds its receptor (PTH1R) -> ⬆️RANK-L, which binds to RANK on osteoclasts -> ⬆️Ca through bone resorption
2⃣Kidney: PTH binds PTH1R -> ⬆️Ca reabsorption (via TRPV5,6 channel) & ⬆️PTH excretion*
*PTH = "Phosphate-TRASHING Hormone"
[6]
1⃣Bones: PTH binds its receptor (PTH1R) -> ⬆️RANK-L, which binds to RANK on osteoclasts -> ⬆️Ca through bone resorption
2⃣Kidney: PTH binds PTH1R -> ⬆️Ca reabsorption (via TRPV5,6 channel) & ⬆️PTH excretion*
*PTH = "Phosphate-TRASHING Hormone"
[6]

(Kidney cont.) PTH also ⬆️ 25-hydroxyvitamin D 1-α-hydroxylase enzyme (CYP27B1)
1-α-hydroxylase converts 25-hydroxyvitamin D ➡️ active 1,25-dihydroxyvitamin D (calcitriol)
this brings us to 👇
[7]
1-α-hydroxylase converts 25-hydroxyvitamin D ➡️ active 1,25-dihydroxyvitamin D (calcitriol)
this brings us to 👇
[7]
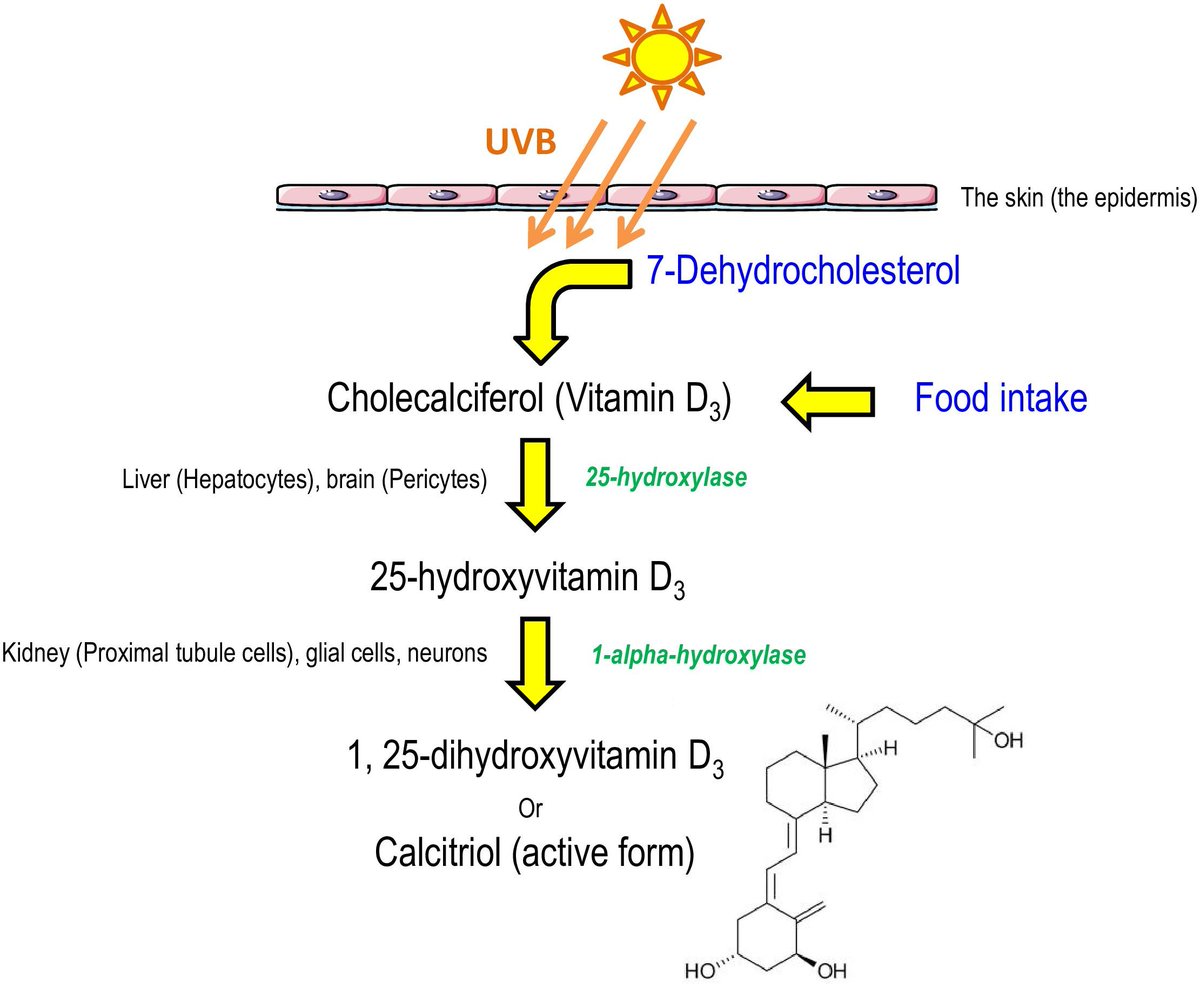
3⃣GI tract: PTH now *indirectly* promotes Ca reabsorption via calcitriol (1,25(OH)2D), which binds to the vitamin D receptor (VDR) in enterocytes -> ⬆️ Ca uptake from the diet via TRPV6 channel, among other effects
🔑overall, PTH -> ⬆️Ca, ⬇️Phos
[8]
🔑overall, PTH -> ⬆️Ca, ⬇️Phos
[8]

Finally, we arrive at the causes of hypercalcemia
@ohamnvik teaches us to think in TWO major buckets:
1⃣PTH-dependent
2⃣PTH-independent
@haematognomist made this nice framework 👇
2 more frameworks @PennMedicine & @CPSolvers: med.upenn.edu
clinicalproblemsolving.com
@ohamnvik teaches us to think in TWO major buckets:
1⃣PTH-dependent
2⃣PTH-independent
@haematognomist made this nice framework 👇
2 more frameworks @PennMedicine & @CPSolvers: med.upenn.edu
clinicalproblemsolving.com
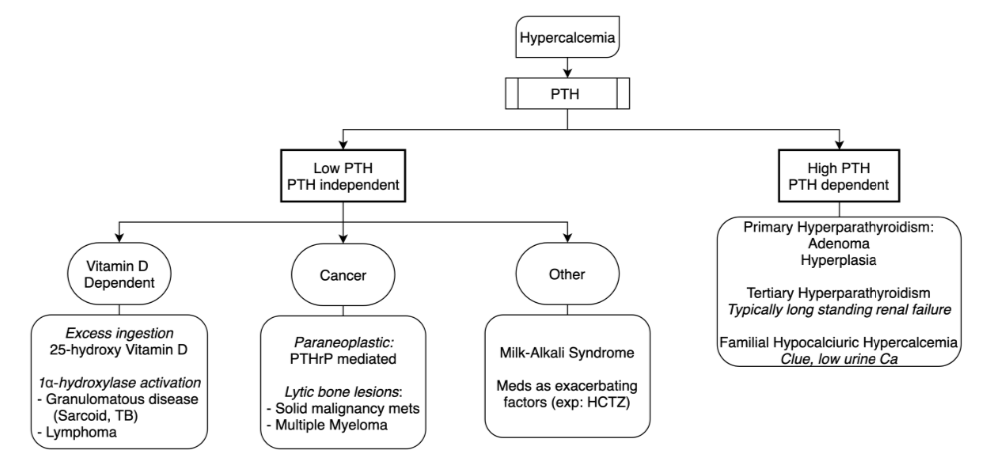
Let's start by breaking down PTH-dependent causes of hyperCa:
PRIMARY hyperparathyroidism, PTH is⬆️
Causes:
1⃣Parathyroid adenoma, hyperplasia, carcinoma
2⃣Multiple endocrine neoplasia (MEN) 1, 2A
3⃣FHH
-
TERTIARY hyperparathyroidism, PTH is⬆️⬆️
Cause:
1⃣Chronic renal failure
PRIMARY hyperparathyroidism, PTH is⬆️
Causes:
1⃣Parathyroid adenoma, hyperplasia, carcinoma
2⃣Multiple endocrine neoplasia (MEN) 1, 2A
3⃣FHH
-
TERTIARY hyperparathyroidism, PTH is⬆️⬆️
Cause:
1⃣Chronic renal failure


PTH-independent causes of hyperCa:
CANCER:
-Paraneoplastic (via PTH-related peptide = PTHrP)
⬆️PTHrP: squamous cell carcinoma of lung, carcinomas of breast, renal, bladder, ovary
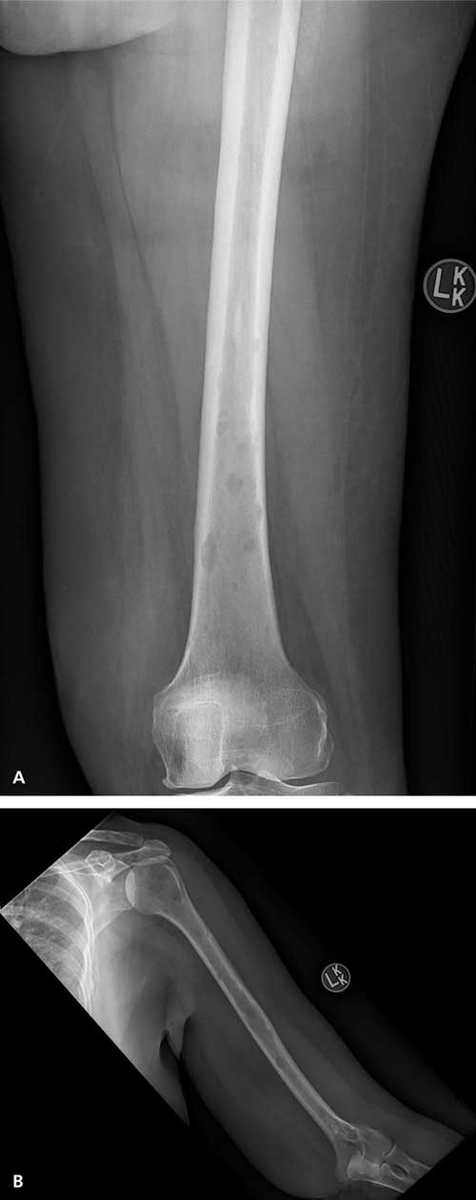
-Lytic bone lesions (Multiple myeloma, Adult T-cell lymphoma)
[9]
CANCER:
-Paraneoplastic (via PTH-related peptide = PTHrP)
⬆️PTHrP: squamous cell carcinoma of lung, carcinomas of breast, renal, bladder, ovary
-Lytic bone lesions (Multiple myeloma, Adult T-cell lymphoma)
[9]

VITAMIN D:
-Hypervitaminosis D (vit. D excess/intoxication)
-1-α-hydroxylase activity in *Granulomatous diseases* (TB, sarcoid, histoplasmosis, GPA) & ectopic 1-α-hydroxylase in Lymphoma
OTHER:
-Ingestion of excess calcium (Milk Alkali syndrome, e.g. TUMS)
-Meds (e.g. HCTZ)
-Hypervitaminosis D (vit. D excess/intoxication)
-1-α-hydroxylase activity in *Granulomatous diseases* (TB, sarcoid, histoplasmosis, GPA) & ectopic 1-α-hydroxylase in Lymphoma
OTHER:
-Ingestion of excess calcium (Milk Alkali syndrome, e.g. TUMS)
-Meds (e.g. HCTZ)


[*Spoiler alert*]
for more on TUMS-induced hypercalcemia (i.e. Milk Alkali Syndrome) check out Episode 79 from our friends at @CPSolvers & case presenter @AnandJag1:
clinicalproblemsolving.com
for more on TUMS-induced hypercalcemia (i.e. Milk Alkali Syndrome) check out Episode 79 from our friends at @CPSolvers & case presenter @AnandJag1:
clinicalproblemsolving.com
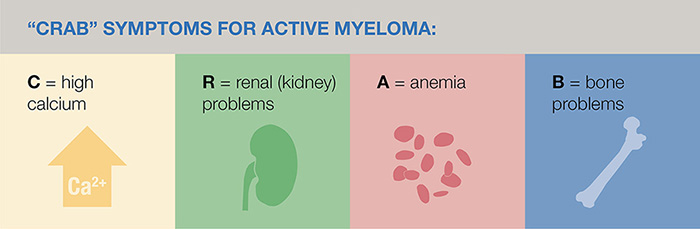
reminder that in Multiple Myeloma the "C" in CRAB criteria = hyperCalcemia
hypercalcemia = secondary to the lytic bone lesions seen w/ MM
for more clinical practice w/ hyperCa in malignancy:
VMR 52 w/ @tmodarressi: clinicalproblemsolving.com
VMR 63: clinicalproblemsolving.com
[10]
hypercalcemia = secondary to the lytic bone lesions seen w/ MM
for more clinical practice w/ hyperCa in malignancy:
VMR 52 w/ @tmodarressi: clinicalproblemsolving.com
VMR 63: clinicalproblemsolving.com
[10]

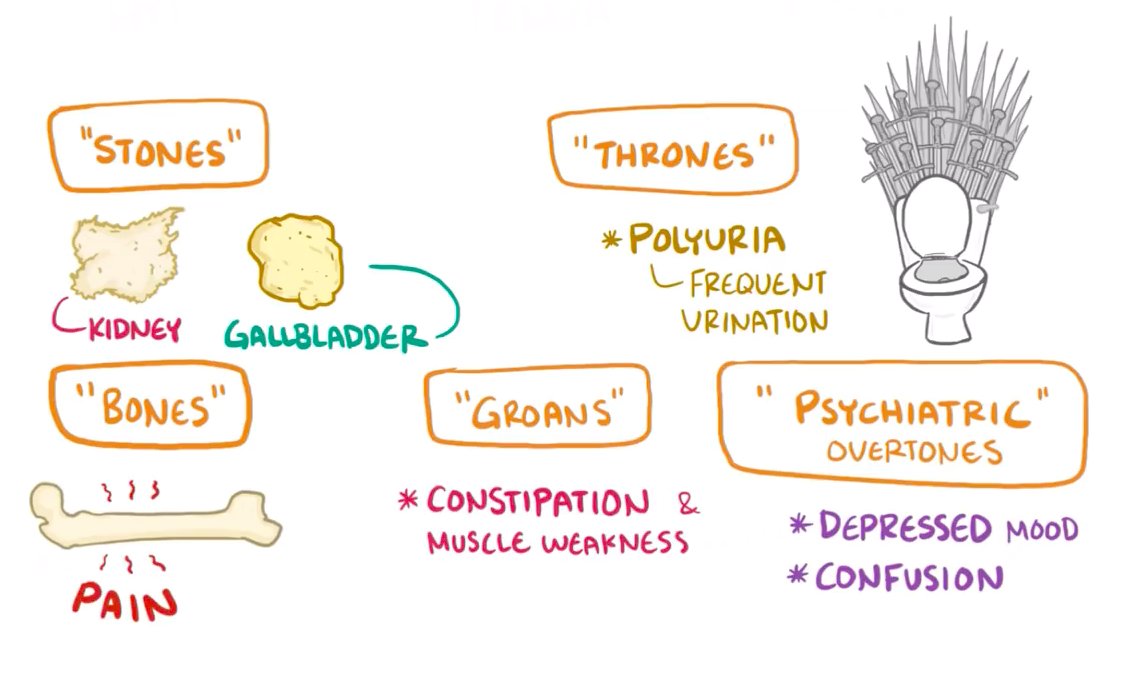
@ohamnvik reminds us that we can see hyperCa in the absence of any symptoms!
typically start to see sx at ~11.5 mg/dL, severe sx >13 mg/dL
Remember the "classic" hyperCa sx (see image👇)
*HyperCa can precipitate nephrogenic diabetes insipidus (NDI) -> polyuria, & pancreatitis
typically start to see sx at ~11.5 mg/dL, severe sx >13 mg/dL
Remember the "classic" hyperCa sx (see image👇)
*HyperCa can precipitate nephrogenic diabetes insipidus (NDI) -> polyuria, & pancreatitis
Alas, we're nearing the end... How about a quick quiz to test your knowledge?
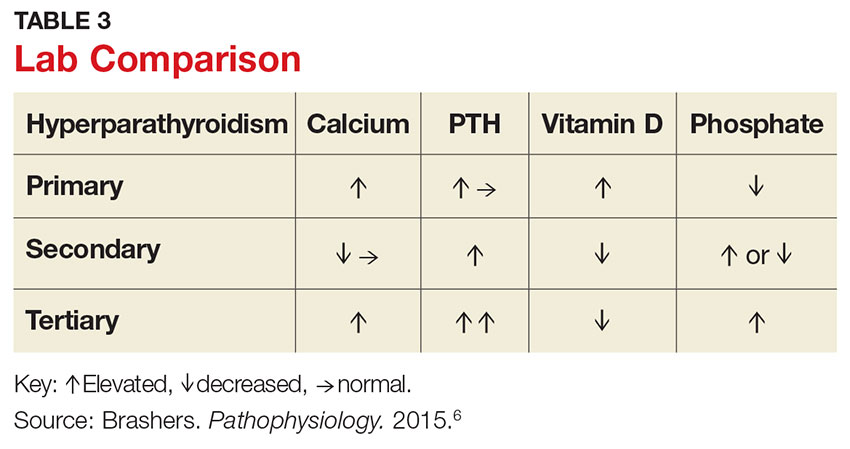
in PRIMARY hyperparathyroidism, what are the typical labs?
in PRIMARY hyperparathyroidism, what are the typical labs?
to recap:
Primary hyperparathyroidism: ⬆️/nl PTH, ⬆️Ca, ⬇️phos
Tertiary hyperparathyroidism: ⬆️⬆️ PTH, ⬆️Ca, ⬆️phos (due to ESRD)
mdedge.com
Primary hyperparathyroidism: ⬆️/nl PTH, ⬆️Ca, ⬇️phos
Tertiary hyperparathyroidism: ⬆️⬆️ PTH, ⬆️Ca, ⬆️phos (due to ESRD)
mdedge.com
For more on clinical presentation, management, case discussion, and other clinical pearls, be sure to check out Episode 33: Hypercalcemia with Dr. OP Hamnvik!
(sneak peek: he'll be back tomorrow for a Hypocalcemia episode!)
apple.co
(sneak peek: he'll be back tomorrow for a Hypocalcemia episode!)
apple.co

IN SUM:
-Ionized = "free" Ca, which controls PTH level
-Ca sensed in parathyroid Chief cells by CaSR
-CaSR LoF mut. -> FHH
-PTH -> ⬆️Ca, ⬆️active vit. D, ⬇️phos
-HyperCa causes: PTH-dependent (primary, tertiary) & -independent (cancer, vit. D, other)
#hypercalcemia" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
-Ionized = "free" Ca, which controls PTH level
-Ca sensed in parathyroid Chief cells by CaSR
-CaSR LoF mut. -> FHH
-PTH -> ⬆️Ca, ⬆️active vit. D, ⬇️phos
-HyperCa causes: PTH-dependent (primary, tertiary) & -independent (cancer, vit. D, other)
#hypercalcemia" target="_blank" rel="noopener" onclick="event.stopPropagation()">runthelistpodcast.com
REFs:
[1]uclahealth.org
[2]nejm.org
[3]proteinatlas.org
[4]nature.com
[5]youtube.com
[6]nature.com
[7]frontiersin.org
[8]sciencedirect.com
[9]jasn.asnjournals.org
10]aafp.org
[1]uclahealth.org
[2]nejm.org
[3]proteinatlas.org
[4]nature.com
[5]youtube.com
[6]nature.com
[7]frontiersin.org
[8]sciencedirect.com
[9]jasn.asnjournals.org
10]aafp.org
Loading suggestions...