

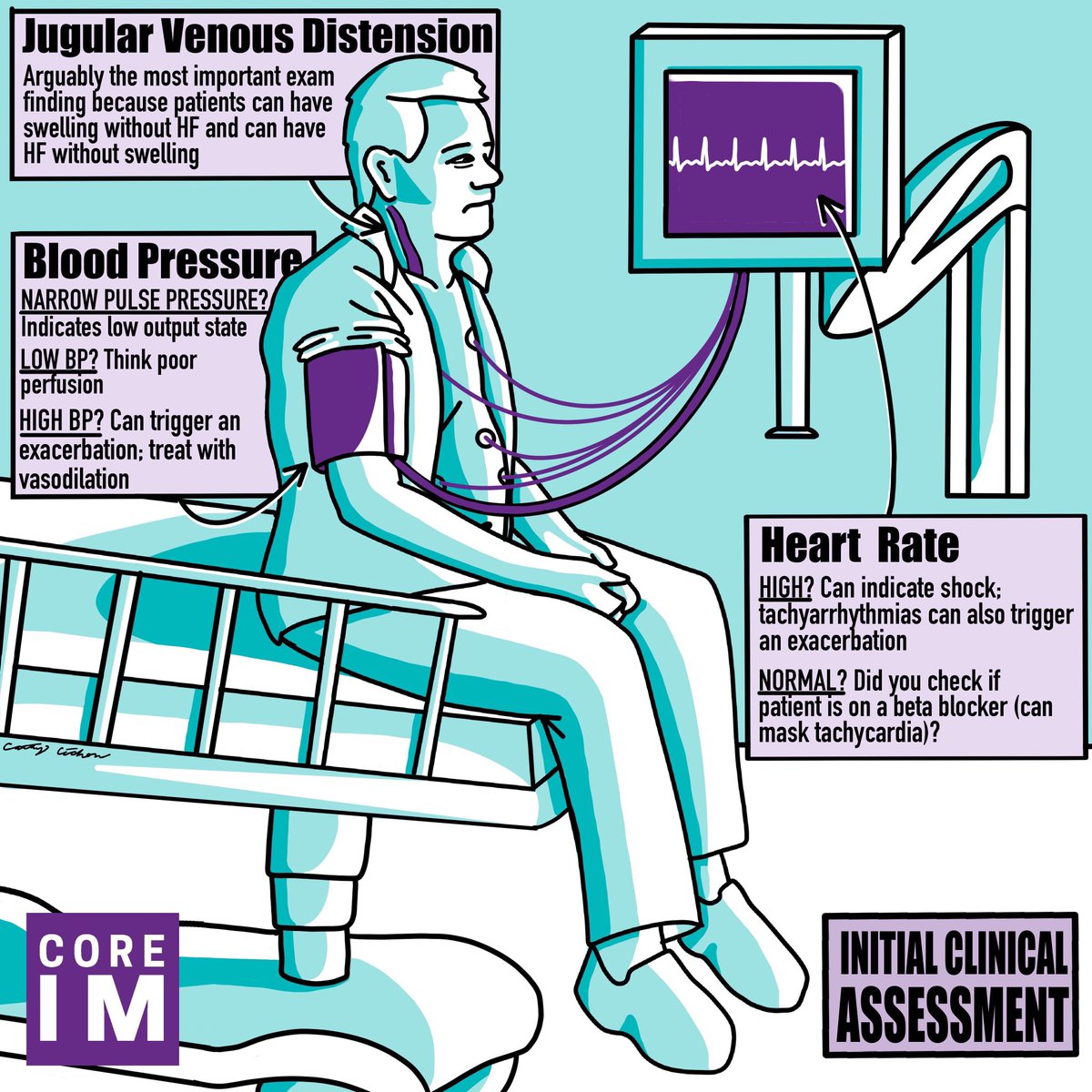
2/ Pearl #1: Initial Clinical Assessment
Are they dry or wet? Warm or cold?
Answers to these questions hinge on your exam and will drive treatment and triage.
Are they dry or wet? Warm or cold?
Answers to these questions hinge on your exam and will drive treatment and triage.
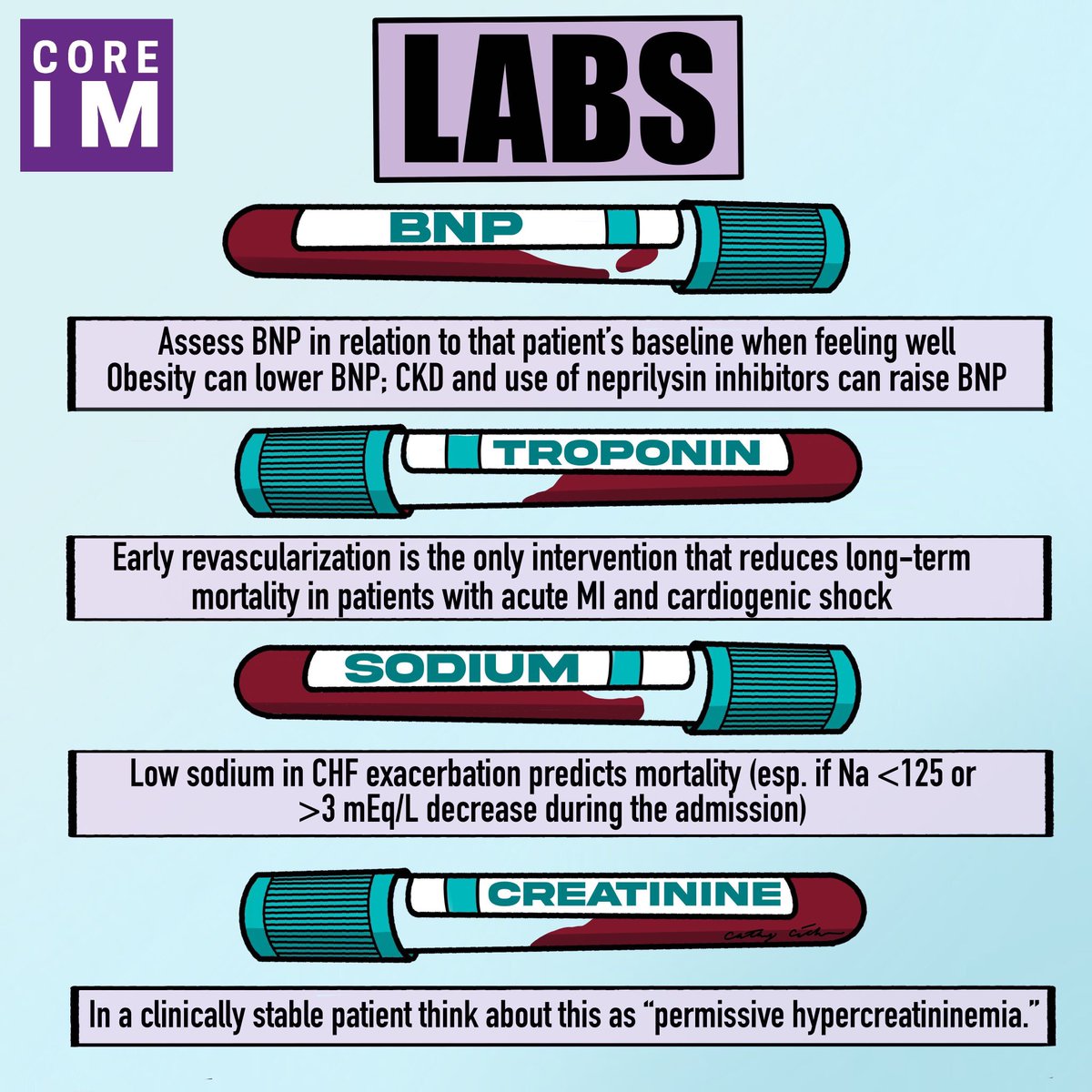
3/ Pearl #2: Initial Lab Workup
A retrospective study from the HARVEST registry found admission hyponatremia <135mEq/L was positively correlated with all-cause mortality, HR 1.43, 95% CI: 1.11-1.83.
A retrospective study from the HARVEST registry found admission hyponatremia <135mEq/L was positively correlated with all-cause mortality, HR 1.43, 95% CI: 1.11-1.83.
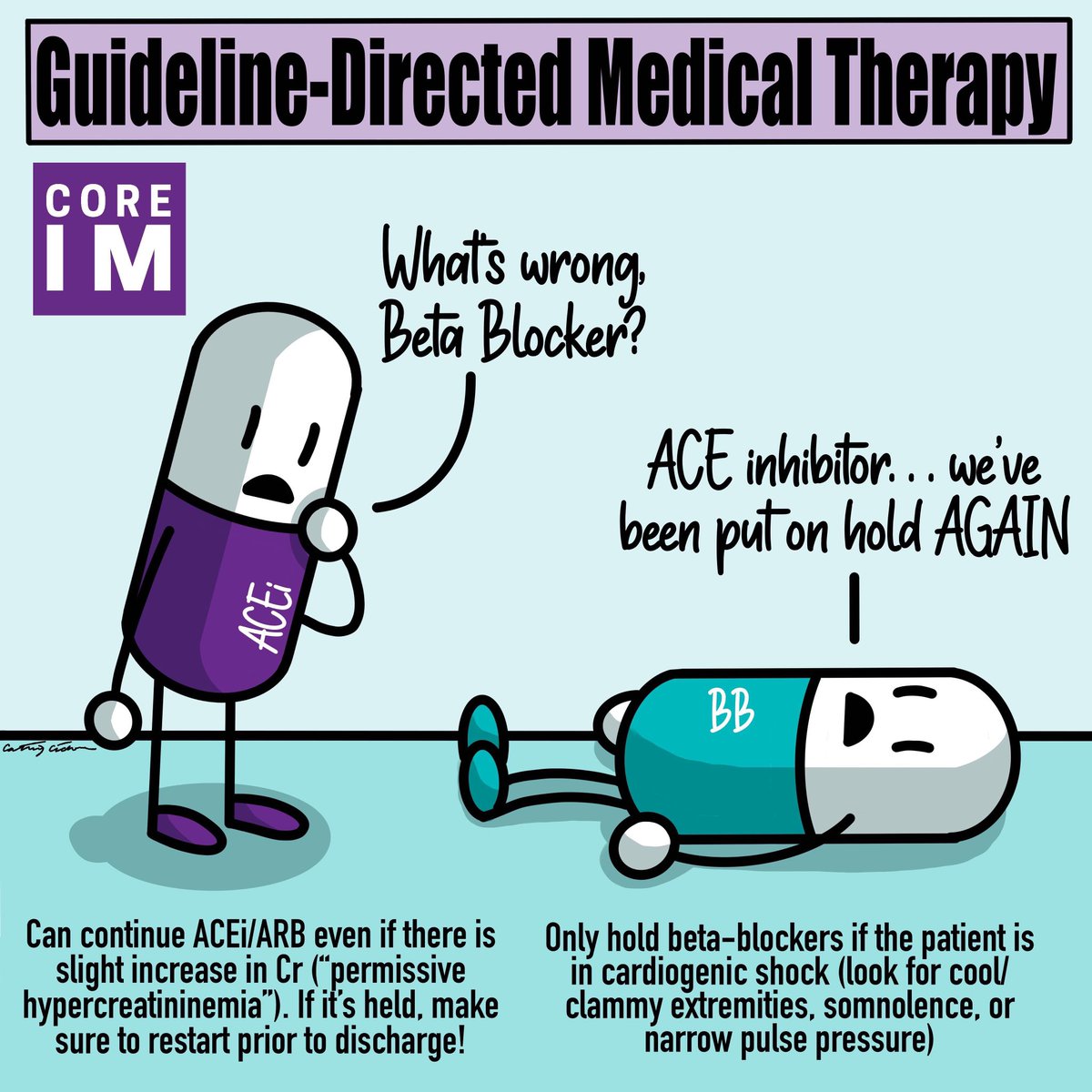
4/ Pearl #3: Home Meds
Only hold BB if pt is in shock. @hswapnil encourages you: be brave!
Consider keeping ACEi/ARB/ARNI/MRA on board during admission.
And if you stop any of these, make sure to restart them before discharge!
Only hold BB if pt is in shock. @hswapnil encourages you: be brave!
Consider keeping ACEi/ARB/ARNI/MRA on board during admission.
And if you stop any of these, make sure to restart them before discharge!
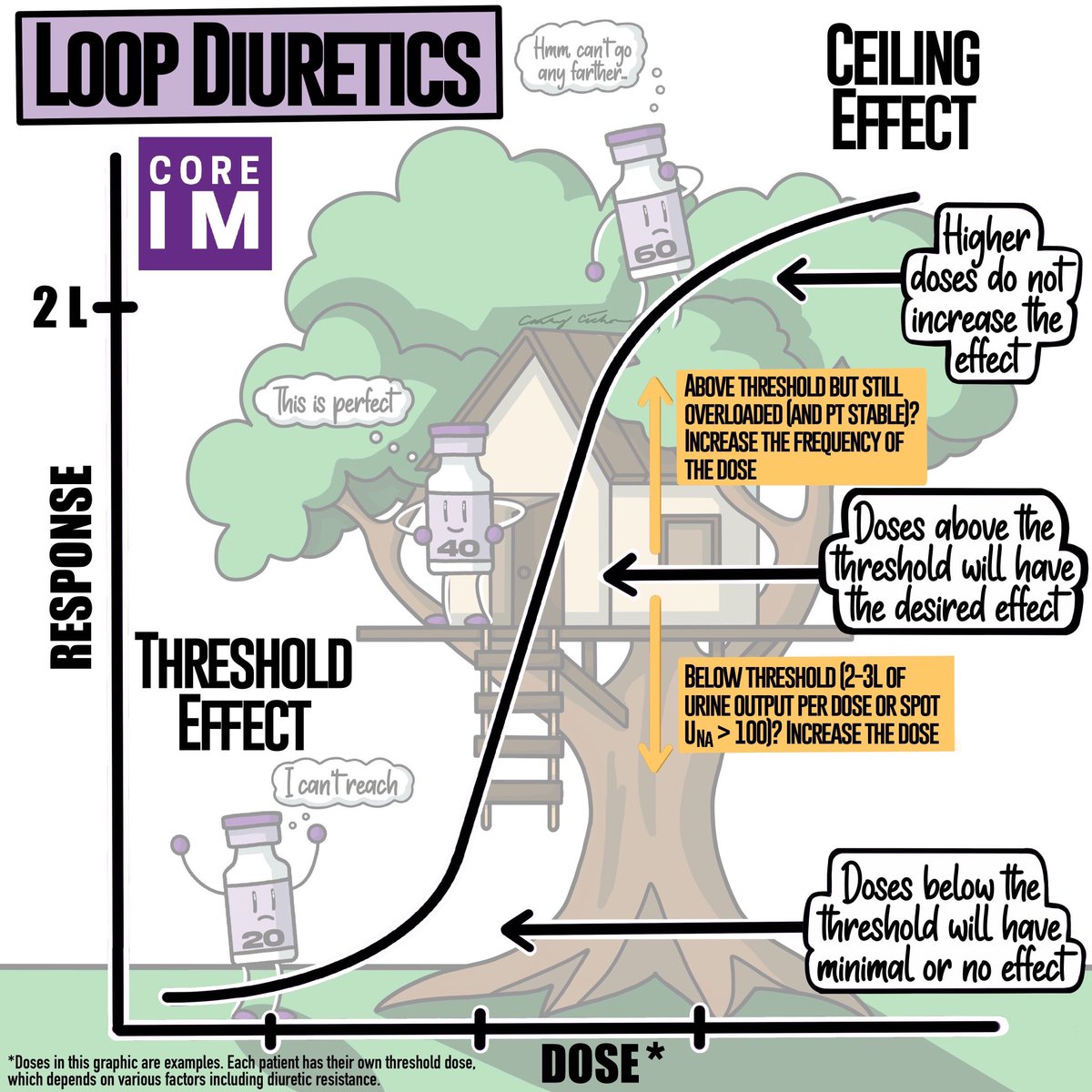
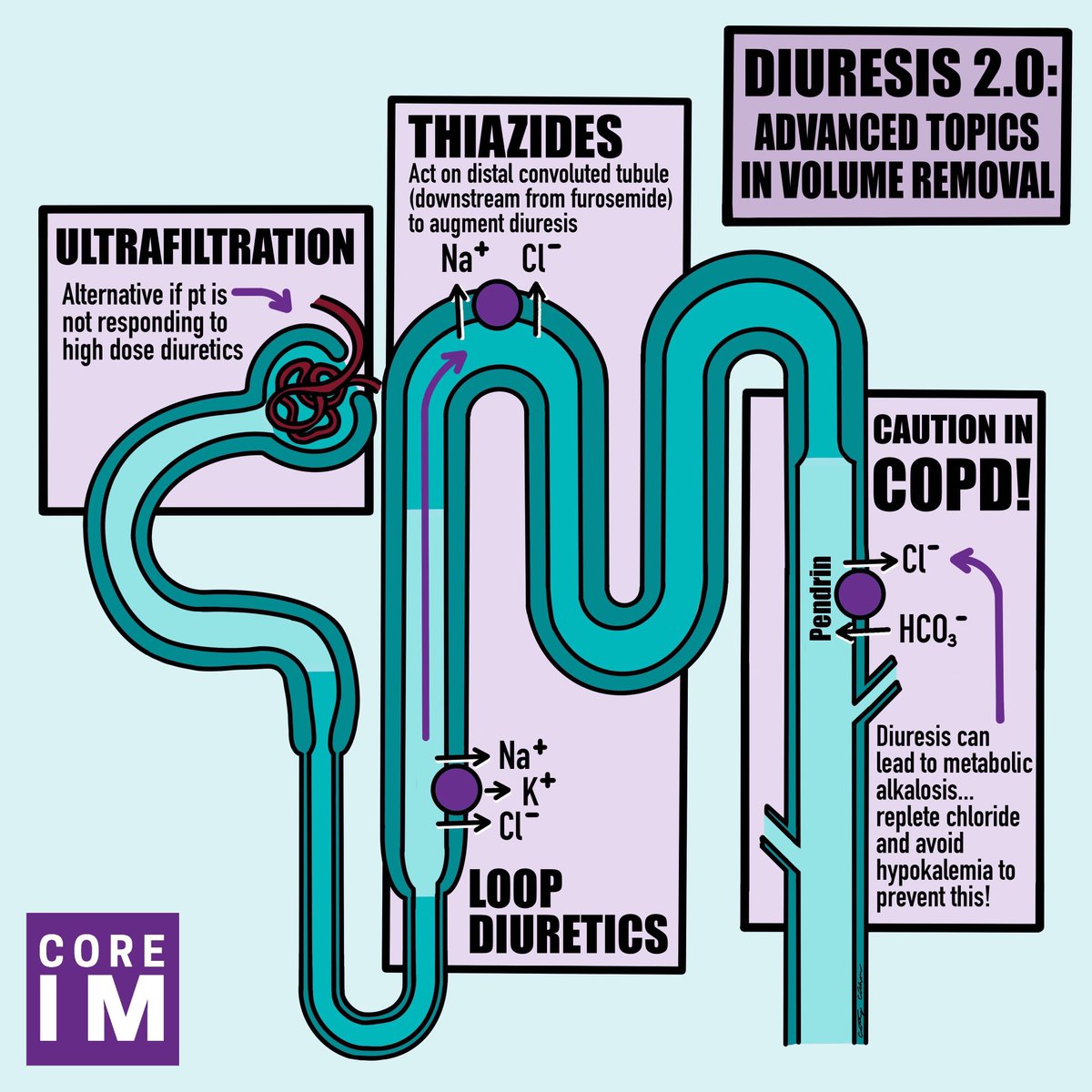
5/ Pearl #4: Loop diuretics
It’s all about thresholds and ceilings.
If you haven’t hit the threshold, your patient won’t pee enough. And once you reach the ceiling, bigger doses aren’t better - but more frequent doses will get your patient where they need to go.
It’s all about thresholds and ceilings.
If you haven’t hit the threshold, your patient won’t pee enough. And once you reach the ceiling, bigger doses aren’t better - but more frequent doses will get your patient where they need to go.
6/ Pearl #5: Additional Volume Removal
Metolazone: its long half-life makes daily dosing unnecessary.
In patients with comorbid COPD, look out for chloride depletion metabolic alkalosis leading to CO2 retention. Pesky pemdrin! Replete Cl with KCl or add spironolactone.
Metolazone: its long half-life makes daily dosing unnecessary.
In patients with comorbid COPD, look out for chloride depletion metabolic alkalosis leading to CO2 retention. Pesky pemdrin! Replete Cl with KCl or add spironolactone.
7/ Finally, raising this baby took a village and we have many folks to thank. Shout out to our cohost @MPDunleavy!
Huge ups to our guest experts: @gregorykatz @hswapnil @sargsyanz @MKIttlesonMD
And for the gorgeous graphics thanks go to @DocScribbles!
Huge ups to our guest experts: @gregorykatz @hswapnil @sargsyanz @MKIttlesonMD
And for the gorgeous graphics thanks go to @DocScribbles!
8/ Last shout out to our new audio editor @onlysolon that made everyone sound like gold and experimented with new music! We welcome any feedback 🙂
Loading suggestions...