
Avoiding airway catastrophe!
When things go sideways, don't be passive
How can we harness a team appropriately?
- @drlauraduggan at #HRreloaded
When things go sideways, don't be passive
How can we harness a team appropriately?
- @drlauraduggan at #HRreloaded


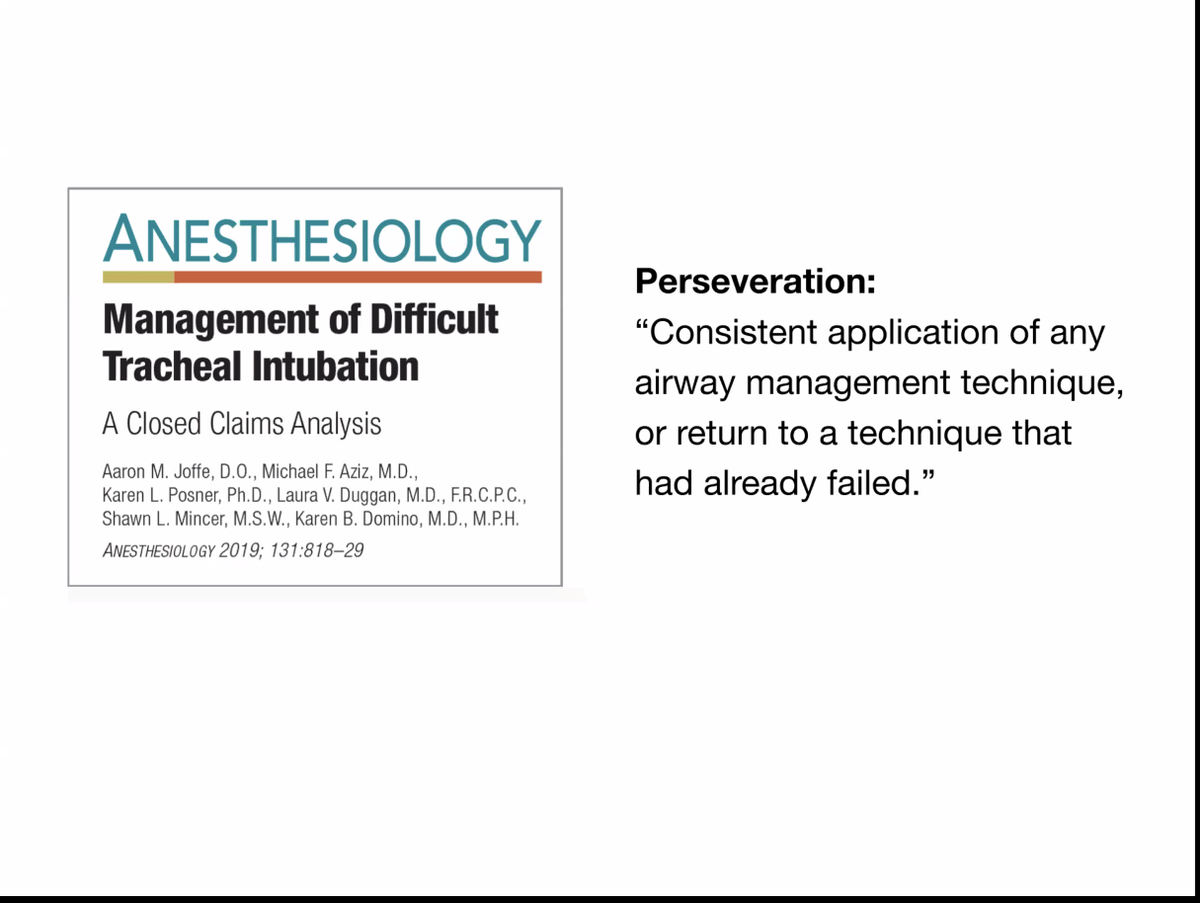
closed claims analysis: what patterns emerge?
10-12 teaching cases in the back are worth reading
- @drlauraduggan at #HRreloaded
10-12 teaching cases in the back are worth reading
- @drlauraduggan at #HRreloaded
30YO woman in plastic surgery office for breast augmentation. 40 minutes of attempts with laryngoscopy and bag-mask ventilation. cric performed after bradycardic and somehow pt did well. errors = lack of LMA, perseveration
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded

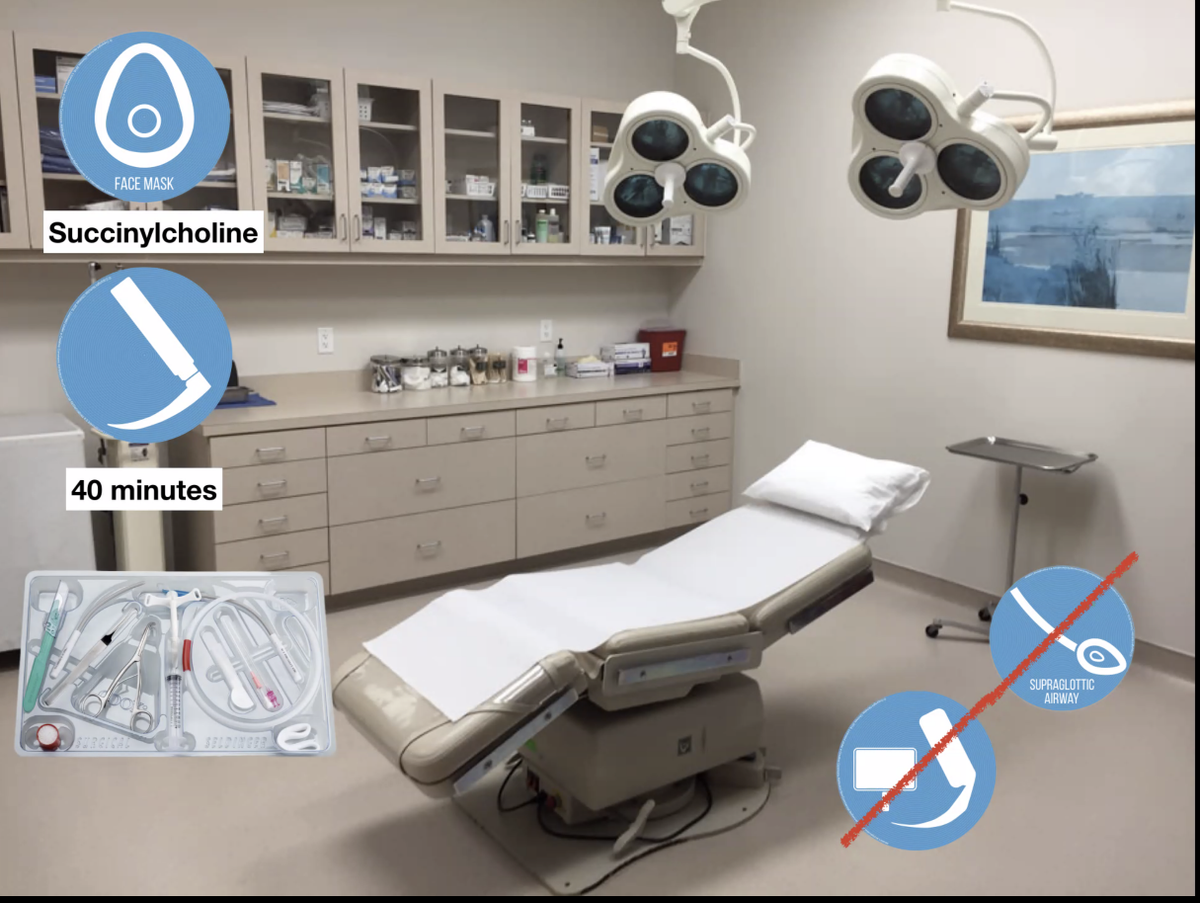
terrible outcomes often occur in elective anesthesia
- people not expecting badness
- inadequate preoxygenation
- hesitency to cric
- @drlauraduggan at #HRreloaded
- people not expecting badness
- inadequate preoxygenation
- hesitency to cric
- @drlauraduggan at #HRreloaded
if the provider is thinking "oh fuck oh fuck oh fuck" then that's a sign of perseveration. journal didn't allow her to add this bit.
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
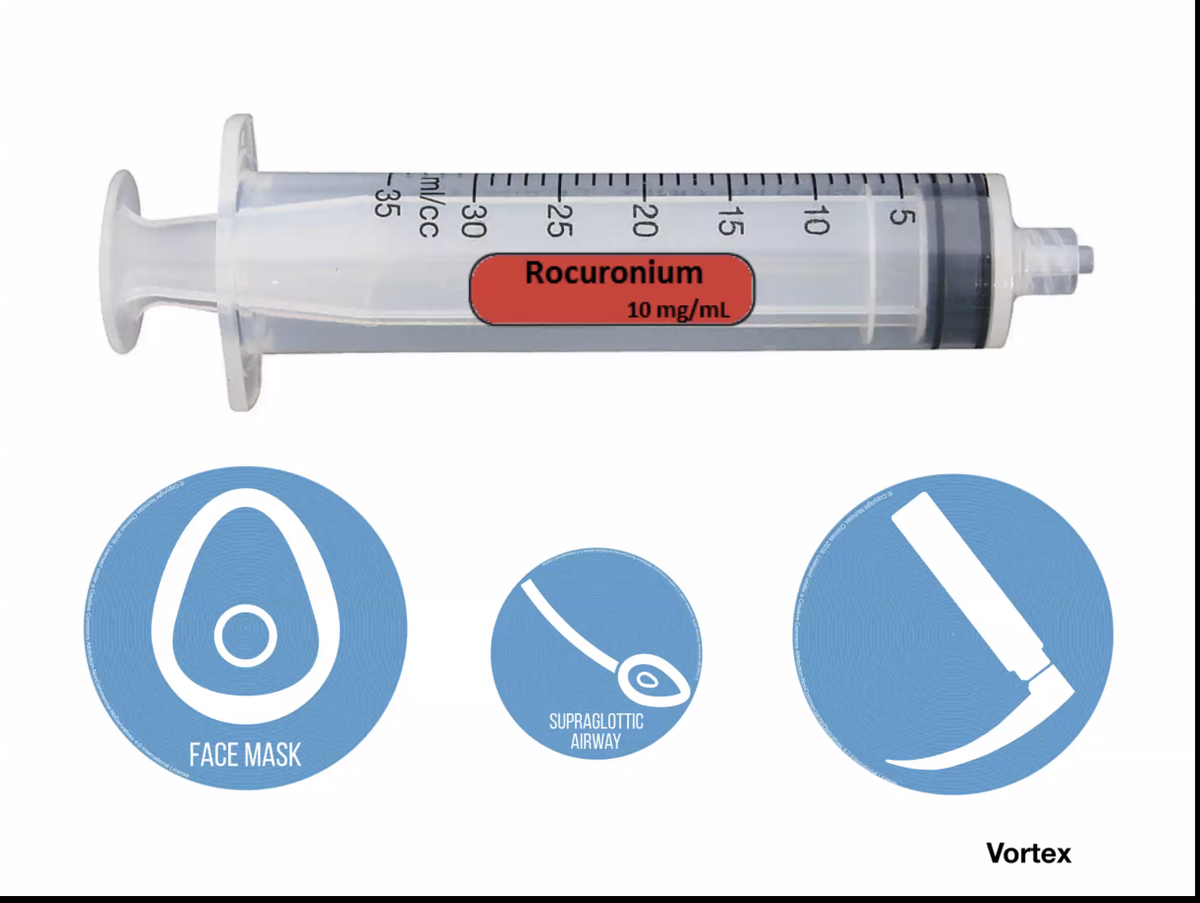
first attempt should be optimized as much as possible (it's not a "look"). long-acting paralytic is the best...
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
use roc and "burn the damn bridge down"
- improves supraglottic
- improves facemask ventilation
- improves intubation
- @drlauraduggan at #HRreloaded
- improves supraglottic
- improves facemask ventilation
- improves intubation
- @drlauraduggan at #HRreloaded

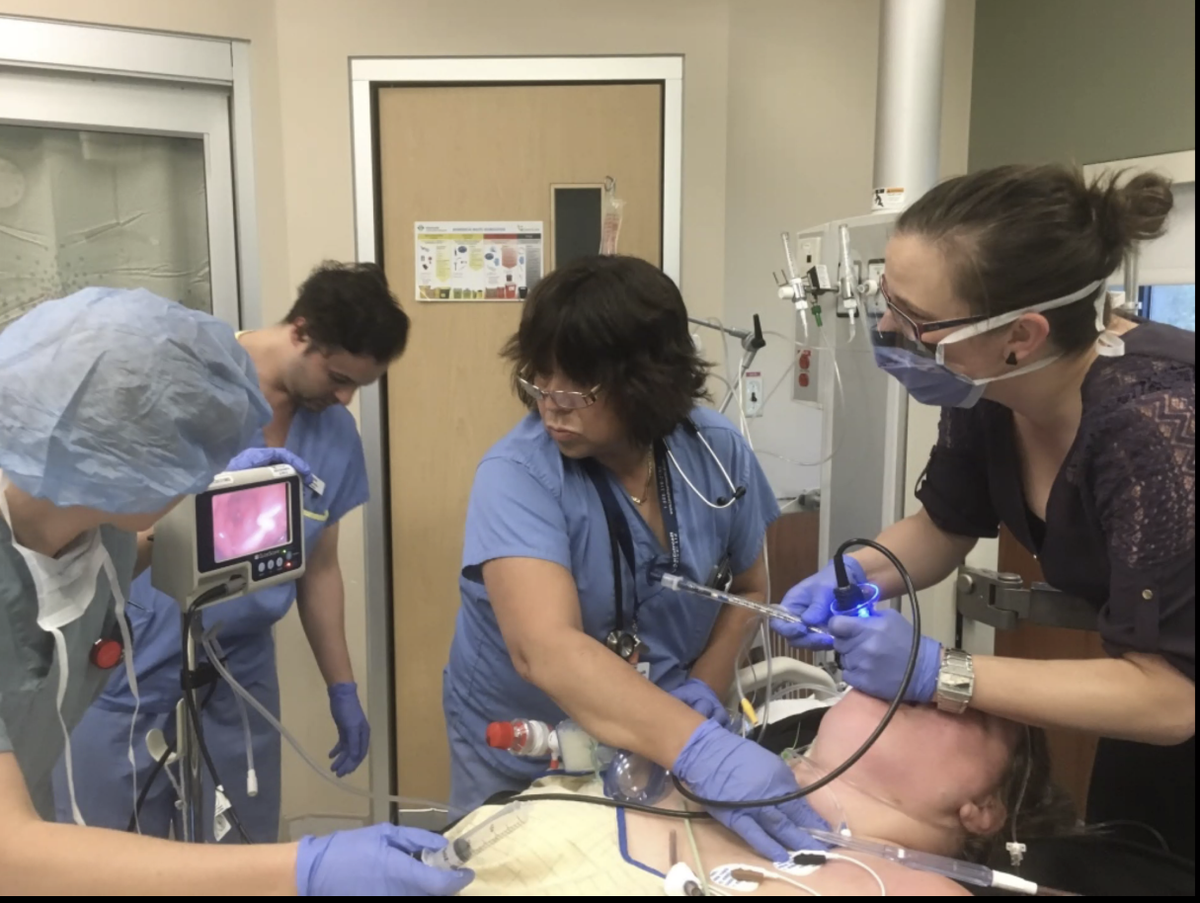
using video-laryngoscopy improves teamwork. people can tell what is going on and help you. do video-laryngoscopy on the first attempt
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
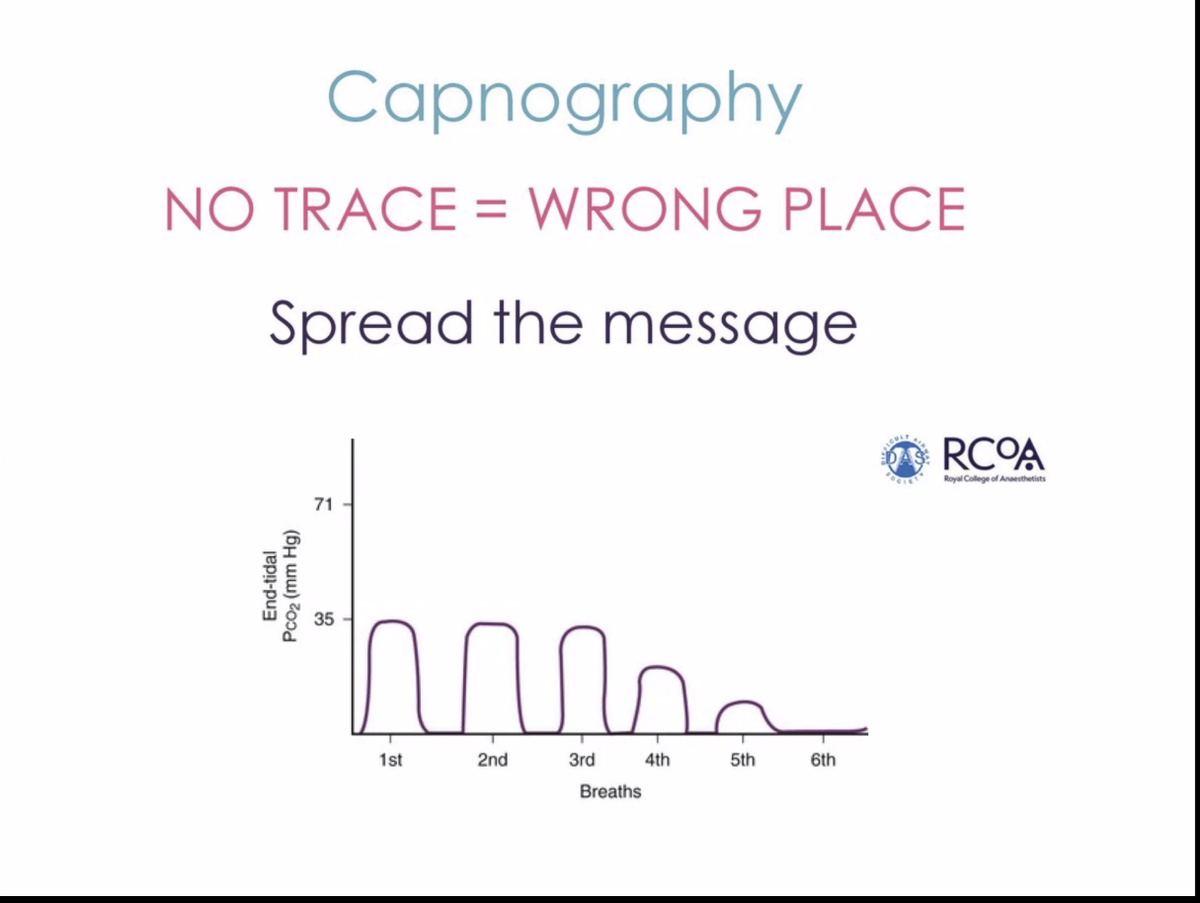
- waveform capnography should be used for every patient and for the entire duration of intubation.
- esophageal intubation: 6th tidal volume will dissapear
- no trace wrong place
- @drlauraduggan at #HRreloaded
- esophageal intubation: 6th tidal volume will dissapear
- no trace wrong place
- @drlauraduggan at #HRreloaded
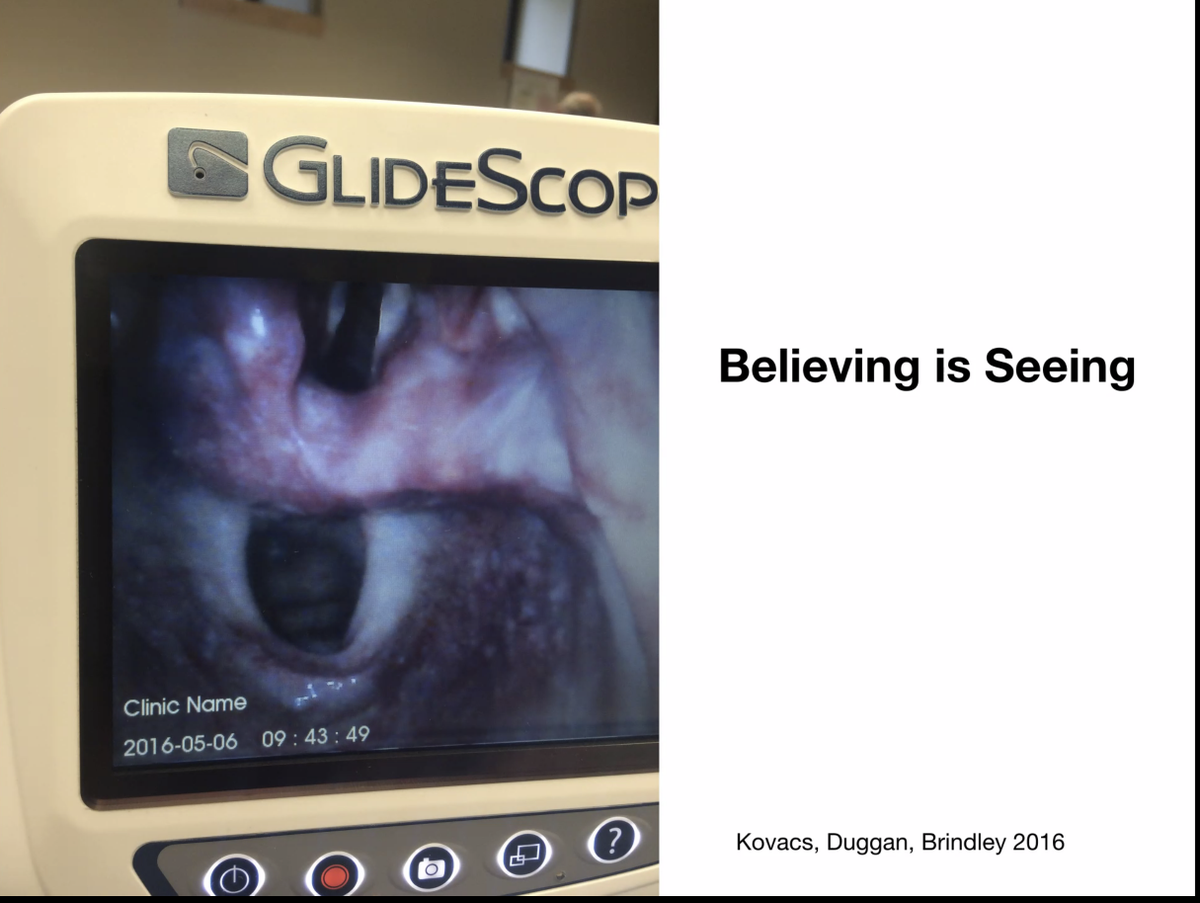
very experienced practitioners can be confused about where the ETT is going. esophagus can mimic the cords!
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
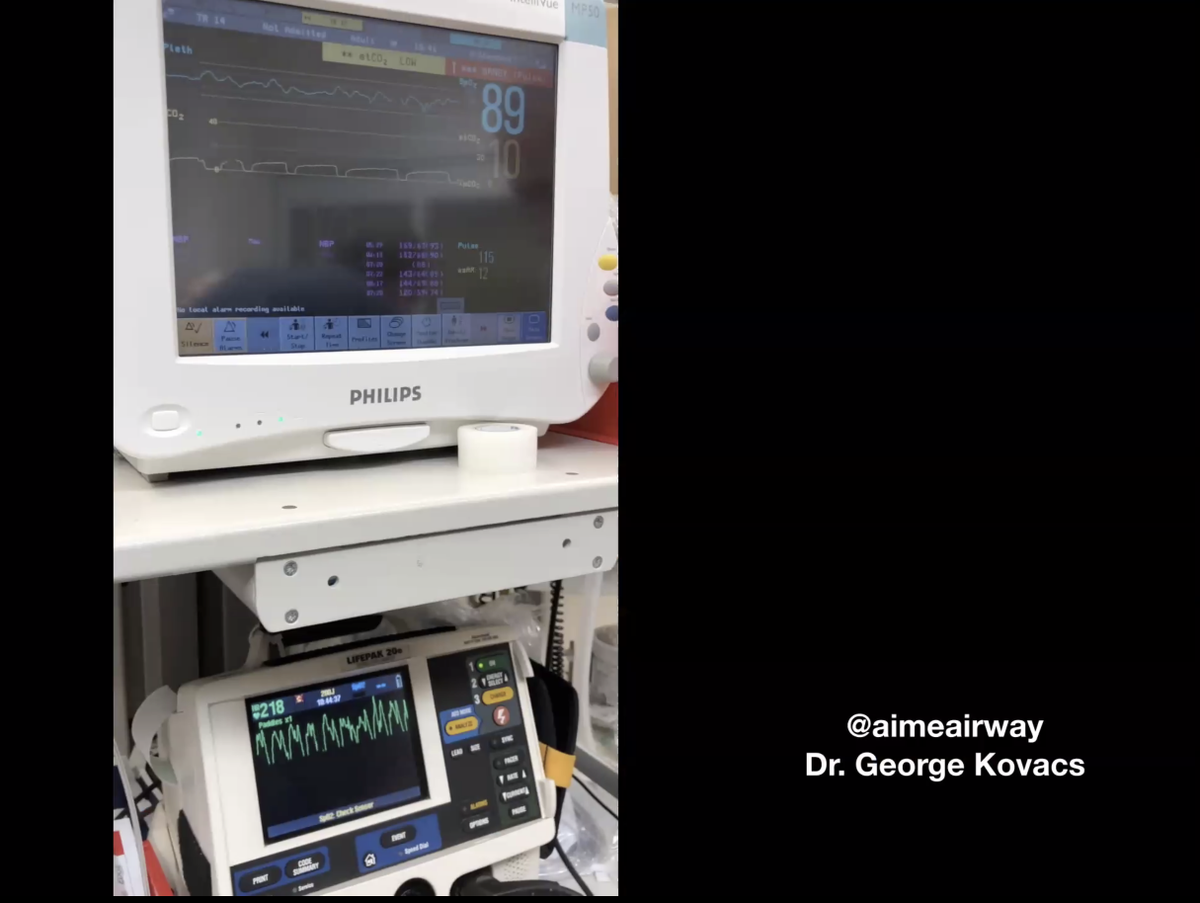
disposable and portable etCO2 monitors are cost-effective. "they are worth their weight in gold"
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded

- need to move from "cant-intubate-cant-oxygenate" to can't-ventilate-can't-oxygenate.
- etCO2 is best real-time indicator of whether we are ventilating. Ventilation falls first, oxygenation will inevitably follow (but may delay).
- @drlauraduggan at #HRreloaded
- etCO2 is best real-time indicator of whether we are ventilating. Ventilation falls first, oxygenation will inevitably follow (but may delay).
- @drlauraduggan at #HRreloaded

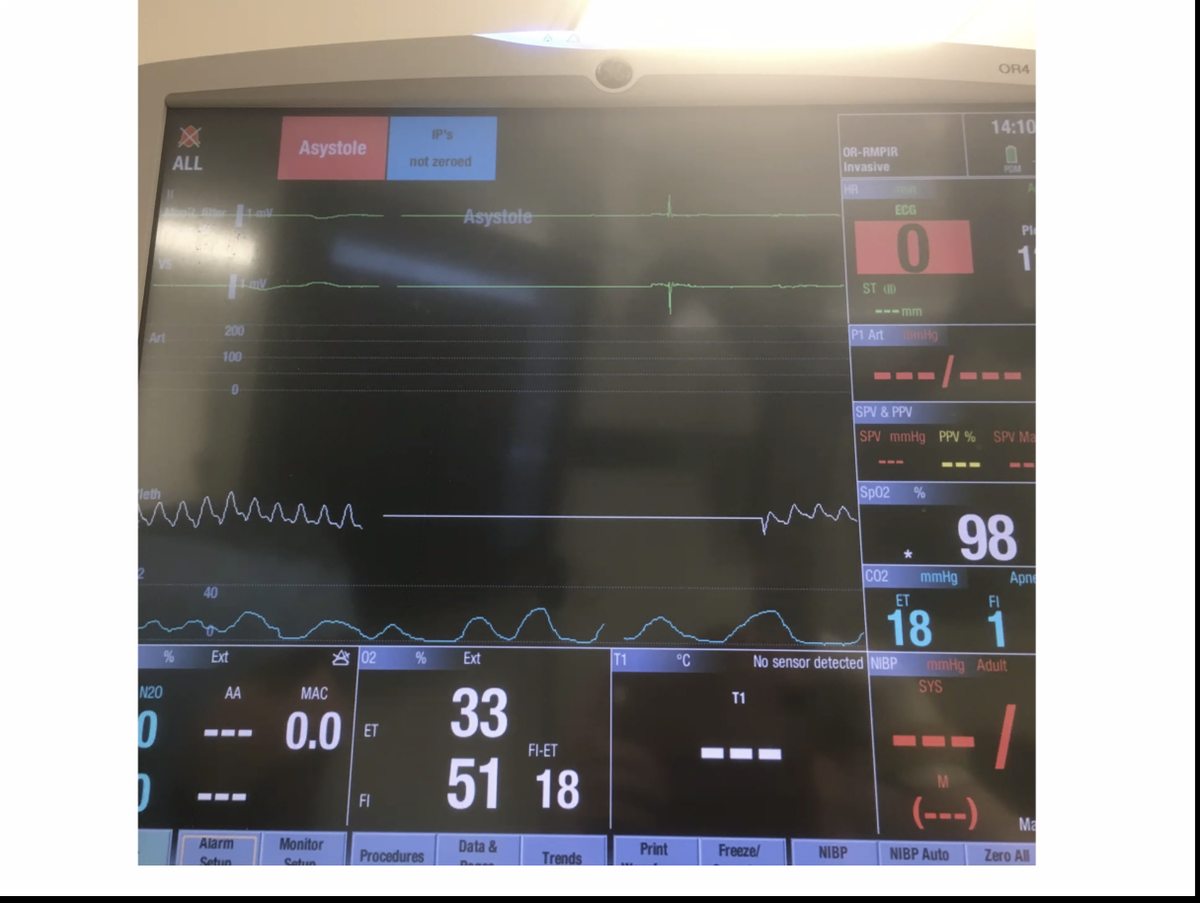
this patient is very difficult to bag. etCO2 waveform is awful, but it takes *minutes* for her saturation to fall.
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded

even in asystole, there should be a CO2 waveform. so absent CO2 waveform means you're in the esophagus! also if etCO2 jumps this can reveal ROSC.
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
"supraglottic airways are the bomb"
fast learning curve
very frequently salvage CVCO situations
- @drlauraduggan at #HRreloaded
fast learning curve
very frequently salvage CVCO situations
- @drlauraduggan at #HRreloaded

we need to ditch the "surgical" airway, because this implies that you need a surgeon. you don't need a surgeon! "this is our lane"
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded

don't mcguyver wierd stuff to try to get people out CVCO. wire-guided, needle-guided techniques fail.
- @drlauraduggan at #HRreloaded
- @drlauraduggan at #HRreloaded
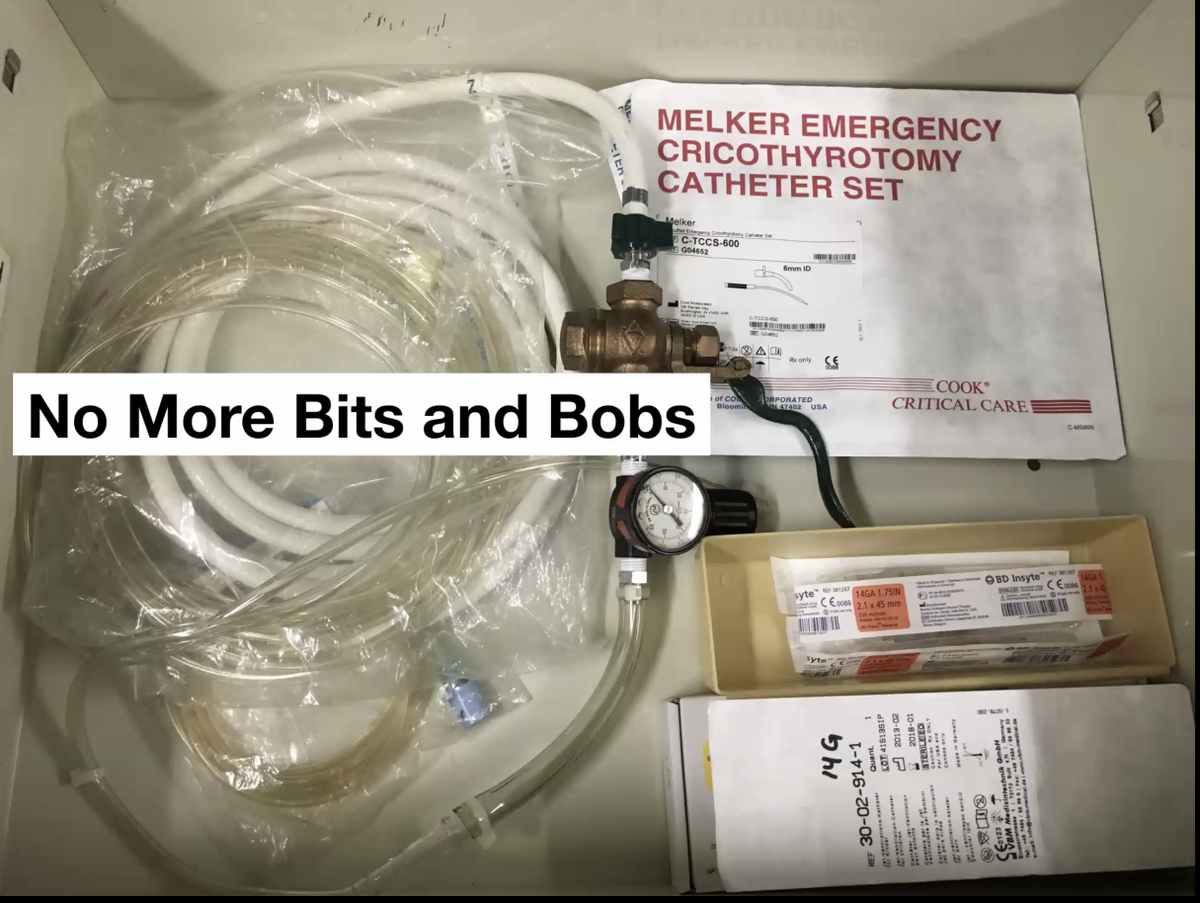
scalpel-finger-bougie will be guideline in canada
always start with vertical incision at least 4-6 cm
- @drlauraduggan at #HRreloaded
always start with vertical incision at least 4-6 cm
- @drlauraduggan at #HRreloaded
take-home messages
- VL to improve communication
- etCO2 waveform & believe it
- long-acting paralytic
- SGA
- Cric
- @drlauraduggan at #HRreloaded
- VL to improve communication
- etCO2 waveform & believe it
- long-acting paralytic
- SGA
- Cric
- @drlauraduggan at #HRreloaded
Loading suggestions...