

1/ Hi #medtwitter! We’re back with a new case @TheSkeletonKG. Call from ER for quadriparesis and dry eyes with dyselectrolytemia. Let's break it down with a #tweetorial #FOAMed #NephTwitter
Link to blog post 👉renalfellow.org
Link to blog post 👉renalfellow.org
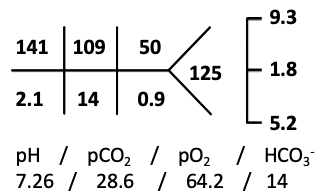
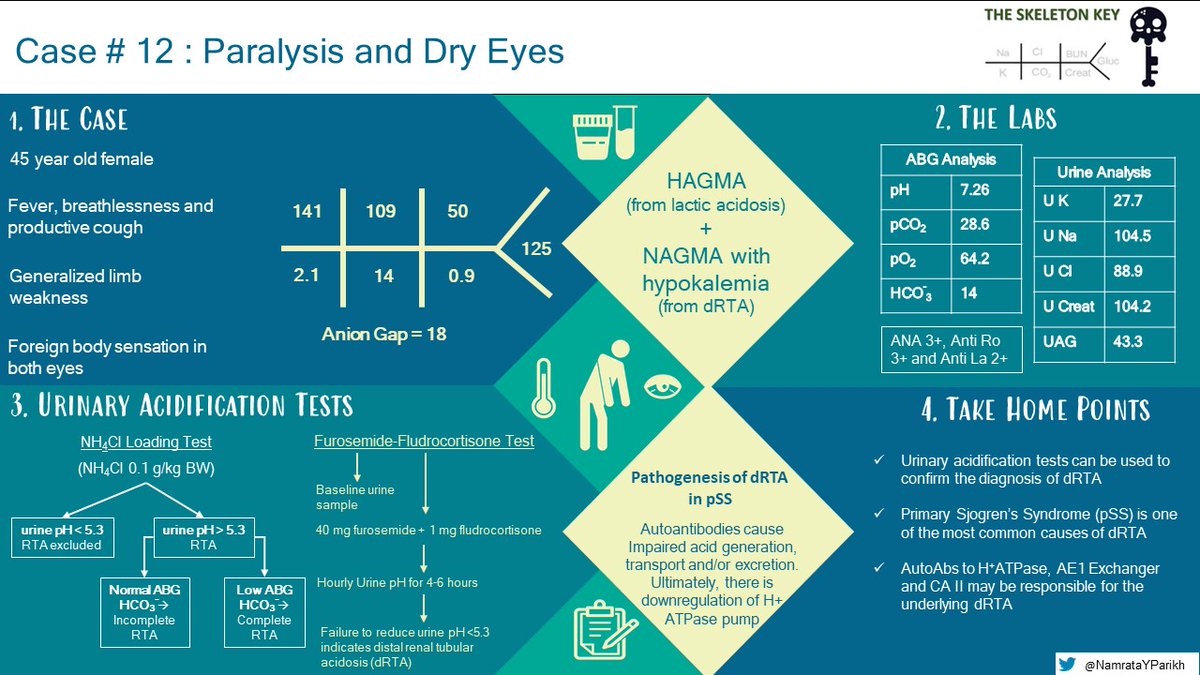
2/ 45 y/o F presents with
⚡️Pneumonia
⚡️Weakness involving all four limbs
⚡️BP of 120/70.
Her labs:
⚡️Pneumonia
⚡️Weakness involving all four limbs
⚡️BP of 120/70.
Her labs:
3/ What is the best next step in her management?
4/ We agree with ‘B’
The first step is to look for indications that require emergency treatment. For hypokalemia this includes changes such as:
⚡️ECG changes
⚡️Muscle weakness
⚡️Serum K+ < 2.5mEq/L
The first step is to look for indications that require emergency treatment. For hypokalemia this includes changes such as:
⚡️ECG changes
⚡️Muscle weakness
⚡️Serum K+ < 2.5mEq/L
5/ Here is the algorithm we follow for the management of hypokalemia. Adapted from Brenner & Rector’s The Kidney 11th Edition

6/ Let's look further into the labs of this patient following the above algorithm
7/ HAGMA can be due to lactic acidosis caused by sepsis (pneumonia)
What could be the cause of NAGMA in this patient?
What could be the cause of NAGMA in this patient?
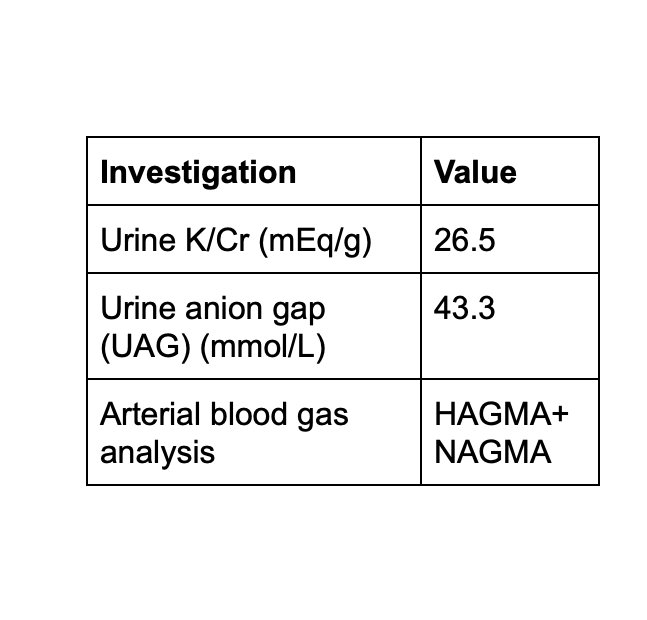
8/ Okay, Let's put it together:
⚡️Low K+
⚡️Urine K/Cr consistent with kidney K+ wasting
⚡️Normal BP
⚡️NAGMA
⚡️Positive UAG
⚡️No features of glycosuria, phosphaturia, uricosuria and aminoaciduria
Looks like our patient has dRTA🤔
⚡️Low K+
⚡️Urine K/Cr consistent with kidney K+ wasting
⚡️Normal BP
⚡️NAGMA
⚡️Positive UAG
⚡️No features of glycosuria, phosphaturia, uricosuria and aminoaciduria
Looks like our patient has dRTA🤔
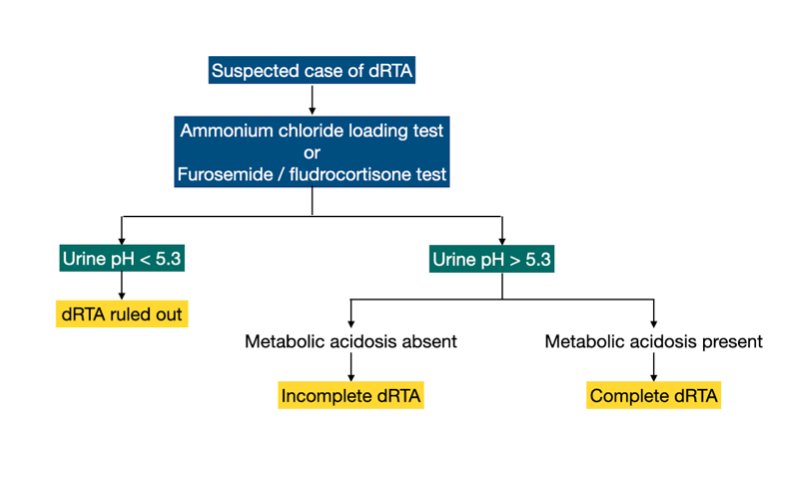
9/ In order to confirm complete dRTA or to test for incomplete dRTA, a ‘test for renal acidification’ is needed.
💥What are the tests for renal acidification?
(*Furosemide/fludrocortisone (F+F) test)
💥What are the tests for renal acidification?
(*Furosemide/fludrocortisone (F+F) test)
10/ Yes, the answer is ‘D’
⚡️The principle of the urine acidification tests is to provide a stimulus for maximal urine acidification
⚡️Inability to reduce urine pH to <5.3 during the test confirms dRTA.
⚡️The principle of the urine acidification tests is to provide a stimulus for maximal urine acidification
⚡️Inability to reduce urine pH to <5.3 during the test confirms dRTA.
11/ In our patient F+F test was done and the diagnosis of distal RTA was confirmed(@Dan_Batlle)
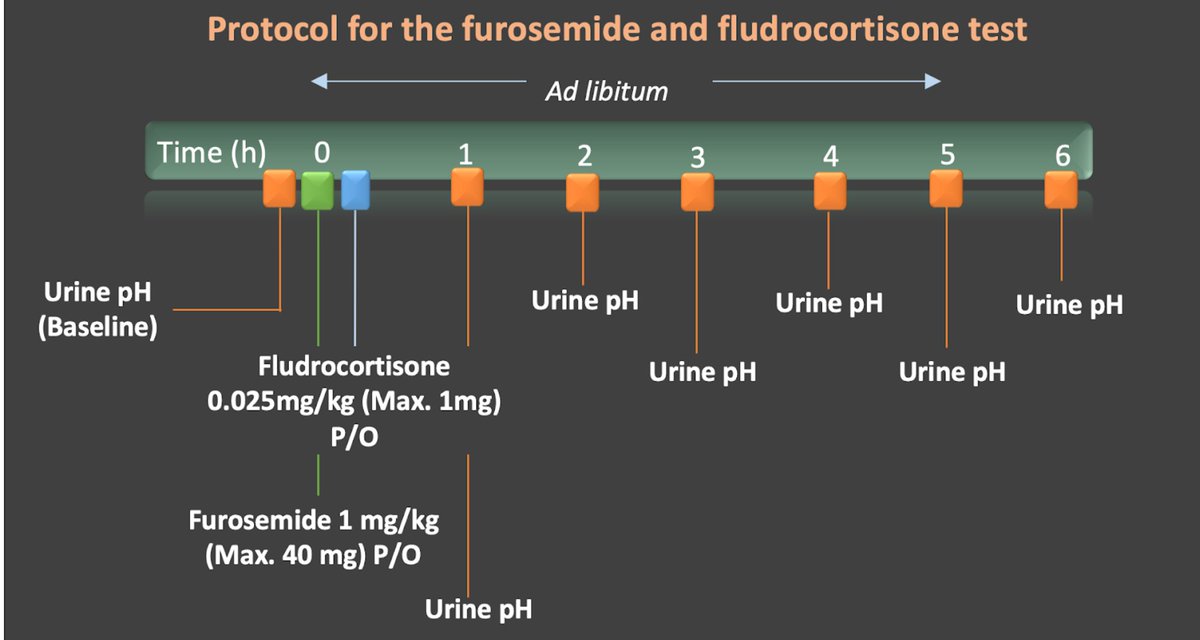
12/ Mechanism of F+F test:
More on this here 👉discovery.ucl.ac.uk
More on this here 👉discovery.ucl.ac.uk

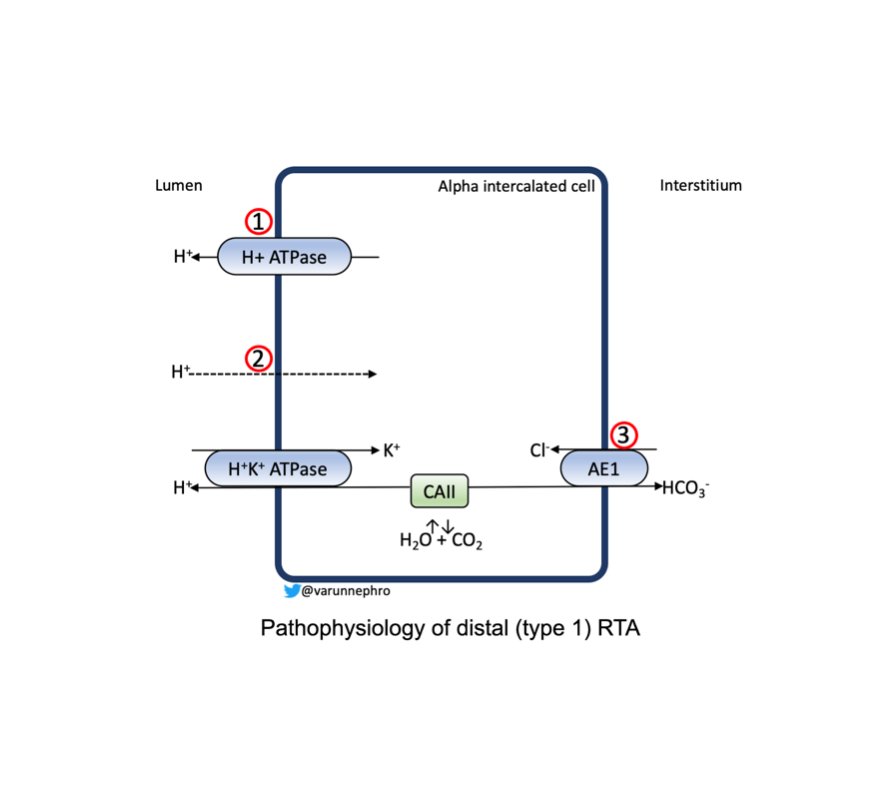
13/ The pathophysiology of dRTA - mainly involves the alpha-intercalated cells by:
1) H+ secretory defect
2) Back leak of H+
3) Defects in basolateral anion exchanger (AE1)
1) H+ secretory defect
2) Back leak of H+
3) Defects in basolateral anion exchanger (AE1)
14/ Wait, but what is the cause of dRTA in our case?
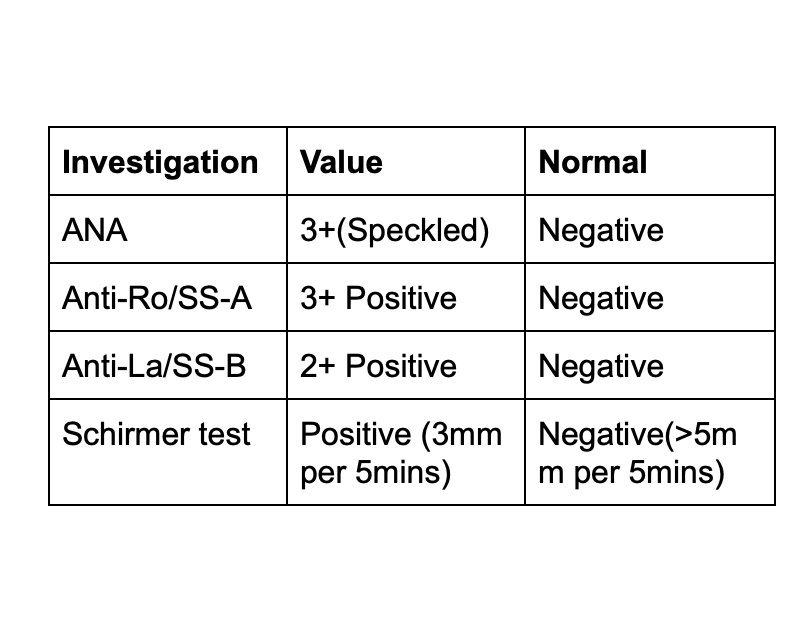
⚡️Patient reports foreign body sensation (dryness) in her eyes
⚡️The results below confirm (2017 ACR-EULAR criteria) the diagnosis of primary Sjögren’s Syndrome (pSS)
More on causes of dRTA here👉ajkd.org
⚡️Patient reports foreign body sensation (dryness) in her eyes
⚡️The results below confirm (2017 ACR-EULAR criteria) the diagnosis of primary Sjögren’s Syndrome (pSS)
More on causes of dRTA here👉ajkd.org
15/ The possible mechanisms of dRTA in pSS are:
💥AutoAb to vacuolar H+-ATPase and AE1 exchanger
💥AutoAb to carbonic anhydrase II (CA II)
More about the kidney manifestations and the pathophysiology of dRTA in pSS from this article 👉nature.com
💥AutoAb to vacuolar H+-ATPase and AE1 exchanger
💥AutoAb to carbonic anhydrase II (CA II)
More about the kidney manifestations and the pathophysiology of dRTA in pSS from this article 👉nature.com
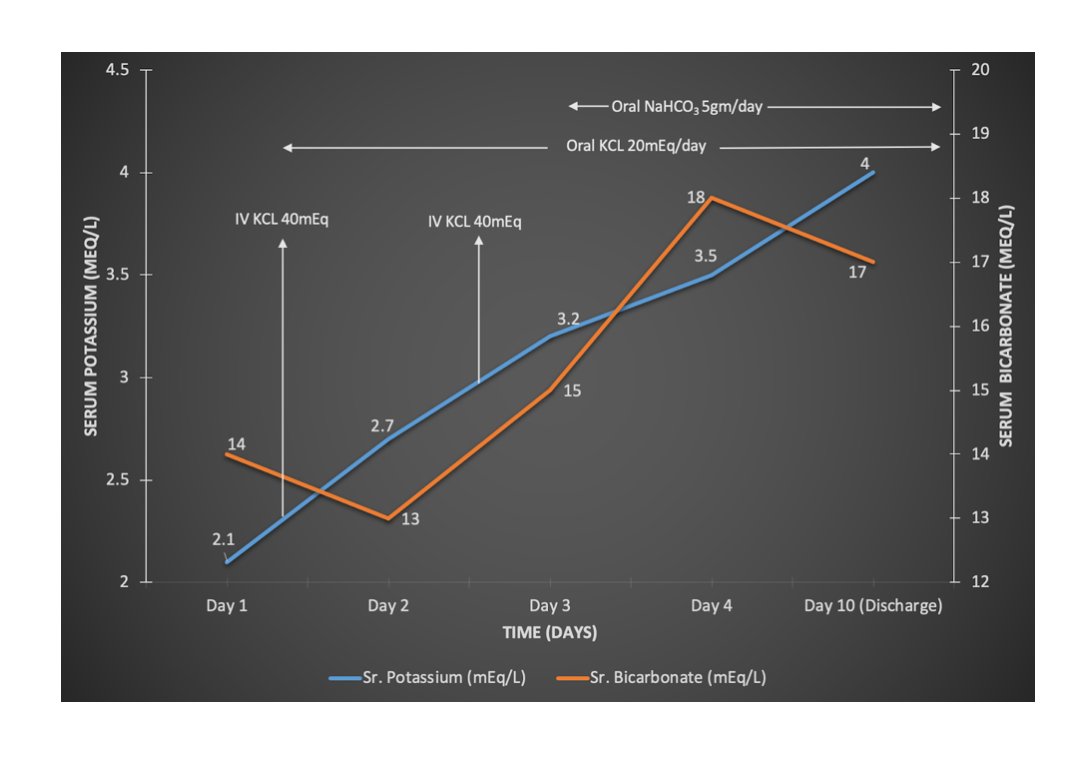
16/ Our patient received the following with an improvement in her potassium, weakness and her other symptoms
⚡️IV KCl correction followed by oral KCl at 20mEq/day
⚡️Oral NaHCO3 at 5gm/day
⚡️IV antibiotics for pneumonia
⚡️Tear replacements for dry eyes
⚡️IV KCl correction followed by oral KCl at 20mEq/day
⚡️Oral NaHCO3 at 5gm/day
⚡️IV antibiotics for pneumonia
⚡️Tear replacements for dry eyes
17/ Serum K+ and HCO3- trend during the hospital stay
18/ Take home points
💥Tests for renal acidification can confirm dRTA
💥Primary Sjogren’s syndrome is one of the common causes of dRTA
💥AutoAb to H+ATPase, AE1 and CA II are the proposed mechanisms for dRTA in pSS
💥Tests for renal acidification can confirm dRTA
💥Primary Sjogren’s syndrome is one of the common causes of dRTA
💥AutoAb to H+ATPase, AE1 and CA II are the proposed mechanisms for dRTA in pSS
19/ ⚡️Check out the amazing VA by @NamrataYParikh and read our 💥post @RenalFellowNtwk (renalfellow.org) to learn more about dRTA, tests for urinary acidification and renal manifestations in pSS
@DTomacruzMD @amyaimei @drM_sudha @cdchu @SaynaNorouzi @kidney_boy
@DTomacruzMD @amyaimei @drM_sudha @cdchu @SaynaNorouzi @kidney_boy
Loading suggestions...