

The Live-Dead qRT-PCR problem, the testing industrial complex and its impact on society.
I never thought the work I did for the human genome project would be weaponized to lock down society. We are now ruled by qPCR right and the transparency on the process is shameful.
I never thought the work I did for the human genome project would be weaponized to lock down society. We are now ruled by qPCR right and the transparency on the process is shameful.
I hope to convey the need to push for public transparency on the CQ values being utilized to count “case” #'s. I also hope to convey the need for home testing and how this regains our medical privacy. It is clearly required for any personalized medicine dream to materialize.
Why listen to me?
I’ve done a lot of PCR (25 yrs). Below is factory floor our R&D team designed, programed, and maintained at The Whitehead Institute/MIT Center for Genome Research. It processed 40M Sanger sequencing reactions/year (a more complicated version of linear PCR)
I’ve done a lot of PCR (25 yrs). Below is factory floor our R&D team designed, programed, and maintained at The Whitehead Institute/MIT Center for Genome Research. It processed 40M Sanger sequencing reactions/year (a more complicated version of linear PCR)

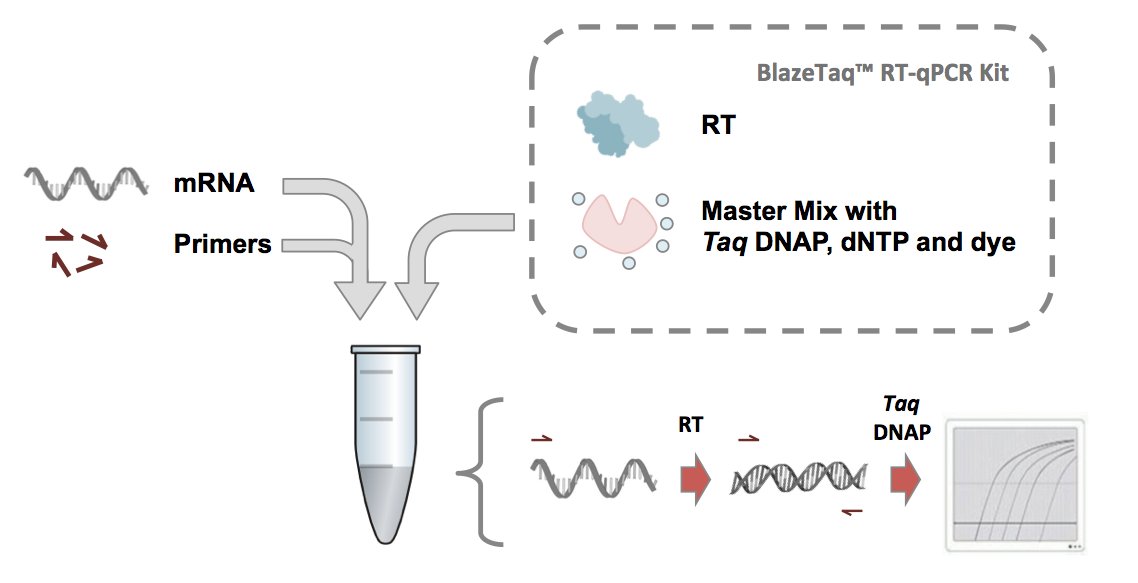
What is the live dead PCR problem? PCR doesn’t count infectious virus. It counts RNA molecules which can be from live or dead virus. Initial infections contain lots of live virus but as you clear the virus the Live-dead ratio shifts more towards the dead.
Jaafar et al addressed this by correlating CQ levels in qPCR with Plaque Forming units (PFUs) on Vero cells. Plaques form only when virus is infectious. Dead Virus forms no plaques.
But culturing virus on Vero cells takes too much time to track pandemics and is hazardous to lab employees as you are replicating live virus.
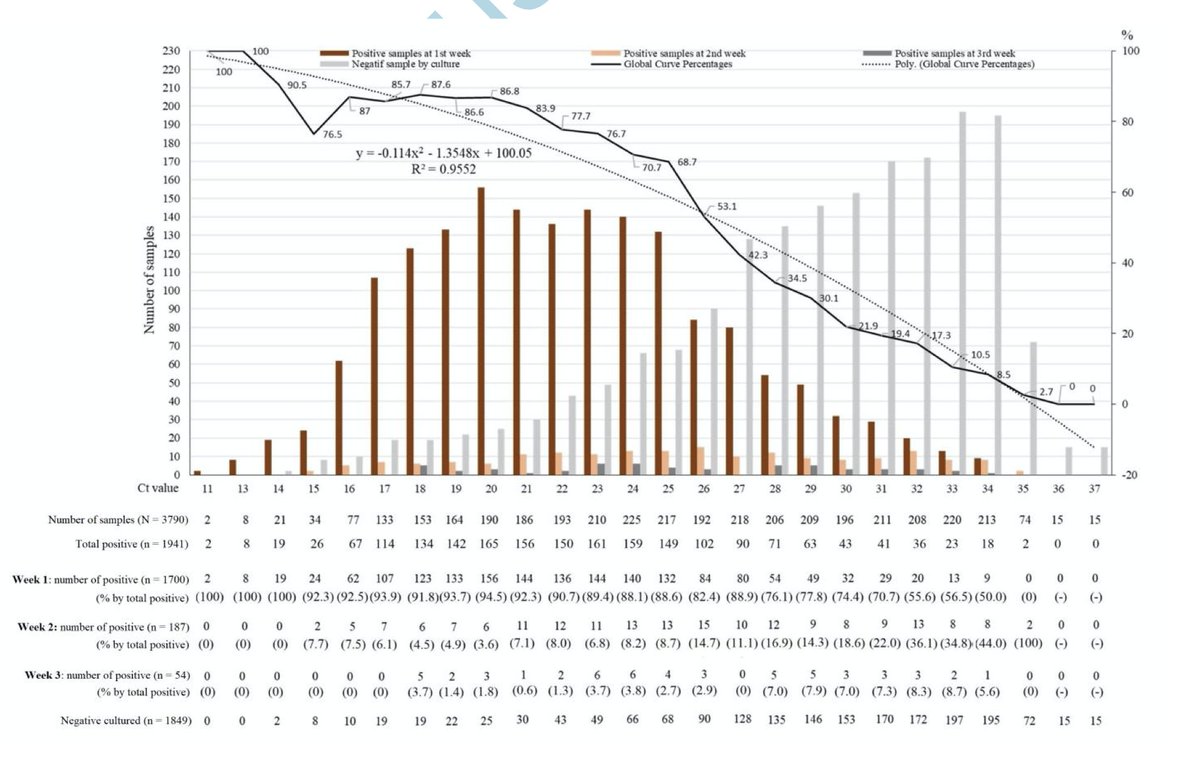
Jaafar et al. showed that Cqs after 33 were mostly dead. Most testing facilities report a positive result if under CQ 40 (but this should be verified in your jurisdiction).
academic.oup.com
academic.oup.com

Due to many diff qPCR tests in the market , one cannot simply lift Jaafar et al equation onto your test but its an important data point.
Cqs are an inverse Log2 scale. Each Cq digit is a factor of 2 so a Cq of 10 is twice as much RNA as a CQ of 11. There are ~3.3 Cqs for every factor of 10. One would use 2^7 or 128 fold to estimate how much difference there is for 7 Cq offset from 33 to 40.
LODs
Limit of Detection.
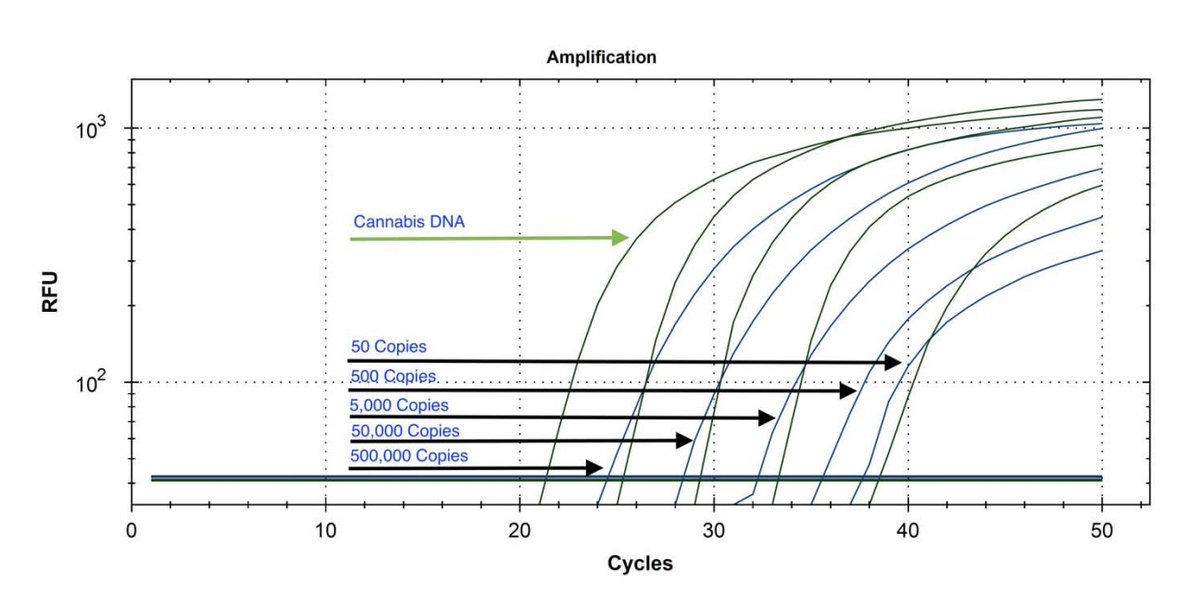
Take RNA, perform a serial dilution in qPCR and measure how low you can go.
Most tests crap out 50 copies of SARs RNA at around 37 cycles. Calling positives past your Limit of detection is shady. I think there is a lot of this going on.
Limit of Detection.
Take RNA, perform a serial dilution in qPCR and measure how low you can go.
Most tests crap out 50 copies of SARs RNA at around 37 cycles. Calling positives past your Limit of detection is shady. I think there is a lot of this going on.
This can create False positives that can transform a pandemic into a “case-ademic”. There are a few papers circulating that demonstrate this effect on other outbreaks that have occurred in the past. Please post them to this thread if you have them at your fingertips.
Sampling limitations.
LODs are measured putting RNA straight into the qPCR. Reality requires qPCR of a nasal swab usually soaked into 1ml of fluid and no-one PCRs the whole milliliter. They take 1/25th - 1/50th of this into the qPCR.
LODs are measured putting RNA straight into the qPCR. Reality requires qPCR of a nasal swab usually soaked into 1ml of fluid and no-one PCRs the whole milliliter. They take 1/25th - 1/50th of this into the qPCR.
If you have 1 copy on that swab and you only take 1/50th of the volume into qPCR.. you have a poisson sampling problem are unlikely to find the single molecule unless 50 tests are performed. This can create false negatives. SNPs under primers can create false negatives as well.
SNPs under primers are something we need to watch as the virus mutates. I think this is a smaller problem right now but needs to be considered when looking at re-infection data.
To understand these have a look at an EUA for the Roche qPCR assay. FDA RUO for Roche as an example
To understand these have a look at an EUA for the Roche qPCR assay. FDA RUO for Roche as an example
FDA EUA links and a few studies comparing different kits performance in the market place.
fda.gov
jcm.asm.org
ncbi.nlm.nih.gov
fda.gov
jcm.asm.org
ncbi.nlm.nih.gov
These FP rates may be low but when the disease prevalence is low, the FPs become a higher % of the total number of positive tests. 1% population disease prevalence with a 1% FP rate would deliver 10 FPs and 10TP out of 1000 tests but you wouldn’t know which of the 20 are T or F.
For some tests the FP rate must be below 1:1000 as we see positivity rates like this at some universities.
See Northeastern university rates (150/~300,000)
news.northeastern.edu
See Northeastern university rates (150/~300,000)
news.northeastern.edu
If you assume those NE tests are FPs, this is an upper bounds on the FP rate. Reality is they are probably a mixture but public transparency on the FPs and FN of the test being run is sorely lacking. This is clinically irresponsible.
Why Live-Dead matters.
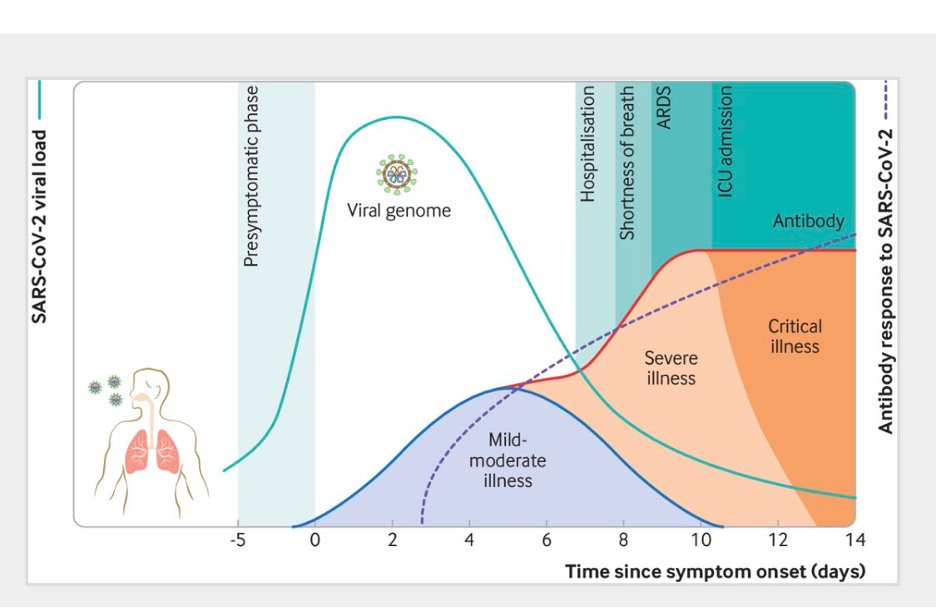
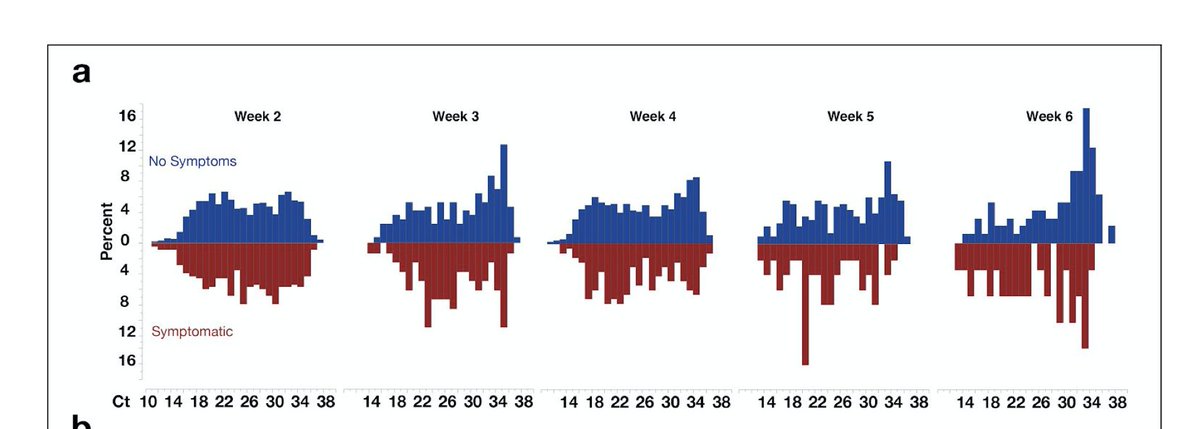
The majority of the time a patient is qPCR positive (<40Cq) is the tail end of the disease where the virus is shedding and more dead than alive RNA. I call this the lower infectivity long tail. People detected in this window are usually non-infectious
The majority of the time a patient is qPCR positive (<40Cq) is the tail end of the disease where the virus is shedding and more dead than alive RNA. I call this the lower infectivity long tail. People detected in this window are usually non-infectious
These poor folks are quarantined, track & traced, medical privacy violated, constitution nullified and shamed from society. But this creates a lot more testing volume! I doubt there is motivation to tighten the dial, despite there being cheap old-school tools which address this.

How does one address this?
Does every test need a Jaafar correlation curve? Maybe. There is another Maniatis/Sambrook trick one could use. This is getting old school, open source and cheap.
Does every test need a Jaafar correlation curve? Maybe. There is another Maniatis/Sambrook trick one could use. This is getting old school, open source and cheap.
Viruses evolved from viroids. They differ in that viruses evolved protein coats to protect the RNA from nucleases. Life has evolved many tools to target and destroy naked viroids and one of them are RNases. These digest RNA into smaller nonfunctional pieces.
RNases are cheap and as ubiquitous as chalk in a classroom in the genomics field. They are easily used and deactivated with RNase blockers.
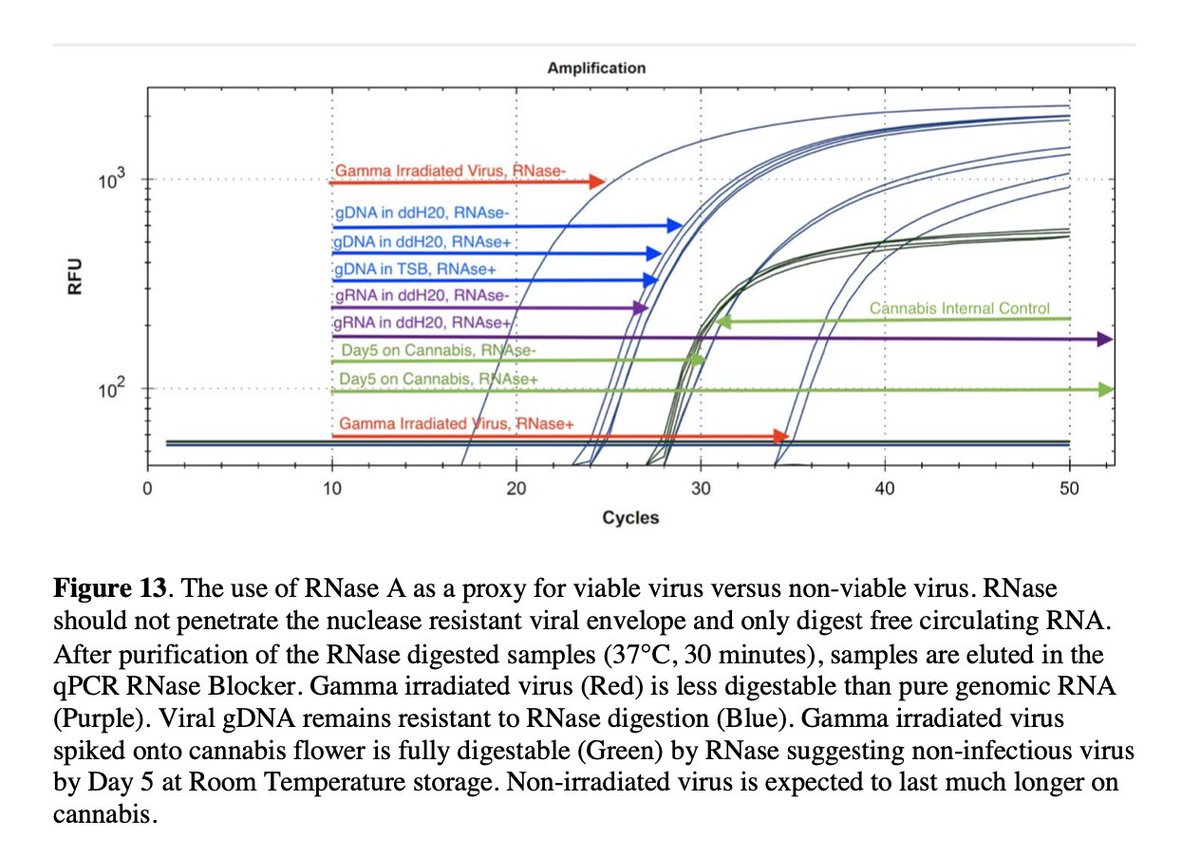
A person skilled in the art would be tempted to RNase treat the nasal sample prior to phage lysis to resolve the non-infectious RNA from the infectious RNA. qPCR could be performed before and after this treatment to measure total RNA and RNA that is nuclease resistant.
Figure 13 in our manuscript makes an attempt at this. It needs more validation with a Jaafar like calibration but derisks much of this approach.
biorxiv.org
biorxiv.org

With the proper internal controls this assay would provide a ratio of Live-Dead viral RNA and provide more clarity on who to retest 24 hours later. Testing 2 days apart can inform you if the total load is going up or going down and rule out FPs and FNs on the first test.
2X the testing but significantly reduce # of people trapped in the long tail and vacuuming in all of their contacts map into a testing frenzy. Net:Net, this would probably mean less testing and I suspect that is why this simple and obvious Live-Dead trick is being ignored.
Here is a paper from Quest Diagnostics looking at testing multiple time points.
medrxiv.org
medrxiv.org
Now that I have your attention regarding Costs... This video from @ThomasEWoods is a must watch.
youtube.com
youtube.com
Some estimates on the cost of track and trace to prevent a single death are staggering.
medrxiv.org
medrxiv.org

This brings up an important economic point. When we print excessive money we end up with Cantillon effects.
aier.org
aier.org

You see inflation in the price of goods through the artery in which the money is being injected. Don’t believe me.. qPCR test are usually under $10. CLIA regs might inflate that cost to $50. Money Printer go BRRRR ...The rapid COVID tests in Mass are $140.
I hope this thread encourages you to ask the testing labs for their FP/FN rates. Push for public transparency of the CQ values to be reported with the Case data. Without this, the FP rates will ensure the pandemic never ends. At home private testing would change this as well.
A final paper from the Broad Institute on CQ values over time and how they creep out towards the LOD.
medrxiv.org
medrxiv.org
Loading suggestions...