

#MedTwitter - we're back with another tweetorial 🥳
Thanks @john_damianosMD for this week's edition on 🩸GI bleeds🩸
Thanks @john_damianosMD for this week's edition on 🩸GI bleeds🩸

ICYMI, listen to our "Episode 4: Lower GI Bleed" pod which featured Dr. Navin Kumar @NavinKumarMD (gastroenterologist), and Dr. Walker Redd @WalkerReddMD (host).
To listen 🔊🍏: apple.co
Let's start with a guiding question below!🧐
To listen 🔊🍏: apple.co
Let's start with a guiding question below!🧐


76 yo F w/ HTN, Afib (on apixaban), & moderate aortic stenosis was admitted with progressive weakness, fatigue, & melena, with Hgb = 6 g/dL.
After💧resuscitation and🩸transfusion, she underwent colonoscopy which did❌locate source.
What is the next diagnostic step?
After💧resuscitation and🩸transfusion, she underwent colonoscopy which did❌locate source.
What is the next diagnostic step?
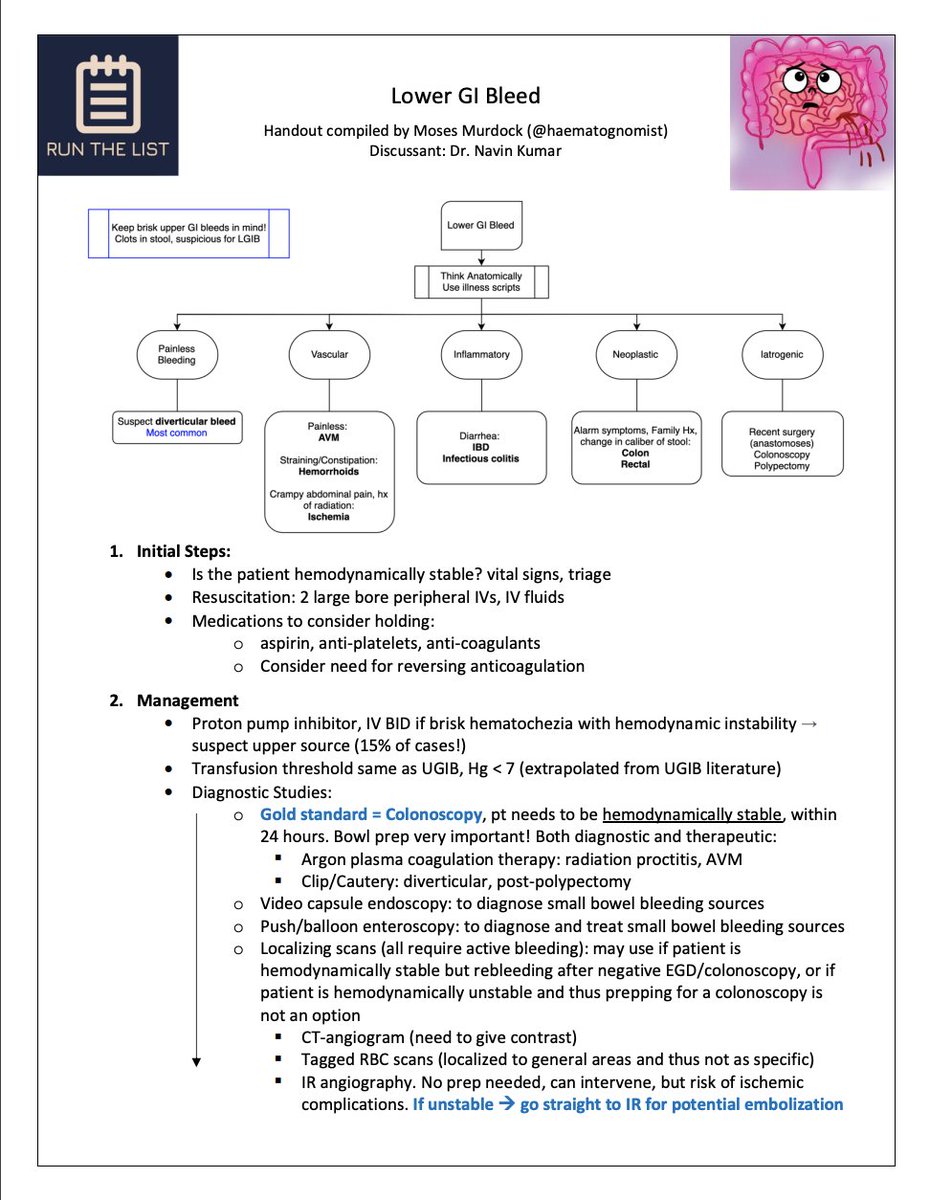
Let's zoom out & consider a general initial approach:
1⃣Is this patient hemodynamically stable?
🩸BP 💓HR 🧠Mental status
2⃣Where is the bleed coming from?
🧬anatomy, etiology, history
3⃣Is the pt on 💊which ⬆️ bleeding risk?
💊warfarin, DOACs, NSAIDs, anti-platelets, etc.
1⃣Is this patient hemodynamically stable?
🩸BP 💓HR 🧠Mental status
2⃣Where is the bleed coming from?
🧬anatomy, etiology, history
3⃣Is the pt on 💊which ⬆️ bleeding risk?
💊warfarin, DOACs, NSAIDs, anti-platelets, etc.

1⃣Prioritize resuscitation to ensure hemodynamic stability
💉💉TWO large bore IVs (≥18 gauge)▶️FLUIDS 💧💧💧
🧫type and screen
🩸TRANSFUSE (goal >7⃣ g/dL)
💉💉TWO large bore IVs (≥18 gauge)▶️FLUIDS 💧💧💧
🧫type and screen
🩸TRANSFUSE (goal >7⃣ g/dL)

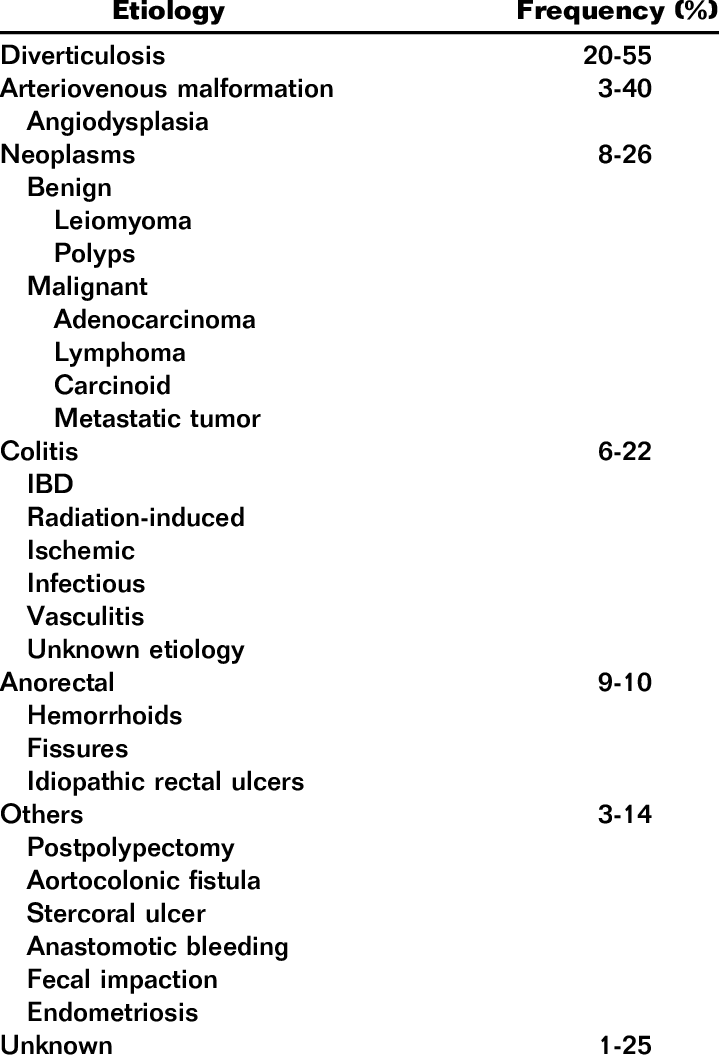
2⃣Think about BLEEDING SOURCE
Anatomy:
⚕️anus, rectosigmoid, colon, small bowel, upper GI
Etiology:
🩸Vascular- diverticulosis, AVMs, hemorrhoids, ischemia, radiation
🔥Inflammatory- IBD, infectious
🦀Neoplastic- colorectal cancer
👩⚕️Iatrogenic- anastomotic, post-polypectomy
Anatomy:
⚕️anus, rectosigmoid, colon, small bowel, upper GI
Etiology:
🩸Vascular- diverticulosis, AVMs, hemorrhoids, ischemia, radiation
🔥Inflammatory- IBD, infectious
🦀Neoplastic- colorectal cancer
👩⚕️Iatrogenic- anastomotic, post-polypectomy
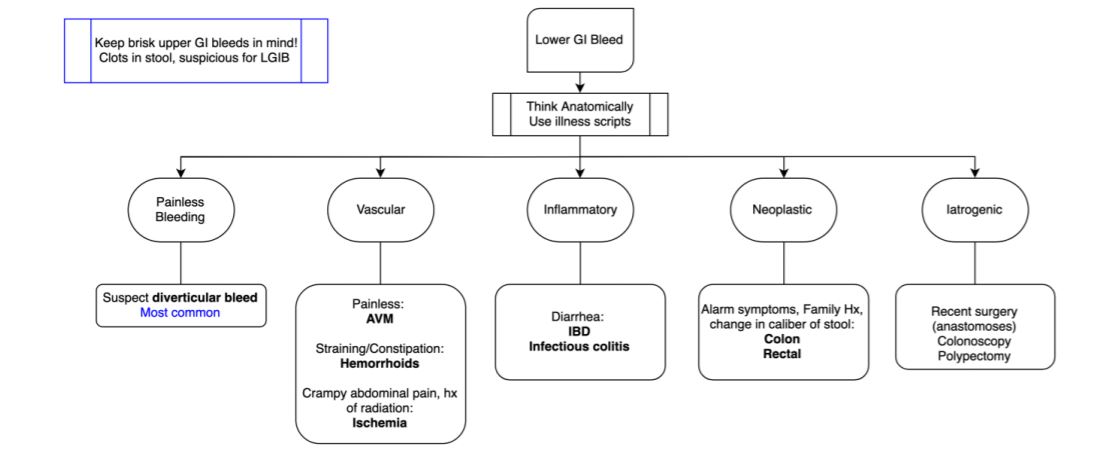
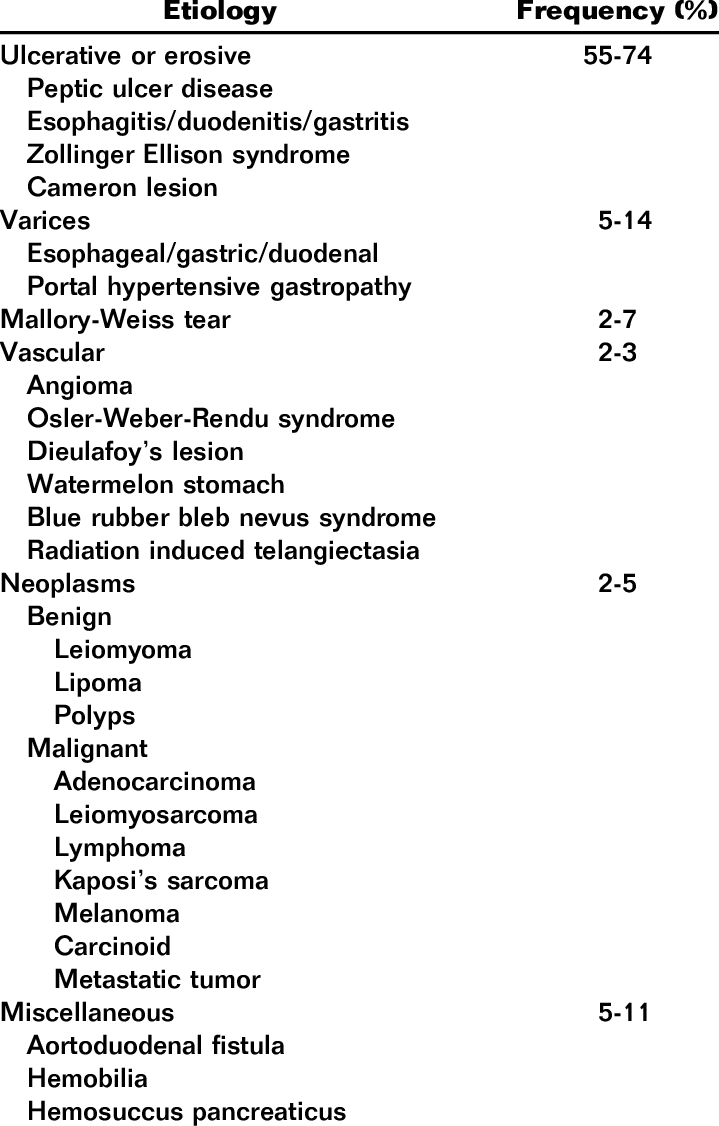
⚠️Don't be fooled⚠️
15% of lower GI bleeds are actually brisk UPPER GI bleeds!
Keep (upper GI) on the ddx, especially in:
❗️hemodynamically unstable pts
❗️clots in 💩
❗️UGIB risk factors (e.g. esophageal varices)
Management:
🔭consider EGD before colonoscopy
💊IV PPI
DDx⬇️
15% of lower GI bleeds are actually brisk UPPER GI bleeds!
Keep (upper GI) on the ddx, especially in:
❗️hemodynamically unstable pts
❗️clots in 💩
❗️UGIB risk factors (e.g. esophageal varices)
Management:
🔭consider EGD before colonoscopy
💊IV PPI
DDx⬇️
🔍Look for bleeds!
🥴Once hemodynamically stable
🔘COLONOSCOPY w/i 24h of presentation
🔘bowel prep = 🔑
Intervenable bleeds:
Diverticular: 📎 = can clip
AVM: 🕯️= argon plasma coagulation
Post-polypectomy bleed: 📎 vs. cautery
Radiation proctitis: 🕯️
Anastomotic bleed: 📎
🥴Once hemodynamically stable
🔘COLONOSCOPY w/i 24h of presentation
🔘bowel prep = 🔑
Intervenable bleeds:
Diverticular: 📎 = can clip
AVM: 🕯️= argon plasma coagulation
Post-polypectomy bleed: 📎 vs. cautery
Radiation proctitis: 🕯️
Anastomotic bleed: 📎
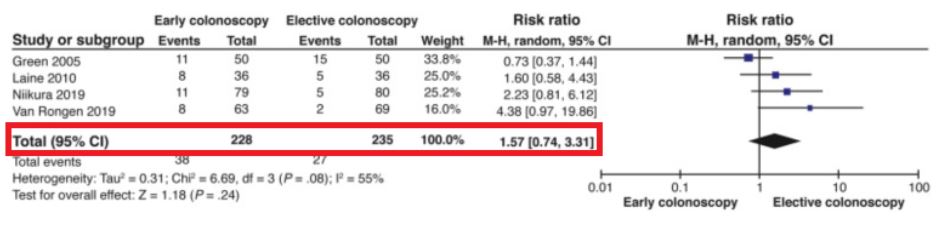
Should we rush to get them in before 24 hours? 🙅♂️
RCTs (pubmed.ncbi.nlm.nih.gov) found that earlier colonoscopy does❌ ⬇️re-bleeding or ⬇️mortality risk.
So instead, focus efforts toward adequate resuscitation & starting bowel prep!
Meta-analysis: pubmed.ncbi.nlm.nih.gov
RCTs (pubmed.ncbi.nlm.nih.gov) found that earlier colonoscopy does❌ ⬇️re-bleeding or ⬇️mortality risk.
So instead, focus efforts toward adequate resuscitation & starting bowel prep!
Meta-analysis: pubmed.ncbi.nlm.nih.gov
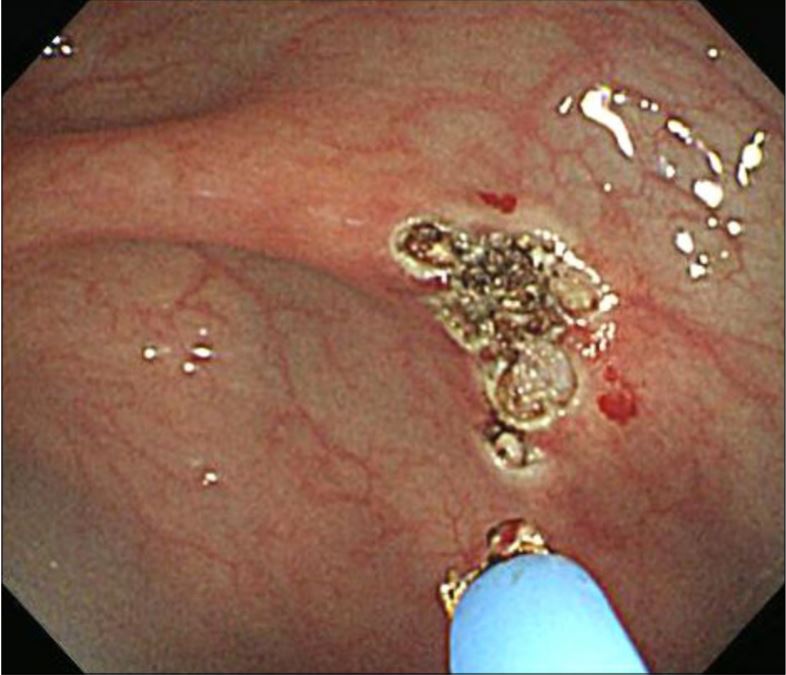
If colonoscopy ❌identify source, try other diagnostic modalities:
🔘EGD (w push enteroscopy for small bowel visualization)
🔘video capsule endoscopy (pic1⬇️ = small bowel AVM)
🔘🎈enteroscopy
🔘Localizing scans:
✅tagged RBC scan (pic2⬇️ = LGIB)
✅CT angio
✅IR angio
🔘EGD (w push enteroscopy for small bowel visualization)
🔘video capsule endoscopy (pic1⬇️ = small bowel AVM)
🔘🎈enteroscopy
🔘Localizing scans:
✅tagged RBC scan (pic2⬇️ = LGIB)
✅CT angio
✅IR angio


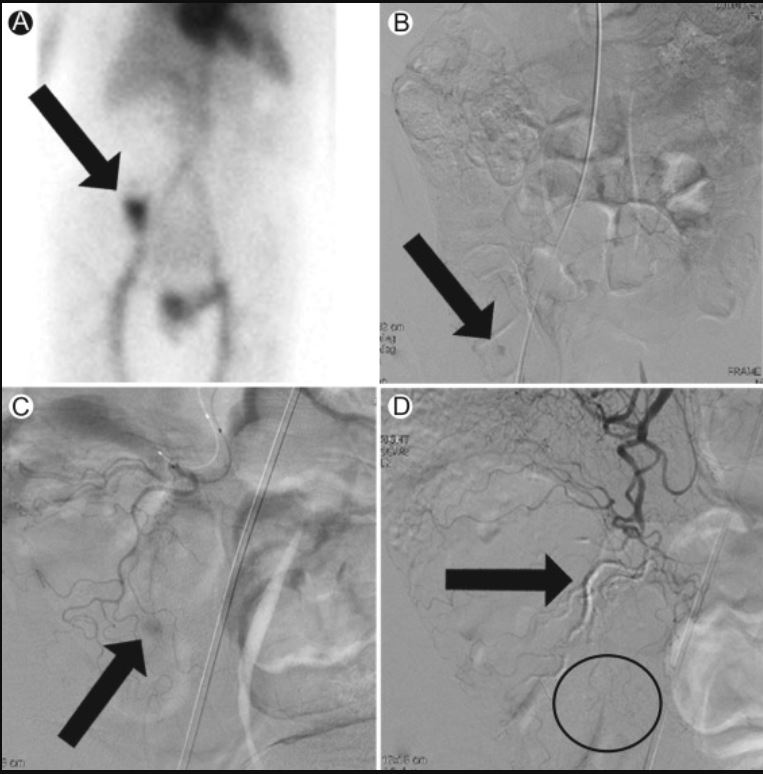
Localizing Scans for a LGIB (Nice job IR😍)
🌟Tagged RBC:⬆️radiotracer uptake in cecum = active🩸in area
🌟Angio of SMA: active🩸in R colon
🌟Angio of ileocolic artery: locates extravasation area
🌟Post-embolization: cast fills culprit ileocolic branch▶️🩸resolved(!)
🌟Tagged RBC:⬆️radiotracer uptake in cecum = active🩸in area
🌟Angio of SMA: active🩸in R colon
🌟Angio of ileocolic artery: locates extravasation area
🌟Post-embolization: cast fills culprit ileocolic branch▶️🩸resolved(!)
Take-aways:
📝Assess HD stability🥴/🤢
🔹influences diagnostic decision: colonoscopy vs IR
🔹prioritize access and resuscitation💧🩸
📝If brisk UPPER GI bleed with severe hematochezia
🔹start PPI💊 & consider EGD first
📝If HDS▶️ bowel prep ASAP
📝Assess HD stability🥴/🤢
🔹influences diagnostic decision: colonoscopy vs IR
🔹prioritize access and resuscitation💧🩸
📝If brisk UPPER GI bleed with severe hematochezia
🔹start PPI💊 & consider EGD first
📝If HDS▶️ bowel prep ASAP
Okay, back to our 👵with a LGIB and negative colonoscopy. What's the next diagnostic step?
✅EGD with push enteroscopy!
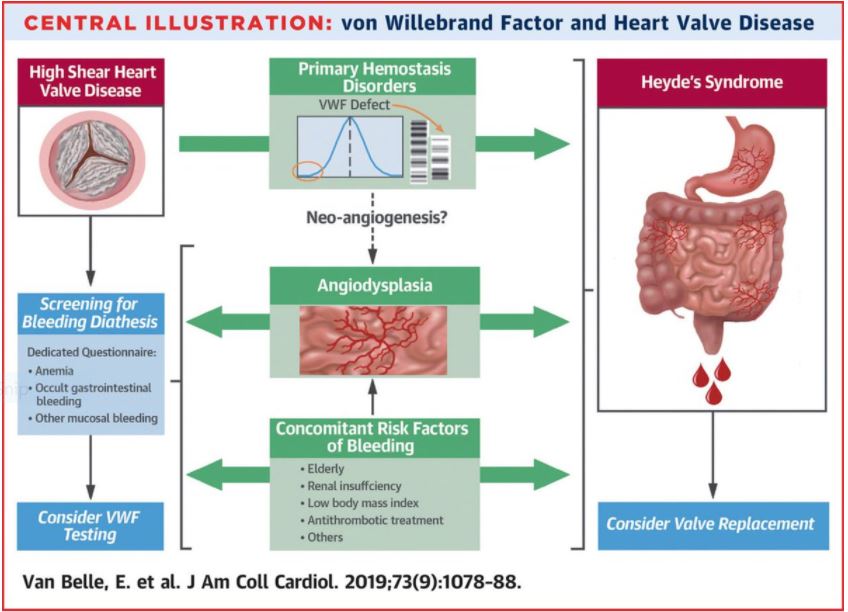
This is likely a small bowel bleed. In our patient with aortic stenosis, this may be HEYDE SYNDROME, which describes the association between AS and small bowel AVMs (via acquired von Willebrand factor deficiency)! 🤯
This is likely a small bowel bleed. In our patient with aortic stenosis, this may be HEYDE SYNDROME, which describes the association between AS and small bowel AVMs (via acquired von Willebrand factor deficiency)! 🤯
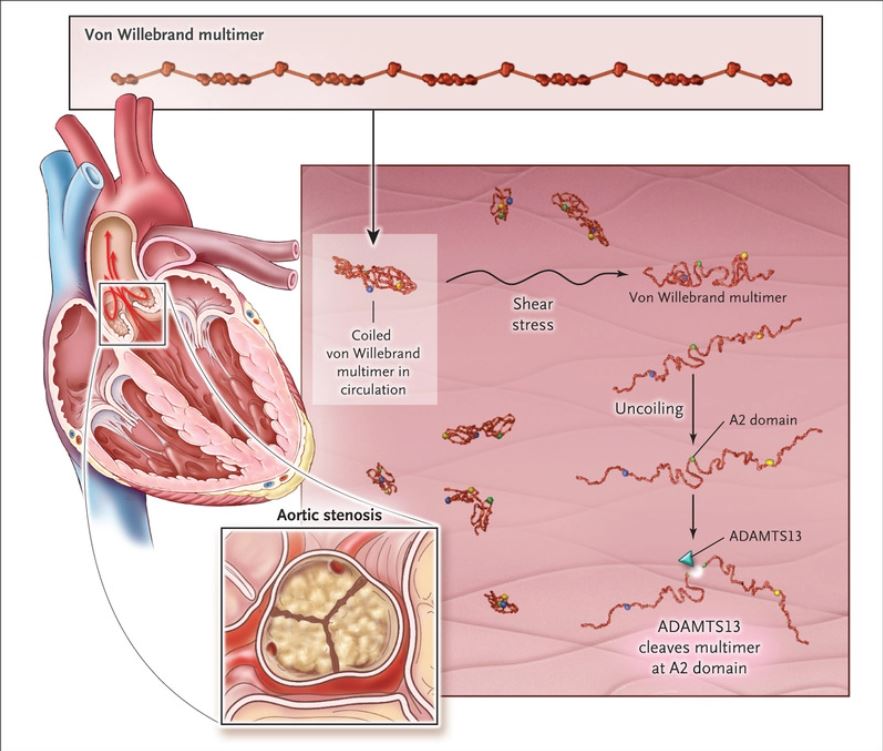
HEYDE SYNDROME SUMMARY:
📐Triad= aortic stenosis, GI🩸, acquired vWF deficiency
📐age▶️tissue degeneration▶️AS
🫀shear stress▶️vWF unfolding▶️⬆️ADAMTS13✂️
🫀⬇️perfusion/cholesterol emboli▶️GI tissue hypoxia🤢
✅End result: small bowel AVMs▶️🩸
✅consider valve replacement
📐Triad= aortic stenosis, GI🩸, acquired vWF deficiency
📐age▶️tissue degeneration▶️AS
🫀shear stress▶️vWF unfolding▶️⬆️ADAMTS13✂️
🫀⬇️perfusion/cholesterol emboli▶️GI tissue hypoxia🤢
✅End result: small bowel AVMs▶️🩸
✅consider valve replacement
References:
[7]linkinghub.elsevier.com
[8]kjg.or.kr
[9]pubmed.ncbi.nlm.nih.gov, pubmed.ncbi.nlm.nih.gov
[10]gut.bmj.com, link.springer.com
[11]techvir.com
[14]nejm.org
[15]dl.uswr.ac.ir
[7]linkinghub.elsevier.com
[8]kjg.or.kr
[9]pubmed.ncbi.nlm.nih.gov, pubmed.ncbi.nlm.nih.gov
[10]gut.bmj.com, link.springer.com
[11]techvir.com
[14]nejm.org
[15]dl.uswr.ac.ir
Loading suggestions...