

1/ 📢Hello #MedTwitter
Let’s talk about pediatric #MPGN / ‘Immune complex GN’ #ICGN today
A few pearls from the 1st @ASPNeph pathology webinar of 2021
#tweetorial #NephTwitter
Let's begin with a poll:
❓Which of the following is true about IC-MPGN?
Let’s talk about pediatric #MPGN / ‘Immune complex GN’ #ICGN today
A few pearls from the 1st @ASPNeph pathology webinar of 2021
#tweetorial #NephTwitter
Let's begin with a poll:
❓Which of the following is true about IC-MPGN?
2/ All the above
⚡️There is limited data on epidemiology
⚡️The estimated prevalence is 1 to 2/ million children, 5 to 15 years of age
⚡️There is limited data on epidemiology
⚡️The estimated prevalence is 1 to 2/ million children, 5 to 15 years of age
3/💥MPGN denotes “pattern of injury” not etiology
⚡️Characteristic mesangial & endocapillary cellularity
⚡️Thickening of glomerular capillary walls due to subendothelial deposition of IC/complement factors
⚡️Characteristic mesangial & endocapillary cellularity
⚡️Thickening of glomerular capillary walls due to subendothelial deposition of IC/complement factors

4/ 💥Type III hypersensitivity reaction💥 is the hallmark of the disease
⚡️”Anything” can form IC→IC deposition→activation of immune cells→ ‘complement activation’→ Glomerular injury
⚡️complement dysregulation is the key🗝️factor
⚡️”Anything” can form IC→IC deposition→activation of immune cells→ ‘complement activation’→ Glomerular injury
⚡️complement dysregulation is the key🗝️factor

5/ 💥Currently, “triggers/ risk factors” for host injury are unknown
⚡️Damage is inversely proportional to Antigen (Ag) clearing
⚡️In other words, chronic antigenemia = chronic inflammation
⚡️Damage is inversely proportional to Antigen (Ag) clearing
⚡️In other words, chronic antigenemia = chronic inflammation
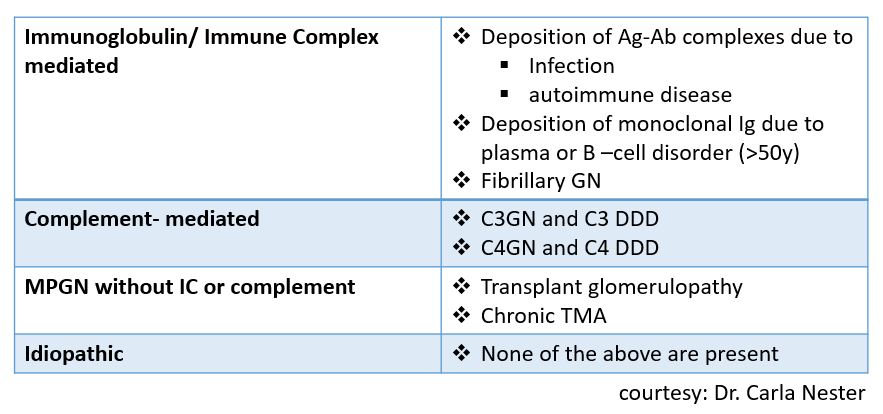
6/ 💥Latest classification is based on IF-
⚡️C3 dominant deposits→ C3 Glomerulopathy (C3GN & DDD)- rare
⚡️C3 + Ig deposits→ Ig- MPGN (Immunoglobulin asso. MPGN)
⚡️No deposits MPGN→ Chr. TMA, transplant glomerulopathy, etc.
⚡️C3 dominant deposits→ C3 Glomerulopathy (C3GN & DDD)- rare
⚡️C3 + Ig deposits→ Ig- MPGN (Immunoglobulin asso. MPGN)
⚡️No deposits MPGN→ Chr. TMA, transplant glomerulopathy, etc.

7/ 💥Etiopathogenesis:
⚡️IC- MPGN is via CLASSICAL complement pathway activation,
⚡️C3G is due to primary alternative complement pathway dysregulation
⚡️IC- MPGN is via CLASSICAL complement pathway activation,
⚡️C3G is due to primary alternative complement pathway dysregulation

8/💥 MPGN is associated with a variety of disorders. Common one being
⚡️Complement system abnormalities
⚡️SLE
⚡️Hepatitis B &C
⚡️>50y -monoclonal gammopathies
⚡️Complement system abnormalities
⚡️SLE
⚡️Hepatitis B &C
⚡️>50y -monoclonal gammopathies

9/ 💥What is the most common presentation of IC-MPGN?
10/ Ans: Hematuria
💥Clinical presentation is heterogeneous
⚡️ranges from asymptomatic hematuria to AKI
⚡️In a pediatric study: hematuria> HTN > NS #secsectitle0030" target="_blank" rel="noopener" onclick="event.stopPropagation()">kireports.org
💥Clinical presentation is heterogeneous
⚡️ranges from asymptomatic hematuria to AKI
⚡️In a pediatric study: hematuria> HTN > NS #secsectitle0030" target="_blank" rel="noopener" onclick="event.stopPropagation()">kireports.org

11/💥 A 14 yr old adolescent male patient presented with HTN, hematuria, nephrotic syndrome, and AKI. Kidney biopsy revealed IC-MPGN. What will be your initial workup?
12/ 💥Ans: All the above
⚡️GOAL: identifying Treatable Target⚡️
📌Rule out PIGN prior to assigning IC-GN/ C3GN diagnosis
📌Hx driven work-up: Viral titers, Autoimmune/ Rheum. evaluation, Immune Cell Abnormality, etc
📌If no etiology is found--> assess complement dysregulation
⚡️GOAL: identifying Treatable Target⚡️
📌Rule out PIGN prior to assigning IC-GN/ C3GN diagnosis
📌Hx driven work-up: Viral titers, Autoimmune/ Rheum. evaluation, Immune Cell Abnormality, etc
📌If no etiology is found--> assess complement dysregulation

13/💥 Kidney Biopsy in IC-MPGN shows:
⚡️LM: Mesangial proliferation and GBM thickening.
“smashed blueberry pancake” appearance - by @Trumidor
⚡️IF: C3 deposits + Ig deposits
⚡️EM: Mesangial proliferation, GBM thickening, mesangial deposits
⚡️LM: Mesangial proliferation and GBM thickening.
“smashed blueberry pancake” appearance - by @Trumidor
⚡️IF: C3 deposits + Ig deposits
⚡️EM: Mesangial proliferation, GBM thickening, mesangial deposits


14/ 💥Rx: treating the etiology, ↓ underlying immune dysregulation & burden of HTN & proteinuria
⚡️No curative option
⚡Mostly expert-opinion based Rx data
⚡️RAASi, HTN & Lipid-lowering agents - all
⚡️Steroids, MMF & rarely CNI
⚡️PLEX, Rituximab, Eculizumab- inconsistent data
⚡️No curative option
⚡Mostly expert-opinion based Rx data
⚡️RAASi, HTN & Lipid-lowering agents - all
⚡️Steroids, MMF & rarely CNI
⚡️PLEX, Rituximab, Eculizumab- inconsistent data

15/ 💥Prognosis:
⚡️pediatric pts with IC-MPGN/ C3G have better outcomes than adults
⚡️Progression to advanced CKD- rare in children
⚡️HTN & proteinuria remain suboptimally controlled
⚡️Poor prognosis: NS, low eGFR at the onset, persistent HTN & chronic changes on biopsy
⚡️pediatric pts with IC-MPGN/ C3G have better outcomes than adults
⚡️Progression to advanced CKD- rare in children
⚡️HTN & proteinuria remain suboptimally controlled
⚡️Poor prognosis: NS, low eGFR at the onset, persistent HTN & chronic changes on biopsy

16/💥Thank you for scrolling till the end!
For case-based discussion on this topic logon to @ASPNeph January pathology webinar
Until next time…
#MOC2credits
#FellowFOAMgroup #pediatricnephrology
@pedsnephrology @Trumidor @kidnyhealth @priti899 @RoshanPGeorgeMD
For case-based discussion on this topic logon to @ASPNeph January pathology webinar
Until next time…
#MOC2credits
#FellowFOAMgroup #pediatricnephrology
@pedsnephrology @Trumidor @kidnyhealth @priti899 @RoshanPGeorgeMD
@rattibha unroll please
Loading suggestions...