

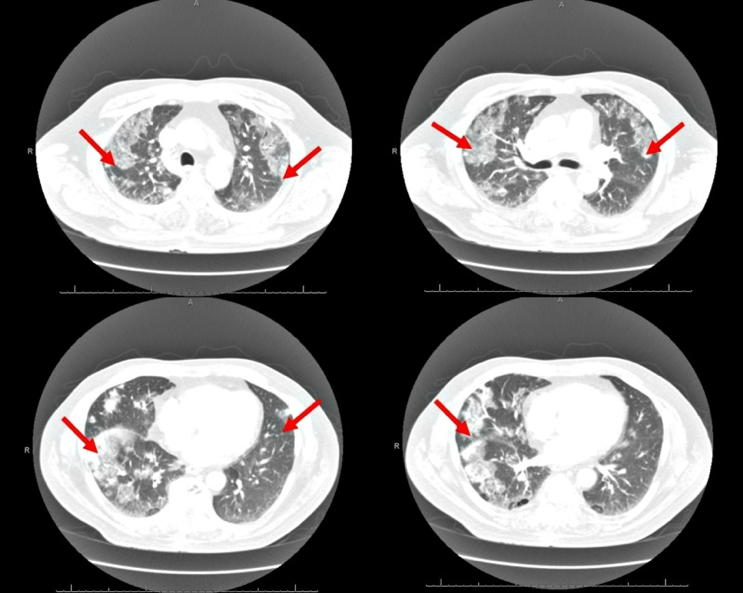
(1/10) Pt on D7 daptomycin (DAP) for MRSA 🩸 BSI develops dyspnea, fever 🥵, diffuse bilateral infiltrates on CXR. Intubated ➡️ Bronch w/BAL NGTD. WBC 12 (Neuts 0.6 / Eos 0.3 /Lymphs 0.18). Likely diagnosis?
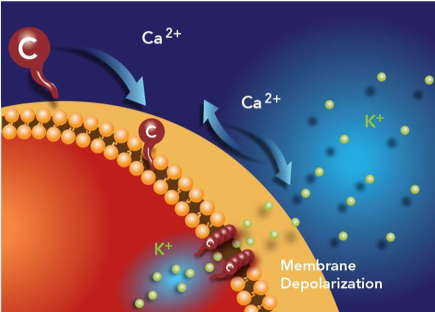
Let's start by exploring the DAP MOA🔨 DAP binds and depolarizes the cell membrane, allowing efflux of K+ ☠️. cubicin.com
(3/10) DAP is a workhorse 🐴 for MRSA, but this MOA results in 2 respiratory 🫁 tract problems.
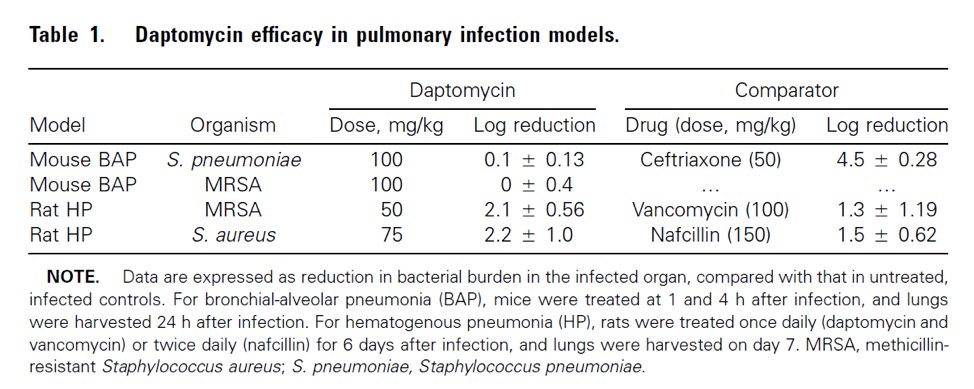
(4/10) #1 DAP is deactivated by lung surfactant making it ineffective for PNA. This 🐭 model demonstrates little/no DAP lung activity. 🤔pubmed.ncbi.nlm.nih.gov
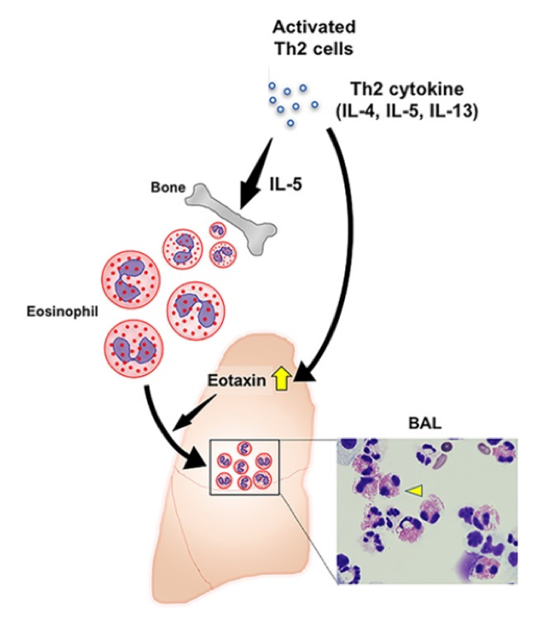
(5/10) #2: DAP interaction with surfactant ➡ inflammation ➡ T-cell activation ➡ IL-5 release ➡ eosinophil production ➡ eotaxin attraction of eosinophils to the 🫁. (Picture: onlinelibrary.wiley.com)
(6/10) DAP-induced eosinophilic PNA (AEP) should be suspected with DAP exposure + >25% eosinophils in bronch +🌡️ fever + 😮💨 dyspnea + new diffuse bilateral infiltrates on CT/CXR. ncbi.nlm.nih.gov
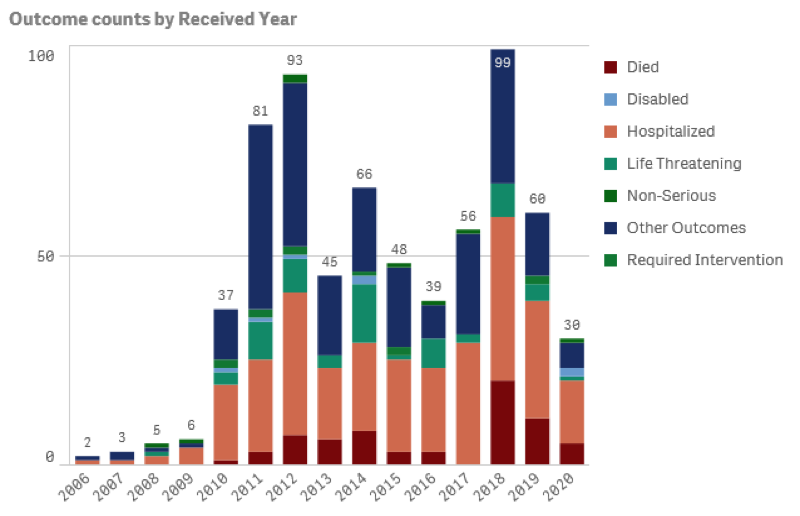
(7/10) There are <700 FAERS reports of DAP AEP over 15 years, with a majority of patients requiring hospitalization 🏥 and intervention. (fis.fda.gov)
(8/10) Common🧵? Incidence independent of dose (4-10 mg/kg), median duration of therapy 2.8 weeks, 77% pts had ⬆️ peripheral EOS. Resolution occurred within ⌛️48-72 hours DAP D/C. aricjournal.biomedcentral.com
(9/10) Management: ❌ stop daptomycin. Consider corticosteroids: IV methylprednisolone 💉 60-125 mg Q6H ➡ 💊 prednisone 40-60 mg taper over 2-6 weeks. DAP rechallenge not 🙅 recommended. aricjournal.biomedcentral.com
(10/10) Recap:
1⃣AEP is a serious ADE of DAP and is under-reported
2⃣DAP attracted to alveolar surfactant ➡ inflammation recruits eosinophils
3⃣Mgmt = Discontinue DAP and consider corticosteroids
4⃣DAP rechallenge NOT recommended
1⃣AEP is a serious ADE of DAP and is under-reported
2⃣DAP attracted to alveolar surfactant ➡ inflammation recruits eosinophils
3⃣Mgmt = Discontinue DAP and consider corticosteroids
4⃣DAP rechallenge NOT recommended
Loading suggestions...