

1/9
For #ICUproviders, #neurologyresidents and other providers that don't do brain death testing on the regular, a quick #tweetortial on optimizing your patient! (My first #tweetorial!) #MedEd #endneurophobia #critcare #NeuroTwitterNetwork #neurotwitter @NMatch2021
For #ICUproviders, #neurologyresidents and other providers that don't do brain death testing on the regular, a quick #tweetortial on optimizing your patient! (My first #tweetorial!) #MedEd #endneurophobia #critcare #NeuroTwitterNetwork #neurotwitter @NMatch2021

2/9
2/8nfirm that the patient has a reason to have complete cessation of ALL brain function; this means evaluating that the lesion is NOT just resulting in coma or locked-in state. The pt cannot have facial injuries or baseline cranial nerve deficits that interfere w/ testing
2/8nfirm that the patient has a reason to have complete cessation of ALL brain function; this means evaluating that the lesion is NOT just resulting in coma or locked-in state. The pt cannot have facial injuries or baseline cranial nerve deficits that interfere w/ testing
3/9
No confounders allowed! Patient needs to be 5 half-lives from the last sedation and paralytics, confirm w/ train of 4. In drug cases of drug overdoses repeat Utoxs may be requested. Major metabolic derangements (uremia, hyperammonemia, etc) also a no-no. Hypernatremia ok.
No confounders allowed! Patient needs to be 5 half-lives from the last sedation and paralytics, confirm w/ train of 4. In drug cases of drug overdoses repeat Utoxs may be requested. Major metabolic derangements (uremia, hyperammonemia, etc) also a no-no. Hypernatremia ok.
4/9
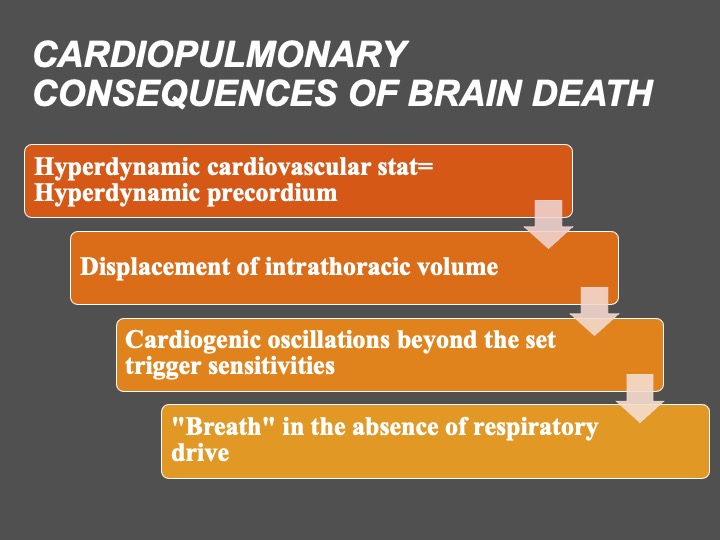
Sometimes we hear from teams that it seems like the patient meets all criteria, but... they are triggering the vent?
This can be a false finding!!!!!! The cardiac cycle may be triggering the vent if the vent is set at a sensitive flow or pressure trigger
Sometimes we hear from teams that it seems like the patient meets all criteria, but... they are triggering the vent?
This can be a false finding!!!!!! The cardiac cycle may be triggering the vent if the vent is set at a sensitive flow or pressure trigger
5/9
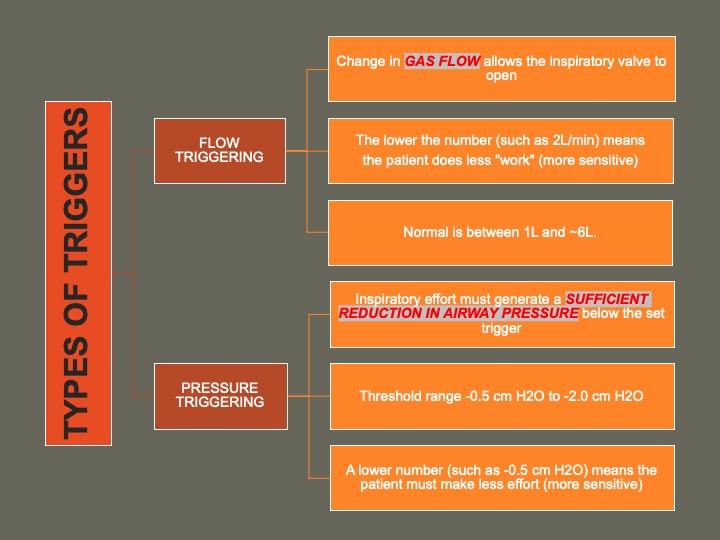
To confirm that they are really not breathing, set the flow or pressure trigger higher (for example, Flow to 6L/min). And now see if they are triggering breaths.
See slide that explains how vent triggers work:
To confirm that they are really not breathing, set the flow or pressure trigger higher (for example, Flow to 6L/min). And now see if they are triggering breaths.
See slide that explains how vent triggers work:

6/9
Watch out for Diabetes Insipidus! Herniation can cause major UOP and cause the patient to go into shock. Protocols differ but if you see clear urine and UOP>200ccx2 hours, it's time to check STAT urine Osm/serum Na.
Watch out for Diabetes Insipidus! Herniation can cause major UOP and cause the patient to go into shock. Protocols differ but if you see clear urine and UOP>200ccx2 hours, it's time to check STAT urine Osm/serum Na.
7/9
If Uosm<100 and serum sodium rising, consider Vasopressin 5u IV (lasts ~6h) & starting a vaso got (@ 0.5-1u/hour, not the shock dosing). Institutions differ on protocols 4 central DI, ok to manage differently; but, make sure you are keeping I=O to prevent shock!
If Uosm<100 and serum sodium rising, consider Vasopressin 5u IV (lasts ~6h) & starting a vaso got (@ 0.5-1u/hour, not the shock dosing). Institutions differ on protocols 4 central DI, ok to manage differently; but, make sure you are keeping I=O to prevent shock!
8/9
Patients must be warm (>36 degrees), hemodynamically stable (pressers are ok, SBP>100), and normocapnic (pCO2 35-45). Apnea testing will require that they have been preoxygenated.
Patients must be warm (>36 degrees), hemodynamically stable (pressers are ok, SBP>100), and normocapnic (pCO2 35-45). Apnea testing will require that they have been preoxygenated.
9/9
Ready for testing! @aan and @NeurocritCareJ have online tools and checklists to use. Always have an exam completed by an experienced provider. Miss anything? @JackieKraft4 @feras_akbik @Capt_Ammonia
Ready for testing! @aan and @NeurocritCareJ have online tools and checklists to use. Always have an exam completed by an experienced provider. Miss anything? @JackieKraft4 @feras_akbik @Capt_Ammonia
Loading suggestions...