

It's time folks! Welcome to this week's CbD! Tonight we have the fantastic @aswinchari as our moderator 🧠👏 look out for the code word that will be required for the feedback form to receive certificates of participation... and with that, let get started!
1. A 19 y/o male presents to a district general hospital ED after being hit over the top of the head by a baseball bat. He was walking in the park with his friends when this happened and believes it was a case of mistaken identity.

He loses consciousness temporarily, but wakes up within a few seconds, and vomits. His friends rush him into the emergency department. Based on this history, what are your thoughts on a differential diagnosis?
3. Great work guys! Some differentials include: extradural haematoma, subdural haematoma, subarachnoid haemorrhage, depressed skull fracture, traumatic brain injury, transient ischemia attack, intracranial abscess.
4. On arrival in ED, the patient is assessed by the nursing staff. The patient is alert and oriented to time, place, person. He’s chatting and able to move his whole body. He recalls the events of this afternoon quite well. What would you like to do?
5. Good work folks, you request a CT head. A non-contrast CT scan is the most common imaging modality to assess for intracranial bleeding. Guidelines exist to determine those who require an immediate CT or those requiring a CT within 8 hours of injury, see table!
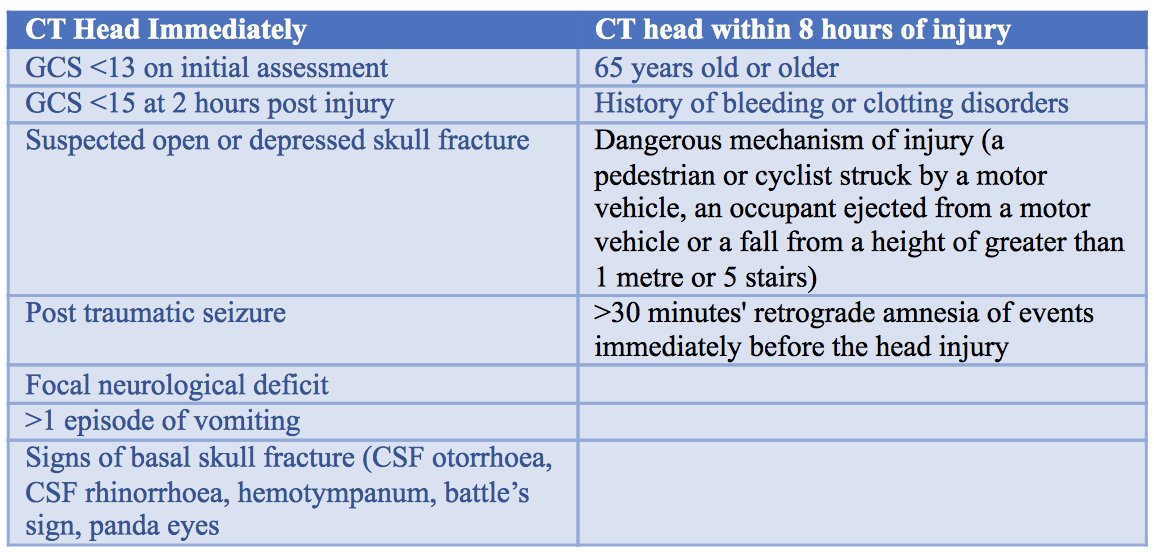
6. Given his dangerous mechanism of injury, and the loss of consciousness, a CT head is performed. What does it show?
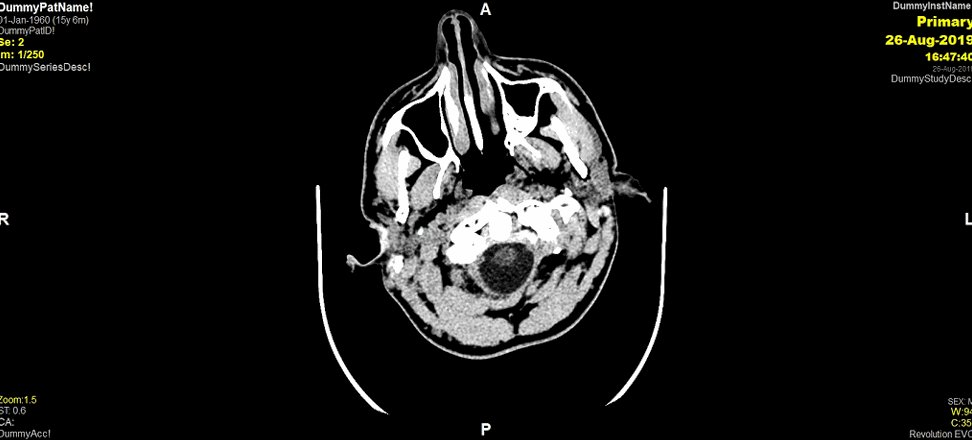
7. Indeed! The CTH shows a L sided EDH. You’ll see from this scan there is no effacement of the ventricles nor midline shift. Because of the findings, you refer him to the on-call neurosurgeon. They are in a hospital 45 mins away. What would you ask if you were that neurosurgeon?

8. You need to establish the duration of time between the injury and the scan, ask about the C-spine/ imaging of C-spine available, neurological exam findings, current observations and recommend continuation of neuro-observations, is the patient on anti-coagulants, DH, PMH
9. You have the option of transferring the patient to a neurosurgical centre or keeping him locally for monitoring. Who wants to transfer and who wants the patient to remain at the district general hospital?

10. Bingo! You decide to transfer the patient. The transfer team arrive to the ED and the patient begins his journey to the neurosurgical centre. Not long into the journey you get a call from the ambulance expressing some concern for the patient...

11. They tell you the patient is only able to move his left side. The patients left arm and leg withdraws from painful stimuli. His eyes are closed and only opens them in response to pain. He is making mumbling noises....
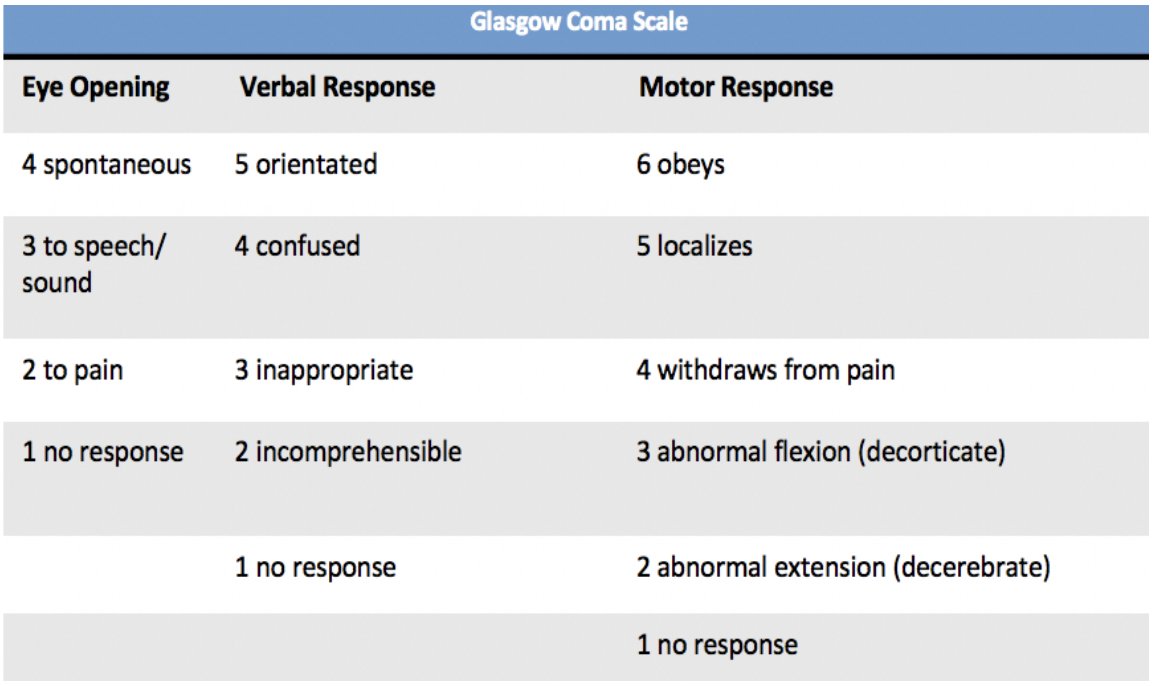
12. Based on the above information, what is his GCS?

Well done guys! The patient has a GCS of 8 (E2 V2 M4). Check out our video here which goes through a detailed examination of the GCS! youtube.com
14. What do you think the transfer team did next in terms of assessing the patient?
15. Absolutely right! The team performed an ABCDE assessment. Initial assessment begins with evaluation of airway, breathing and circulation. An organised approach ensures a complete assessment of head injury.

16. The patients airway is patent. Respiratory rate is 18 breaths/ minute and heart rate is 64 breaths/min. BP is 136/86 mmHg. Pupils are equal and reactive. Is there any speciality you think should be involved at this point/ made aware of the patient?
17. Anaesthetics yes! This is for intubation and mechanical ventilation. Patients with a low conscious level may lack protective airway reflexes and require a definitive airway. A GCS of 8 or less should be considered as such a risk and should be intubated.
18. Luckily you have ensured that there is an anaesthetist with the transfer team. She intubates and mechanically ventilates the patient. Just after the anaesthetist intubates the patient, you get a call saying his left pupil is now blown. What does this mean?

19. So this is a fixed dilated pupil. Most likely due to Uncal (trans-tentorial) herniation....
20. You're one step ahead guys! ...anyone know what uncal herniation is and what is the cause?

21. Uncal herniation occurs when rising ICP causes herniation of the medial temporal lobe from the middle into the posterior fossa, across the tentorial opening. The uncus herniates over the tentorial notch compressing the third cranial nerve located just medial to the uncus.
22. Who knows why pupillary dilatation is often the first sign in uncal herniation?

23. As the parasympathetic fibres are on the outside of the third nerve, the first sign of uncal herniation is usually pupillary dilation...

24. Does anyone know of any other herniation syndromes?

25. Subfalcine herniation (brain extends under the falx cerebri), tonsillar (inferior descent of the cerebellar tonsils below the foramen magnum, central (diencephalon (thalamus and hypothalamus) and medial parts of temporal lobe are forced through a notch in tentorium cerebelli.
26. Really excellent work on the last question guys! What a clever bunch we've got! So moving on, what would you recommend the transferring team to do for this?

27. Raise head of bed to 30 degrees, Mannitol prescription: 0.25-1 g/kg over <20 mins. If the patient had a cervical collar you would consider loosening or removing it. Continue neuro-obs...
28. You call up the receiving hospital and suggest the patient needs a repeat CT scan, why is this appropriate in this case?

29. Well done guys! The accepting neurosurgeon informs you she is going to prepare CT and theatres so that the ambulance team can go straight from the ambulance bay to CT then up to theatres.
30. The results from the head CT are shown below. What do you see?

31. Good work guys! The CT scan demonstrates progression of the L sided EDH, with midline shift and effacement of the ventricles. As a little reminder here is the first CTH we performed. You can see the rapid progression in the extra-axial collection...

31. On neuro-imaging, extradural haematomas give a biconvex/elliptical/ lentiform shape. Does anyone know why this is? (gif inspired by @AbbieTutt!)
32. Extradural haematoma’s (EDH’s) are extra-axial collections. This means they are external to the brain parenchyma. Because they collect between the suture lines of the cranium, they give this elliptical shape!

33. Quick guys! Here is the code word required for the feedback form at the end. Take note! The word is.... pupil

34. So, back to work... who knows where exactly extradural haematomas form?

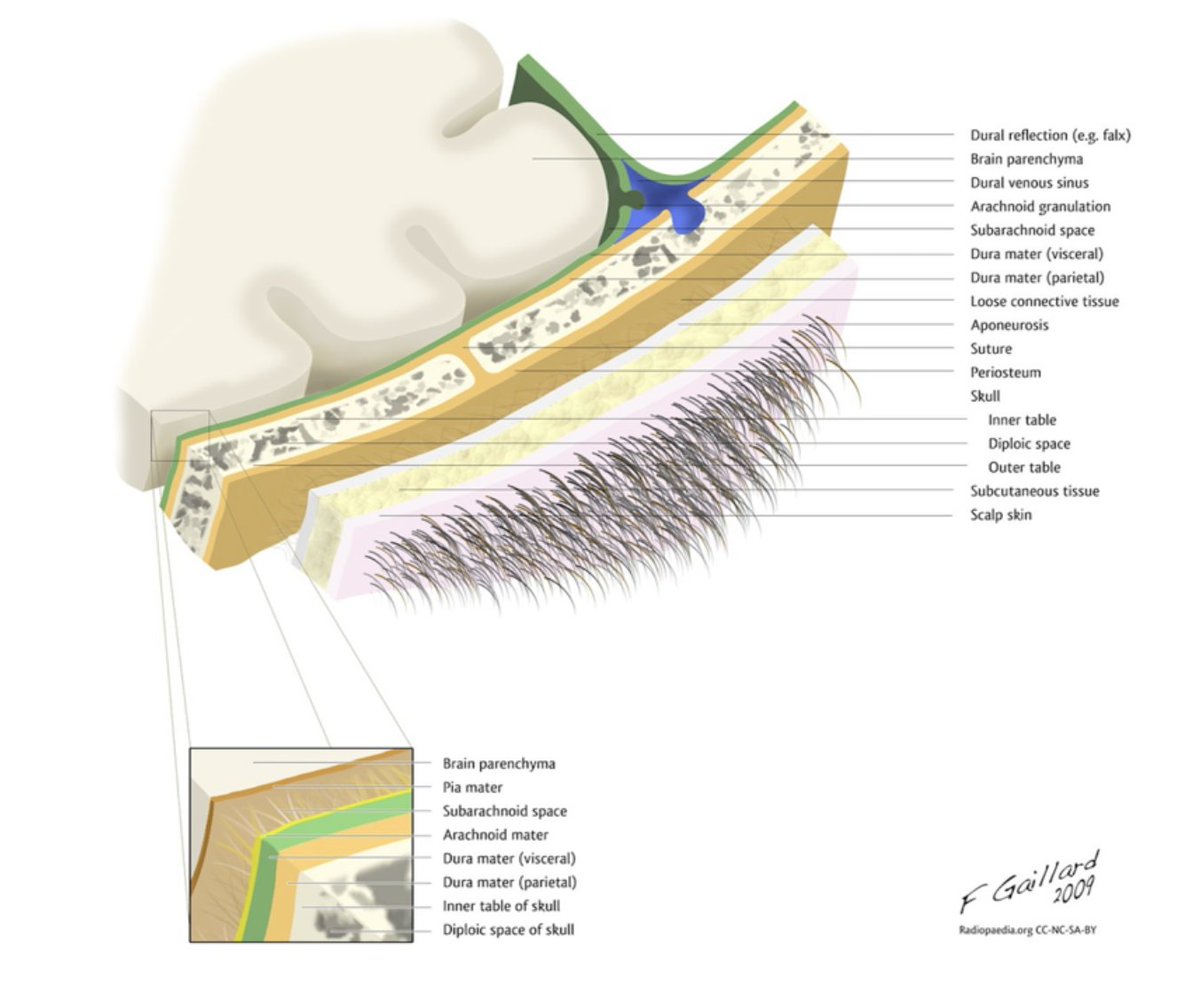
35. They form between the skull and the dura mater. The dura mater is the outermost layer of meninges. Meninges are the membranous covering of the brain and spinal cord. The dura is thick, tough and inextensible and lies directly underneath the bones of the skull...

36. Within the cranial cavity, the dura consists of two connective tissue sheets: periosteal and meningeal layer. The periosteal layer lines the inner surface of the bones of the cranium; the meningeal layer lies deep to the periosteal layer in the cranial cavity...
37. There are three meningeal layers. Who can name the other two for us and describe their location?
38. Well done guys! Pia and arachanoid mater. The arachanoid is the middle layer, lying directly underneath the dura. The pia mater lies below the arachnoid mater and is tightly adhered to the surface of the brain.
39. Who knows which vessel is commonly involved in an extradural haematoma?

40. Spot on! The middle meningeal artery. The middle meningeal artery is a branch of the maxillary artery. The maxillary artery is one of the terminal branches of the external carotid artery.
41. The majority of the time, EDH’s are associated with skull fractures. Due to the location of the middle meningeal artery, tears typically occur during trauma to the lateral aspect of the skull. Who knows which part of the skull the middle meningeal artery overlies?

42. Well done guys! EDHs usually form under the pterion. This is a fragile segment of bone at the junction of the frontal, temporal, parietal and sphenoid bones.

43. It’s also important to note that extradural haematomas can also occur from injury to the diploic veins or the venous sinuses. These often present in a delayed fashion and are often more difficult to treat.

44. So how do extradural haematomas normally present then?

45. They present similar to our patient, patients typically present with an initial loss of consciousness following the trauma then a complete transient recovery known as the ‘lucid interval’. This is then followed by a rapid neurological deterioration.
46. EDHs are often a neurosurgical emergency. This is because arterial bleeding results in a rapid accumulation of blood in the extradural space. The enlarging haematoma leads to an elevation in the ICP. Progression to brain herniation can occur rapidly.
47. So how do we treat extradural haematomas?
48. Great stuff guys! Treatment for EDH include surgical or non-surgical management. Non-surgical management involves serial CT scans and close neurological observation. Surgical management includes a craniotomy to evacuate the clot.

49. So how do we know when to operate? Any thoughts?
50. Well the decision is made on the patients level of consciousness (GCS), CT head findings, pupillary abnormalities and neurological deterioration. Below is the criteria...

51. It is decided to take the patient to theatre for a craniotomy and evacuation of the extradural haematoma. To find out how we perform this surgery, click this link to here! youtu.be
52. Who knows any complications of a craniotomy we look out for?
53. Complications include bleeding intra-operatively and post-operatively, seizure, hydrocephalus, meningitis, neurological deficit related to the area of surgery, coma, death.
54. The EDH is successfully evacuated and the patient is transferred to the neuro-observations ward where he is monitored. A post-operative CT shows complete evacuation of the haematoma and resolution of midline shift.
55. Once the operation has finished, what else do you need to think about?

56. Safeguarding! – talk to your hospital safeguarding team about whether we need to report the incident and what needs to be done to ensure the patient and family/friends are safe.

57. On post-operative day 3 the patient is mobilising well on the ward and is fit for discharge. Before he is discharged, is there anything you might want to advise him on regarding driving?

58. Contact the DVLA. A head injury often requires 6-12 months off driving and is dependent on a number of factors so it’s important to inform the DVLA and seek advice.
59. And that's a wrap! Amazing work guys, you clever bunch! And a BIG thank you to @aswinchari for his amazing words of wisdom 👏 Here is the feedback form to complete in order to receive your certificates of participation (don't forget the code word!) forms.gle
60. See you next time guys!

Loading suggestions...