
1/ Do data support pt trial off sedation for “SAT” when pt is comfortable on current dose? Yes
Shared w permission:
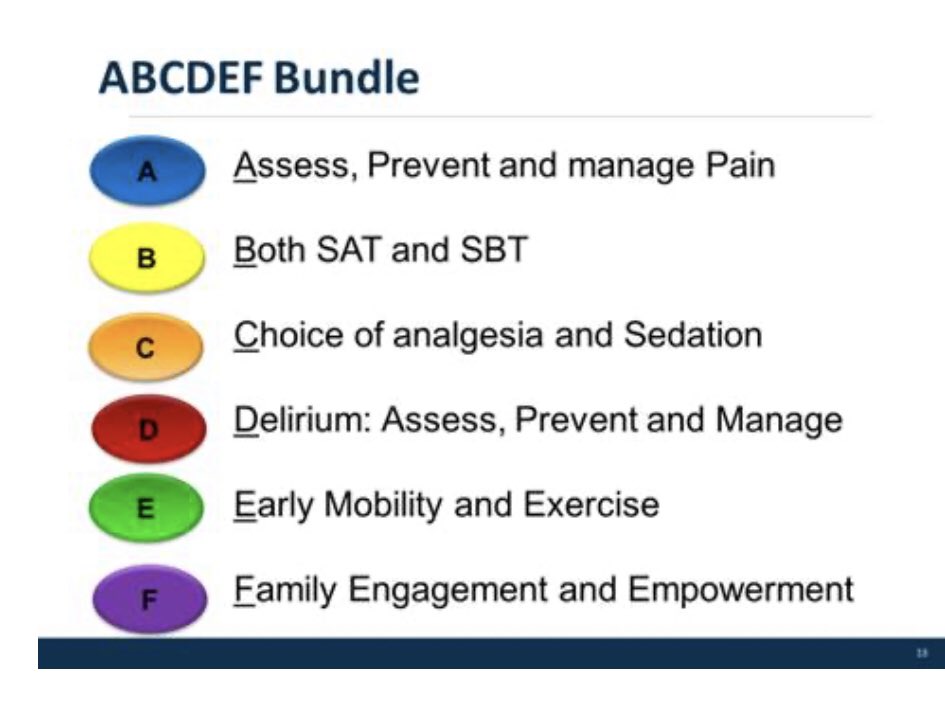
“Dr. Ely, yesterday our ICU #nurses went over #A2Fbundle in Epic for implementation. Do you recommend SAT at RASS Goal of RASS -1 to +1?
#medtwitter #criticalcare
Shared w permission:
“Dr. Ely, yesterday our ICU #nurses went over #A2Fbundle in Epic for implementation. Do you recommend SAT at RASS Goal of RASS -1 to +1?
#medtwitter #criticalcare
2/ Excellent #Nurse added:
“We are currently not doing SAT (Spontaneous Awakening Trial) but keeping pt’s RASS -1 to +1. Just want to make sure we are interpreting #A2Fbundle correctly.”
#TipsForNewDocs
#medstudenttwitter #COVID19 #pandemic
“We are currently not doing SAT (Spontaneous Awakening Trial) but keeping pt’s RASS -1 to +1. Just want to make sure we are interpreting #A2Fbundle correctly.”
#TipsForNewDocs
#medstudenttwitter #COVID19 #pandemic
3/ my Answers:
Great questions. I don’t think +1 (anxiety) is ever a good goal but 0 to -1 is a 👍 default target RASS if we acknowledge there are times when sedation target should acceptably be set as deep as -3/-4 in bad #ARDS or -5 transiently when pt requires paralytics.
Great questions. I don’t think +1 (anxiety) is ever a good goal but 0 to -1 is a 👍 default target RASS if we acknowledge there are times when sedation target should acceptably be set as deep as -3/-4 in bad #ARDS or -5 transiently when pt requires paralytics.
4/ Some HCPs use philosophy that if pt is already “at goal” why shut drugs off?
Well...what if target is wrong? Also, if a drug isn’t needed, it may be hurting a person & costing $$ unnecessarily. Bottom line: you won’t know if it’s needed until you stop it EVERY DAY w SAT.
Well...what if target is wrong? Also, if a drug isn’t needed, it may be hurting a person & costing $$ unnecessarily. Bottom line: you won’t know if it’s needed until you stop it EVERY DAY w SAT.
5/ Data say stop sedation once a day even if at target. Restart as needed at half previous dose. That’s how we designed our Girard T 2008 ABC study in @TheLancet, which showed BIG survival advantage to SATs.
7/fin
Committing pts to more drug doesn’t make sense data-wise or to me as a doc since I can safely test need via an SAT. Assuming pts need more sedation is a sentence in favor of more immobilization, #delirium, ultimately more #dementia & #death.
#A2Fbundle = #humanization
Committing pts to more drug doesn’t make sense data-wise or to me as a doc since I can safely test need via an SAT. Assuming pts need more sedation is a sentence in favor of more immobilization, #delirium, ultimately more #dementia & #death.
#A2Fbundle = #humanization
@threadreaderapp please unroll
Loading suggestions...