
What will you do for this 50yo active male with an isolated closed pelvic ring injury? He was injured 2 days ago and has been HD stable and neuro normal since injury.
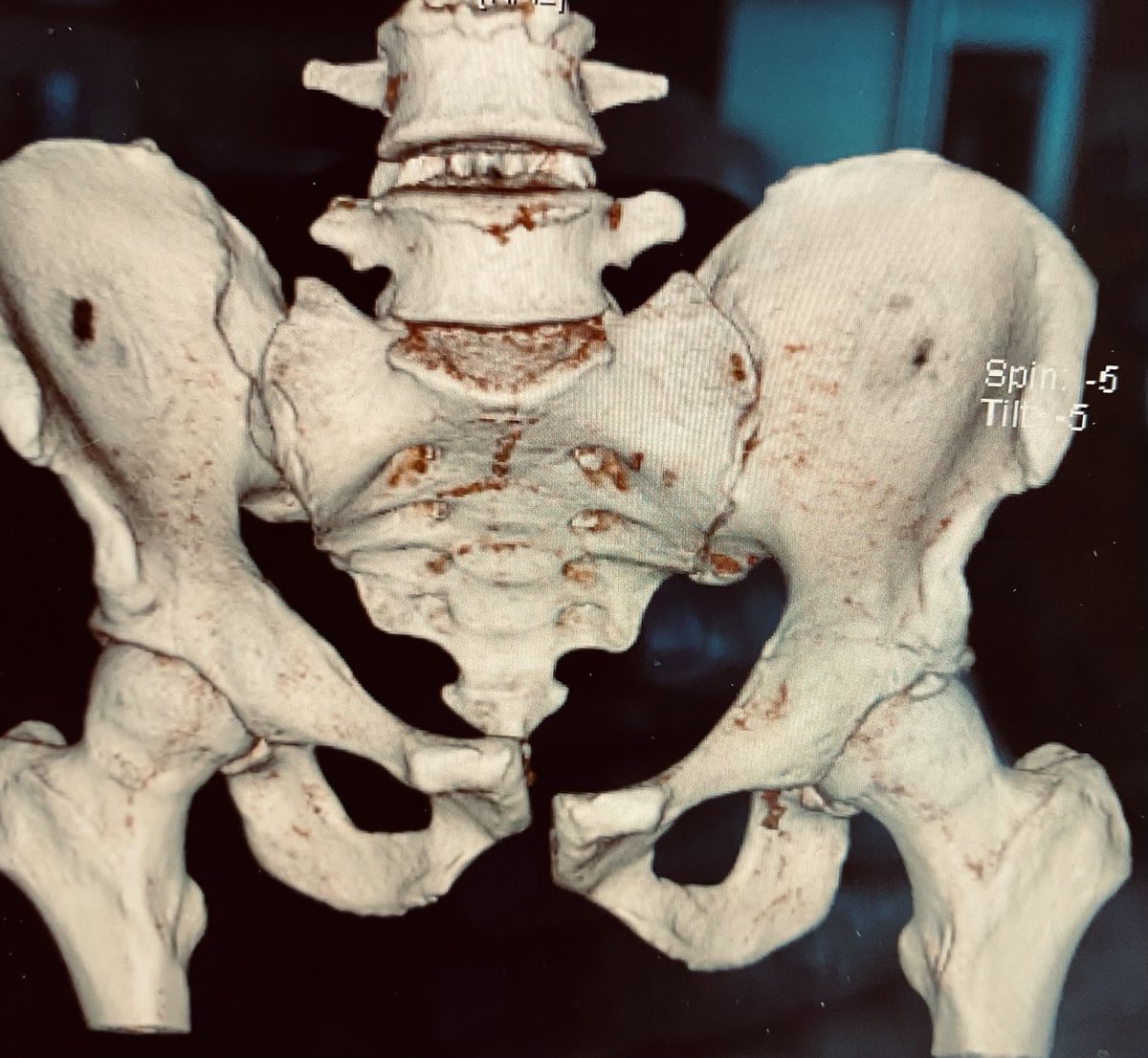
Here is an upper sacral level axial CT image
The posterior pelvis injury is seen as well in this axial CT image at the second sacral level

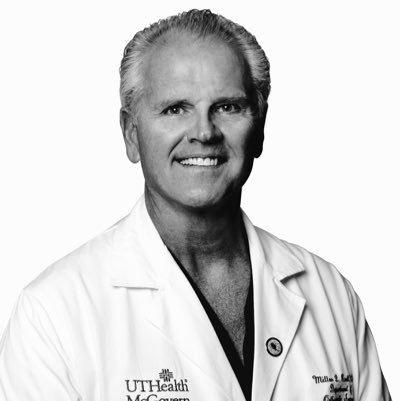
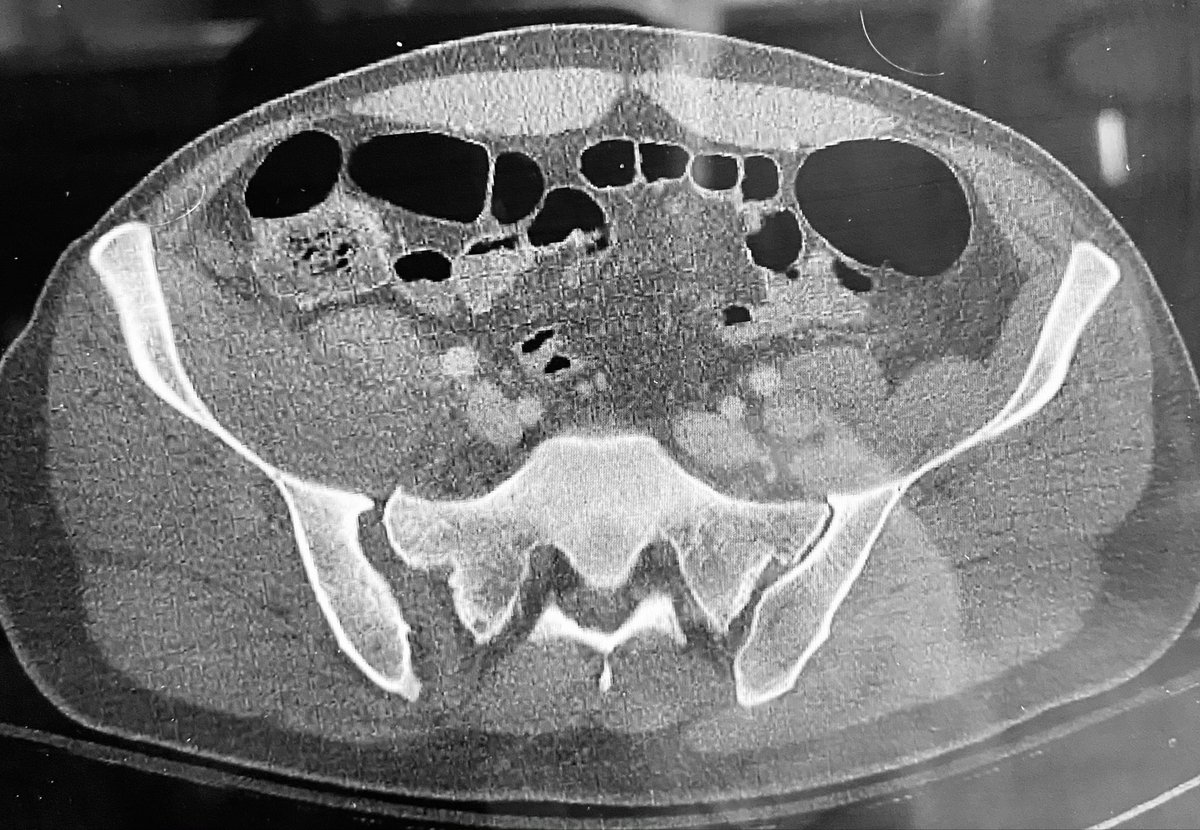
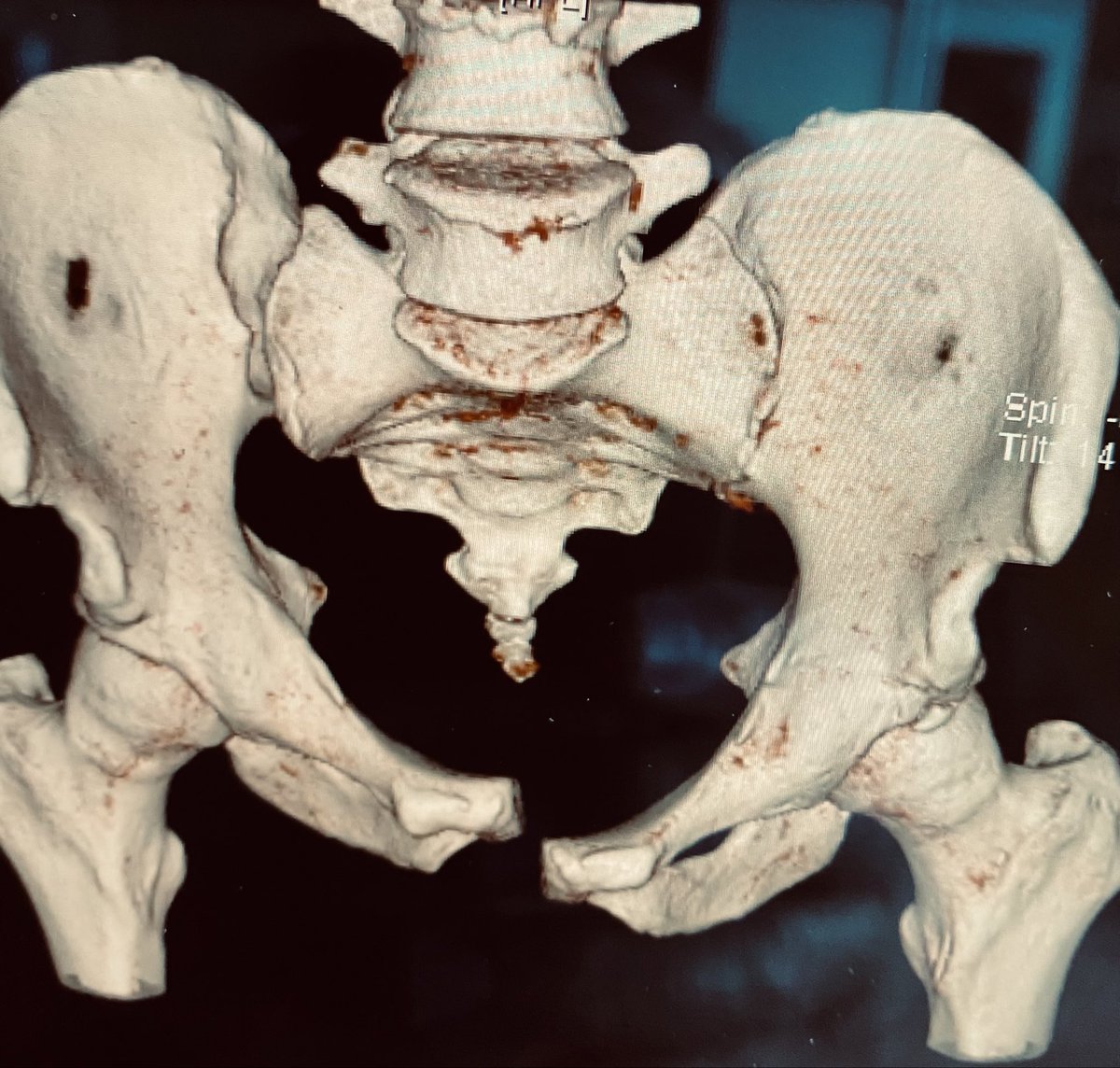
This surface rendered pelvic inlet image demonstrates the right hemipelvic displacement and deformity
With the patient positioned supine, his pelvic region elevated 2-3” on a soft sacral midline support of folded blankets, in 15# of right distal femoral traction, and fully relaxed under GA, this is the right hemipelvic displacement and deformity - how do you use this info?

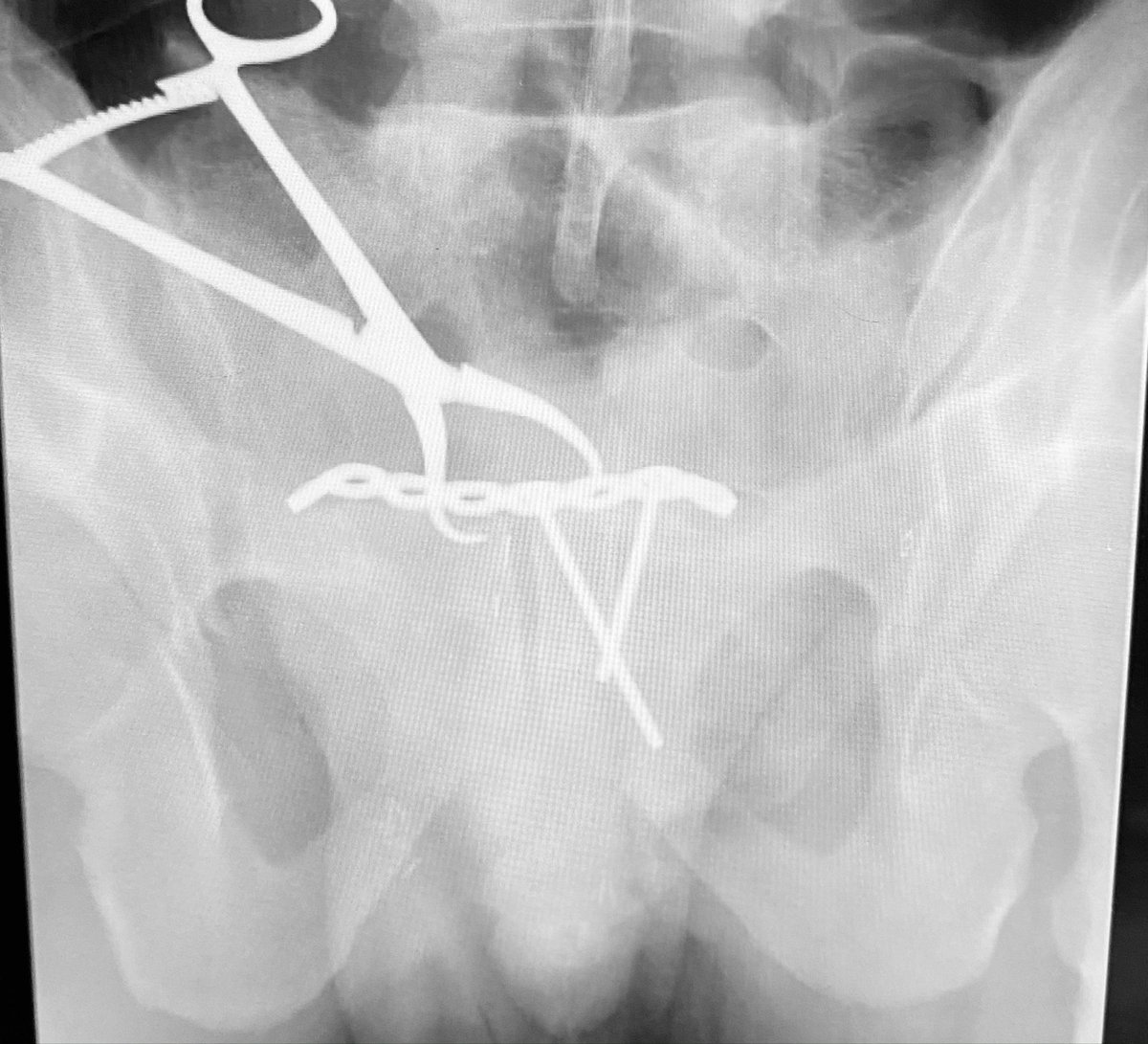
The vector of the tenaculum clamp needed to correct the deformity obstructed plating. So we contoured and secured the plate on the left side and then applied the reduction clamp again vectored as necessary to achieve and maintain the reduction

Another view to show the plate and clamp locations
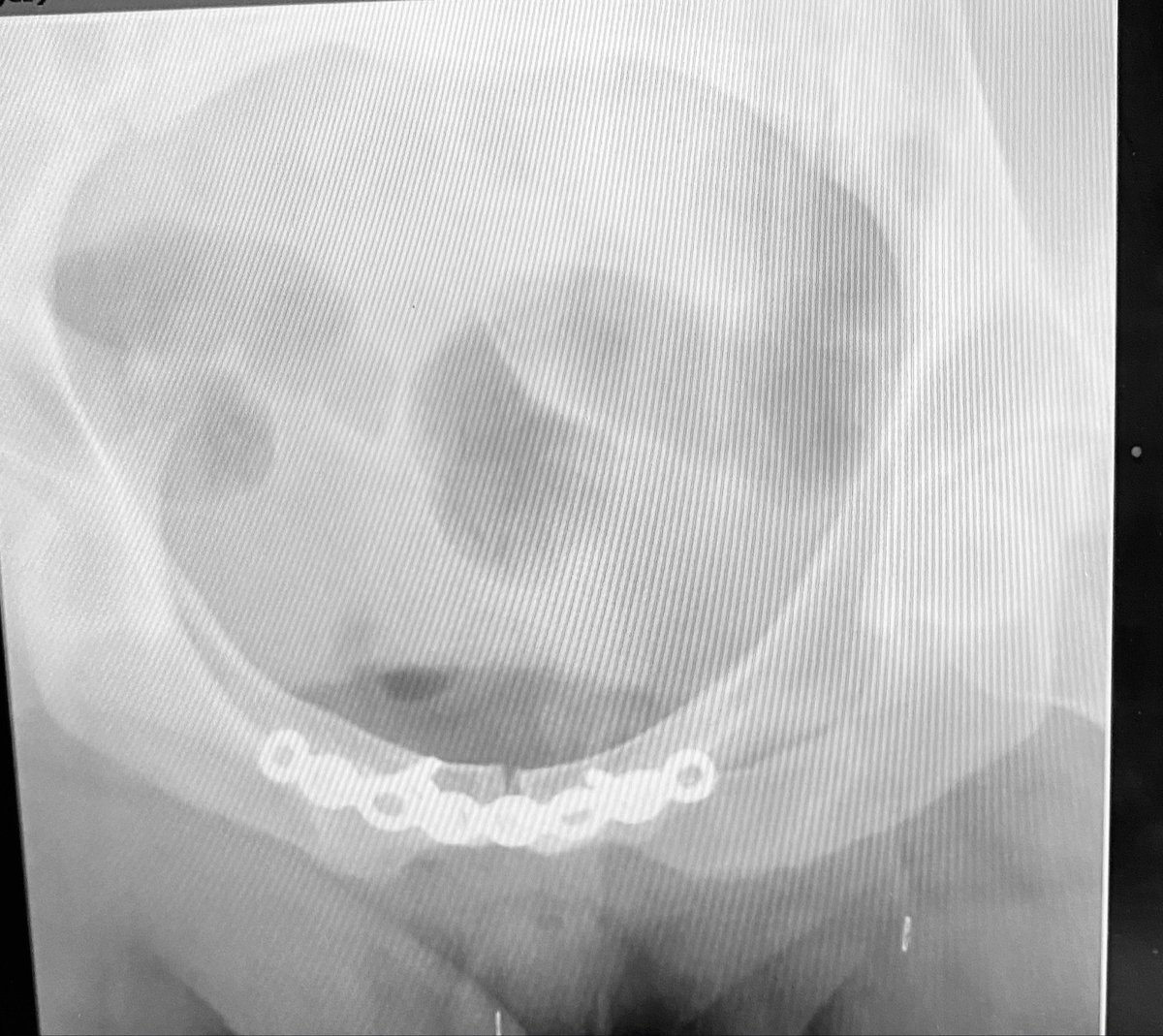
We added more fixation screws to the plate and removed the clamp - is the SI joint sufficiently indirectly reduced for lag screw compression? If so, how do you determine this? Or will this SI joint need ORIF?

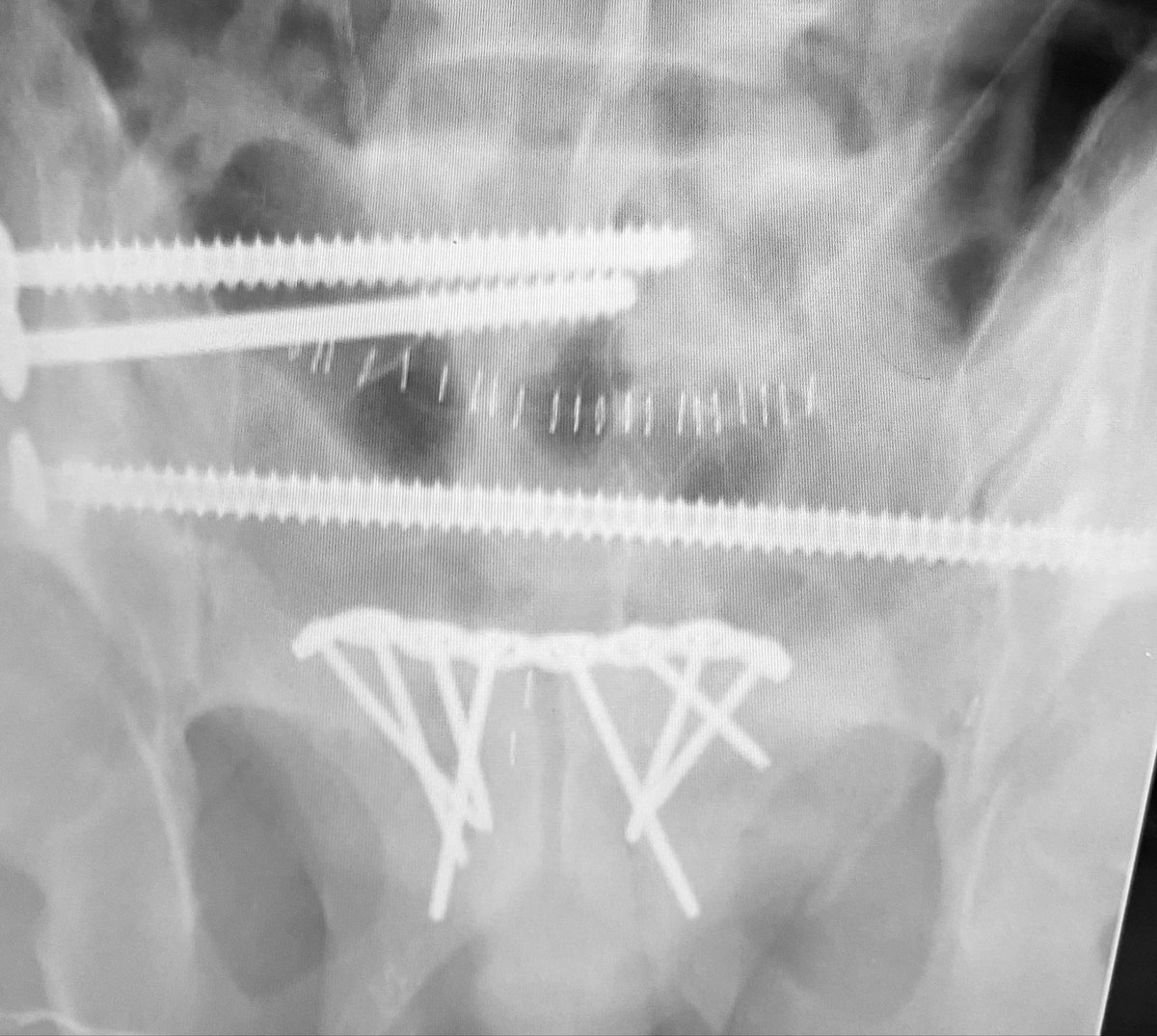
We assess the SI indirect reduction to be essentially purely distracted based on numerous tangential images - we then used an upper sacral segment cannulated iliosacral lag screw over a washer to finally reduce/compress the injured SI joint

Additional fully threaded iliosacral screws were added within the safe osseus fixation pathways to further stabilize the posterior pelvic injury
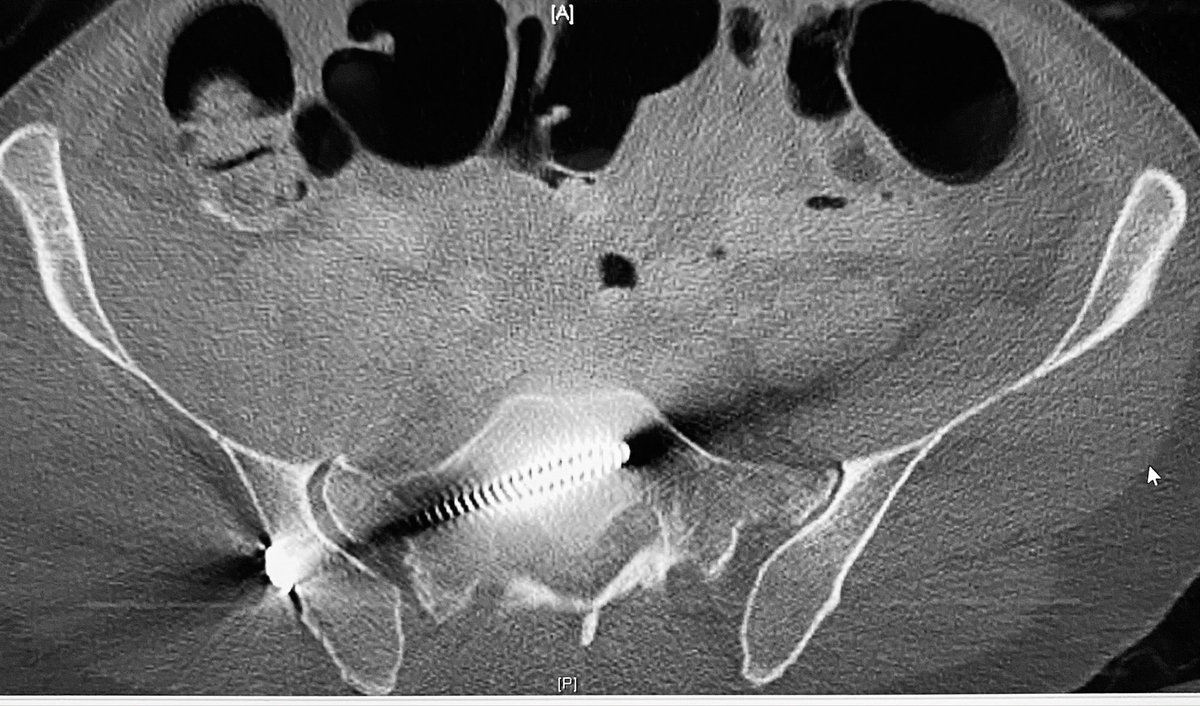
The postop CT axial images reveal the indirect reduction quality and implant location details

Loading suggestions...