

1/15 #EHRA_ESC Tweetorial
#EPeeps, has been some time since our last guidelines tweetorial, we will go back to 2019 today. Let's have a look at the 2019 @escardio Guidelines for the management of patients with supraventricular tachycardia #SVT.
#EHRA_Ecomm @RodrigueGarcia4
#EPeeps, has been some time since our last guidelines tweetorial, we will go back to 2019 today. Let's have a look at the 2019 @escardio Guidelines for the management of patients with supraventricular tachycardia #SVT.
#EHRA_Ecomm @RodrigueGarcia4
2/15
Find the full text document here 👉
academic.oup.com
The last 📚guidelines about SVT were published in 2003 and then needed to be updated! As the present guidelines are very broad, we will focus on the crucial points and the main changes.
Find the full text document here 👉
academic.oup.com
The last 📚guidelines about SVT were published in 2003 and then needed to be updated! As the present guidelines are very broad, we will focus on the crucial points and the main changes.
3/15
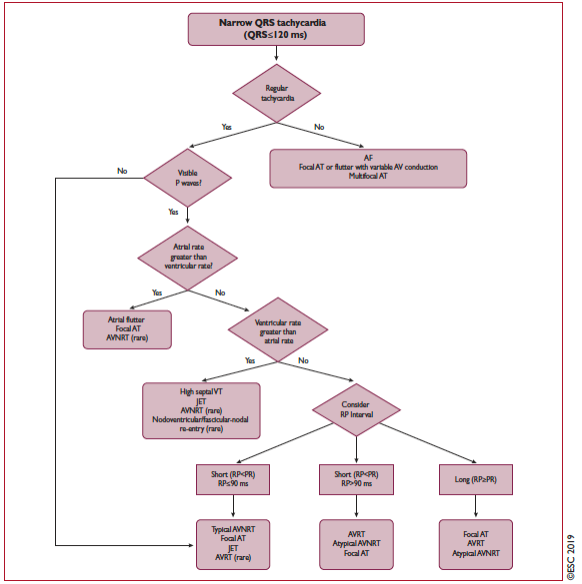
Let's start with the basics: differential diagnosis of narrow QRS tachycardia. Be careful ⚠️⚠️⚠️ , the only trick is that, VT may be relatively narrow QRS when emerging from the high septum !
Let's start with the basics: differential diagnosis of narrow QRS tachycardia. Be careful ⚠️⚠️⚠️ , the only trick is that, VT may be relatively narrow QRS when emerging from the high septum !
4/15
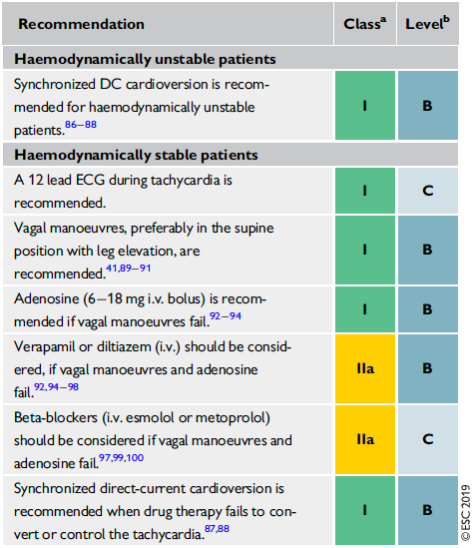
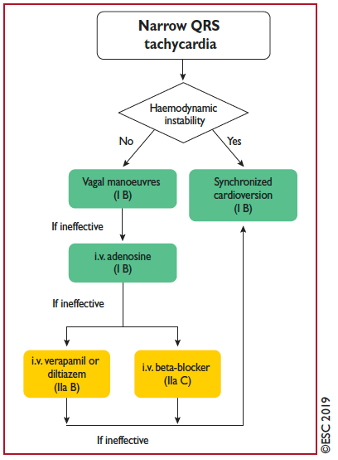
The management of narrow QRS tachycardia in the absence of an established diagnosis depends on the hemodynamic stability of the patient. 1️⃣ Vagal manoeuvres first, 2️⃣ adenosine second, 3️⃣ verapamil, diltiazem and beta-blockers 3rd! Note that the dose of adenosine is 6-18mg
The management of narrow QRS tachycardia in the absence of an established diagnosis depends on the hemodynamic stability of the patient. 1️⃣ Vagal manoeuvres first, 2️⃣ adenosine second, 3️⃣ verapamil, diltiazem and beta-blockers 3rd! Note that the dose of adenosine is 6-18mg
5/15
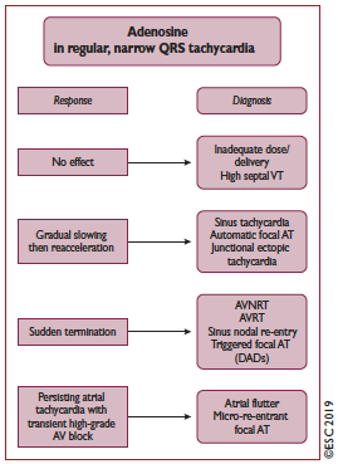
Vagal manoeuvres and adenosine might be very helpful for the diagnosis in case of narrow QRS tachycardia. If you are a fan, check out this 📺 #relVideo" target="_blank" rel="noopener" onclick="event.stopPropagation()">thelancet.com @TheLancet
Vagal manoeuvres and adenosine might be very helpful for the diagnosis in case of narrow QRS tachycardia. If you are a fan, check out this 📺 #relVideo" target="_blank" rel="noopener" onclick="event.stopPropagation()">thelancet.com @TheLancet
6/15
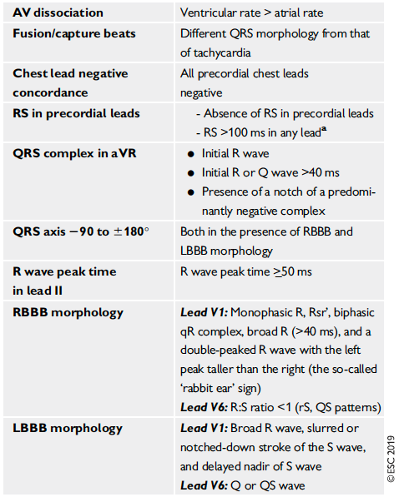
Now, let's complicate things! Wide complex tachycardia might be VT, SVT conducting with BBB aberration, or antegrade conduction over an AP (with reported proportions of 80, 15, and 5%, respectively), preexisting BBB, PMT, or other DD. Here are some 🔑 criteria suggesting VT:
Now, let's complicate things! Wide complex tachycardia might be VT, SVT conducting with BBB aberration, or antegrade conduction over an AP (with reported proportions of 80, 15, and 5%, respectively), preexisting BBB, PMT, or other DD. Here are some 🔑 criteria suggesting VT:
7/15
Management of wide complex tachycardia depends also on hemodynamic stability. If hemodynamic is stable, 1️⃣ vagal manoeuvres first, 2️⃣ adenosine second, 3️⃣ procainamide 3rd! Amiodarone has a IIb class (see 8/15). But never amio first!!!
Management of wide complex tachycardia depends also on hemodynamic stability. If hemodynamic is stable, 1️⃣ vagal manoeuvres first, 2️⃣ adenosine second, 3️⃣ procainamide 3rd! Amiodarone has a IIb class (see 8/15). But never amio first!!!

8/15
If you are not familiar with procainamide, you can check 👀the PROCAMIO study
academic.oup.com.
Compared to IV amiodarone, IV procainamide was safer and more effective to reduce wide complex tachycardia 😯
If you are not familiar with procainamide, you can check 👀the PROCAMIO study
academic.oup.com.
Compared to IV amiodarone, IV procainamide was safer and more effective to reduce wide complex tachycardia 😯
9/15
Inappropr sinus tachy (IST) is a sinus rhythm >100bpm @ rest or min activity out of prop with the level of physical,emotional,pathological stress. ⚠️Prognosis is benign👉Reassurance, exercise training, vol expansion, avoidance of cardiac stimulants. academic.oup.com
Inappropr sinus tachy (IST) is a sinus rhythm >100bpm @ rest or min activity out of prop with the level of physical,emotional,pathological stress. ⚠️Prognosis is benign👉Reassurance, exercise training, vol expansion, avoidance of cardiac stimulants. academic.oup.com

10/15
IST is not Postural orthostatic tachycardia syndrome (POTS)which is an ↗️HR ≥30 bpm when standing >30 s + an absence of orthostatic hypotension (>20 mmHg drop in SBP). Non-pharmacological treatments should be attempted first in all patients. sciencedirect.com
IST is not Postural orthostatic tachycardia syndrome (POTS)which is an ↗️HR ≥30 bpm when standing >30 s + an absence of orthostatic hypotension (>20 mmHg drop in SBP). Non-pharmacological treatments should be attempted first in all patients. sciencedirect.com
11/15
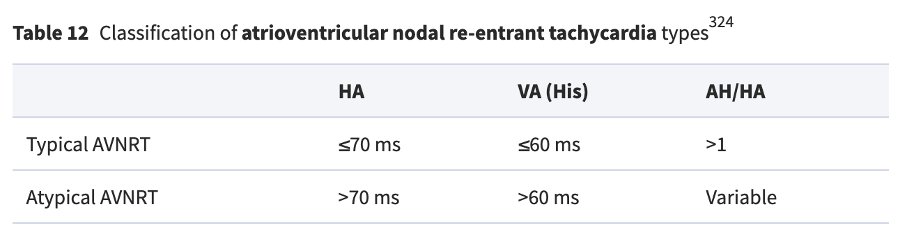
AVNRT denotes re-entry in the area of the AVN, but the exact circuit remains elusive. Atypical AVNRT is seen in ∼6% of all AVNRT cases, and in some patients may coexist with the typical form.
Different forms of AVNRT 🤨 during an EPS 👇
AVNRT denotes re-entry in the area of the AVN, but the exact circuit remains elusive. Atypical AVNRT is seen in ∼6% of all AVNRT cases, and in some patients may coexist with the typical form.
Different forms of AVNRT 🤨 during an EPS 👇
12/15
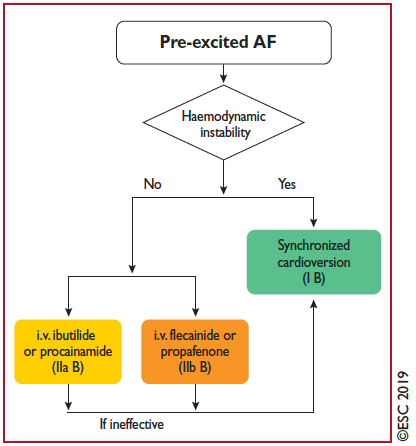
Let's move to AVRT. You will find different algorithms 🤯 for the localization of the AP in the guidelines. Regarding #AF and AVRT, acute management can be stressful 😓. Keep in mind that in case of hemodynamic instability, a cardioversion is recommended ⚡️
Let's move to AVRT. You will find different algorithms 🤯 for the localization of the AP in the guidelines. Regarding #AF and AVRT, acute management can be stressful 😓. Keep in mind that in case of hemodynamic instability, a cardioversion is recommended ⚡️
13/15
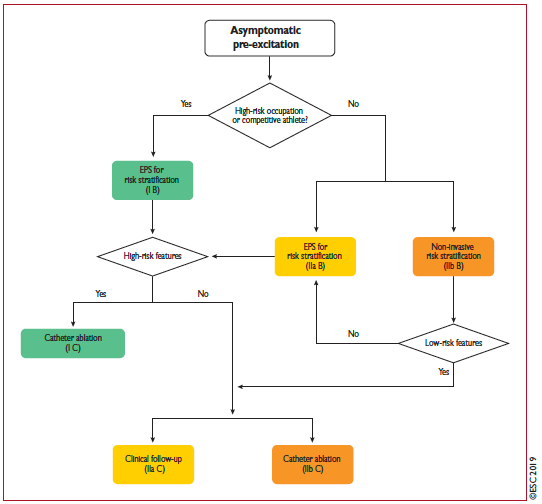
Let's focus on a!symptomatic pre-excitation. SCD secondary to pre-excited AF conducting rapidly over the AP resulting in VF is the most feared. If the patient has a high-risk occupation (pilot/professional driver) or is a competitive athlete, an EPS is recommended (IB).
Let's focus on a!symptomatic pre-excitation. SCD secondary to pre-excited AF conducting rapidly over the AP resulting in VF is the most feared. If the patient has a high-risk occupation (pilot/professional driver) or is a competitive athlete, an EPS is recommended (IB).
14/15
Features associated with an increased risk of SCD include younger age, inducibility of AVRT, multiple APs, and shortest pre-excited RR interval during AF ≤250 ms at baseline or antegrade effective refractory period ≤250 ms.
Features associated with an increased risk of SCD include younger age, inducibility of AVRT, multiple APs, and shortest pre-excited RR interval during AF ≤250 ms at baseline or antegrade effective refractory period ≤250 ms.
15/15
These were just short excerpts.
See the full text of the 2019 @escardio Guidelines on SVT here:
academic.oup.com
See you all at the #EHRA2021 congress next week!
#EHRA_ESC #EHRA_Ecomm @RodrigueGarcia4 @DavidDuncker @Dominik_Linz @KommataVarvara @GuerraCardio
These were just short excerpts.
See the full text of the 2019 @escardio Guidelines on SVT here:
academic.oup.com
See you all at the #EHRA2021 congress next week!
#EHRA_ESC #EHRA_Ecomm @RodrigueGarcia4 @DavidDuncker @Dominik_Linz @KommataVarvara @GuerraCardio
Loading suggestions...