

1/ Ready for a #Tweetorial on coronary artery calcium (CAC) score?
Keep reading to:
☢️Understand the pathophysiology of coronary artery calcium
☢ Identify the utility of the CAC score
☢️Recognize the limitations of CAC scoring
Keep reading to:
☢️Understand the pathophysiology of coronary artery calcium
☢ Identify the utility of the CAC score
☢️Recognize the limitations of CAC scoring
2/ How do you feel about the following statement:
I understand the utility of CAC score and can recognize its strengths and limitations.
I understand the utility of CAC score and can recognize its strengths and limitations.
3/ Let's start with a case!
58 yo👨in office asks about future CVD risk and starting a statin. No angina. Family h/o early MI and 10-year risk-score = 9%. Uncertain about starting meds. In addition to lifestyle changes, next step?
58 yo👨in office asks about future CVD risk and starting a statin. No angina. Family h/o early MI and 10-year risk-score = 9%. Uncertain about starting meds. In addition to lifestyle changes, next step?
4/ In the ️patient above, CAC score is useful to assess role for 1⁰ prevention meds like statins
CAC is an active process:
🦴propagated by inflammation & mediators of oxidative stress
🦴affected by HLD & glucose
CAC is an anatomic measure of calcific plaque burden
CAC is an active process:
🦴propagated by inflammation & mediators of oxidative stress
🦴affected by HLD & glucose
CAC is an anatomic measure of calcific plaque burden

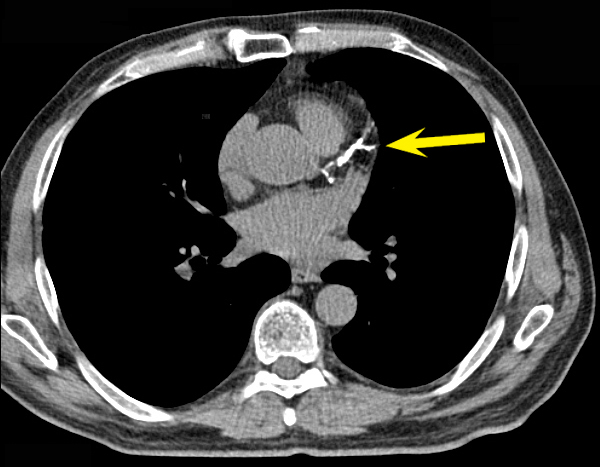
5/ How is CAC score calculated?
Agatston CAC Score is based on a weighted density score – we measure volume of plaque and multiply by a density factor
E.g: Lesion is 15 mm2 and 450 HU (Factor of 4), score is 60. All plaques are summed up to give a total score!
Agatston CAC Score is based on a weighted density score – we measure volume of plaque and multiply by a density factor
E.g: Lesion is 15 mm2 and 450 HU (Factor of 4), score is 60. All plaques are summed up to give a total score!

6/ ⁉️ When to use CAC ⁉️
Most evidence to help risk-stratify and aid in statin therapy decision
✅w/o DM & with LDL-C ≥70-189
✅10-yr ASCVD risk of 5%-20% (borderline-intermediate risk group)
NOT useful for pts with low risk (ASCVD <5%) or high risk (ASCVD >20%)
Most evidence to help risk-stratify and aid in statin therapy decision
✅w/o DM & with LDL-C ≥70-189
✅10-yr ASCVD risk of 5%-20% (borderline-intermediate risk group)
NOT useful for pts with low risk (ASCVD <5%) or high risk (ASCVD >20%)

7/ CAC comes back as 0🎉
Power of Zero➡️defer statin! But what's the "warranty period"
Powerful negative risk predictor, guidelines recommend rescan ~5-10 yrs
More nuanced: 3-7 yr warranty w/ CAC = 0 in MESA study. Timing may be based on risk/comorbidities (age&diabetes)
Power of Zero➡️defer statin! But what's the "warranty period"
Powerful negative risk predictor, guidelines recommend rescan ~5-10 yrs
More nuanced: 3-7 yr warranty w/ CAC = 0 in MESA study. Timing may be based on risk/comorbidities (age&diabetes)

8/ ☠️What about the opposite: CAC comes back as >1,000?☠️
CAC consortium study: 5x risk CVD, 2.8x risk all-cause mortality
Current guidelines have high risk as CAC >300-400, but CAC >1,000 may be distinct group w/ risk similar/📈 than traditional secondary prevention pts
CAC consortium study: 5x risk CVD, 2.8x risk all-cause mortality
Current guidelines have high risk as CAC >300-400, but CAC >1,000 may be distinct group w/ risk similar/📈 than traditional secondary prevention pts

9/ Is calcified plaque the whole story? No!
High risk features of plaque
💥location, diffuseness, bifurcation
💥necrotic core, low-attenuation plaque
💥intraplaque hemorrhage
💥thin fibrous cap
💥positive remodeling
💥spotty micro-calcification
💥macrophage infiltration
High risk features of plaque
💥location, diffuseness, bifurcation
💥necrotic core, low-attenuation plaque
💥intraplaque hemorrhage
💥thin fibrous cap
💥positive remodeling
💥spotty micro-calcification
💥macrophage infiltration
10/ Numerical CAC score can miss high-risk features
Ex: spotty calcification ⬆️ in pts w/ ACS when plaques also show +tive remodeling & low-attenuation
Some features can be assessed further by CT, OCT, IVUS
⬆️risk if >25% of the total score is in the left main coronary
Ex: spotty calcification ⬆️ in pts w/ ACS when plaques also show +tive remodeling & low-attenuation
Some features can be assessed further by CT, OCT, IVUS
⬆️risk if >25% of the total score is in the left main coronary

11/ What if pt is on statin? Does CAC have prognostic utility?
2018 AHA/ACC guidelines: no clinical utility
But CAC consortium retrospective analysis:
⬆️CAC w/ statins remains predictive of CVD mortality, though⬇️prognostic significance
Statins may impact CAC density
2018 AHA/ACC guidelines: no clinical utility
But CAC consortium retrospective analysis:
⬆️CAC w/ statins remains predictive of CVD mortality, though⬇️prognostic significance
Statins may impact CAC density

12/ Let’s Summarize:
CAC➡️highly specific feature of coronary atherosclerosis, use for borderline-intermediate risk pts
CAC=0➡️very strong⛔️predictive value for future CV events
CAC score ≥1,000➡️very aggressive LDL-C lowering
⚡️Limitations: can miss high risk features⚡️
CAC➡️highly specific feature of coronary atherosclerosis, use for borderline-intermediate risk pts
CAC=0➡️very strong⛔️predictive value for future CV events
CAC score ≥1,000➡️very aggressive LDL-C lowering
⚡️Limitations: can miss high risk features⚡️
13/ I feel comfortable with understanding the utility of CAC score and can recognize its strengths and limitations.
14/ I learned something in this Tweetorial that may change my clinical practice.
16/ Also check out the following infographic comparing and contrasting CAC score and CCTA
Thanks to the @cardionerds team for guidance and feedback, especially @EvelynSongMD & @karanpdesai
Thanks to the @cardionerds team for guidance and feedback, especially @EvelynSongMD & @karanpdesai

Loading suggestions...