

🔔LIVE NOW🔔
#MNIBDWebinar w @DCharabaty @EdwardLoftus2 @ibddocmaria
🎯🆕#SEAVUE data
🎯Future of #IBD #Crohns care
Tweet your 💬💭 w us!
🆓 #CME👉integrityce.com
Supported by an educational grant from @JanssenUS
integrityce.com
#MNIBDWebinar w @DCharabaty @EdwardLoftus2 @ibddocmaria
🎯🆕#SEAVUE data
🎯Future of #IBD #Crohns care
Tweet your 💬💭 w us!
🆓 #CME👉integrityce.com
Supported by an educational grant from @JanssenUS
integrityce.com
Post-#MNIBDwebinar #CME #IBDPoll2️⃣
You discuss therapies w a 65yoF w severe #Crohns. She has HTN, psoriasis, breast CA 3 yrs ago. She’s concerned about safety of meds w her PMH.
Based on recs on positioning Rx in Crohns by
@AmerGastroAssn which of the following do you recommend
You discuss therapies w a 65yoF w severe #Crohns. She has HTN, psoriasis, breast CA 3 yrs ago. She’s concerned about safety of meds w her PMH.
Based on recs on positioning Rx in Crohns by
@AmerGastroAssn which of the following do you recommend
Post-#MNIBDwebinar #CME #IBDPoll3️⃣
In the recent #SEAVUE head2head study, which of the following safety outcomes showed the widest numerical difference between UST treated vs ADAL treated pts w #Crohns, in favor w UST?
In the recent #SEAVUE head2head study, which of the following safety outcomes showed the widest numerical difference between UST treated vs ADAL treated pts w #Crohns, in favor w UST?
Post-#MNIBDwebinar #CME #IBDPoll4️⃣
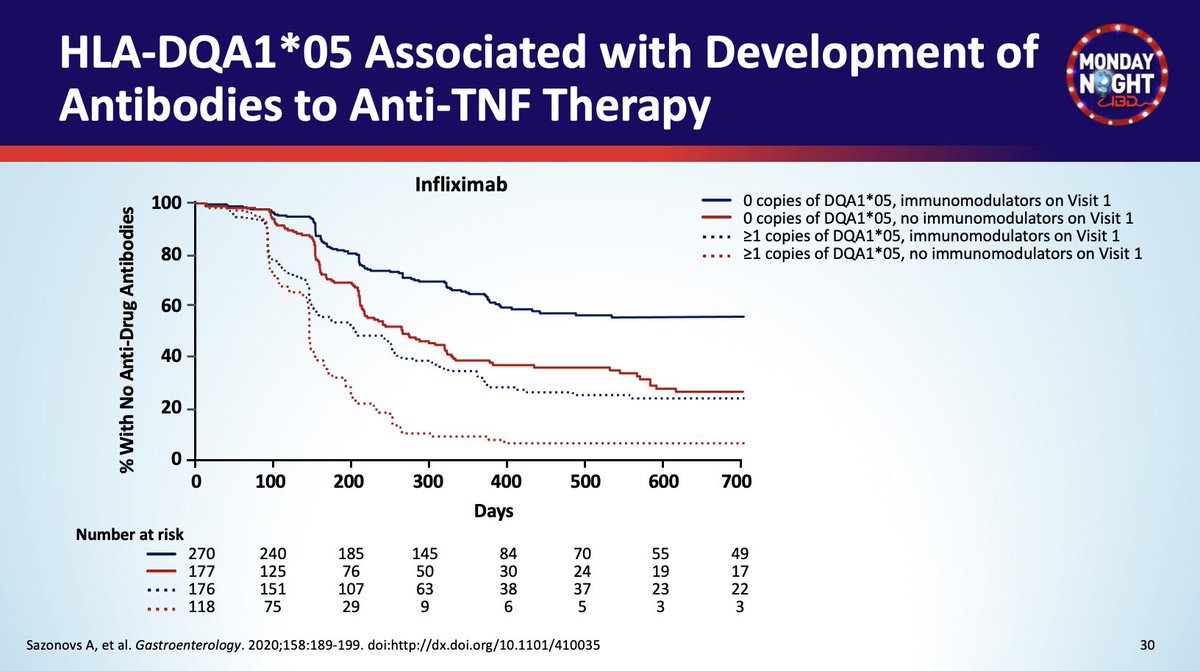
Which of the following baseline pt characteristics is associated with the highest risk of developing antibodies to TNFi in #IBD?
🧬 = HLA-DQA1*05
IMM = immunomodulator
Which of the following baseline pt characteristics is associated with the highest risk of developing antibodies to TNFi in #IBD?
🧬 = HLA-DQA1*05
IMM = immunomodulator
#MNIBDWebinar @DCharabaty
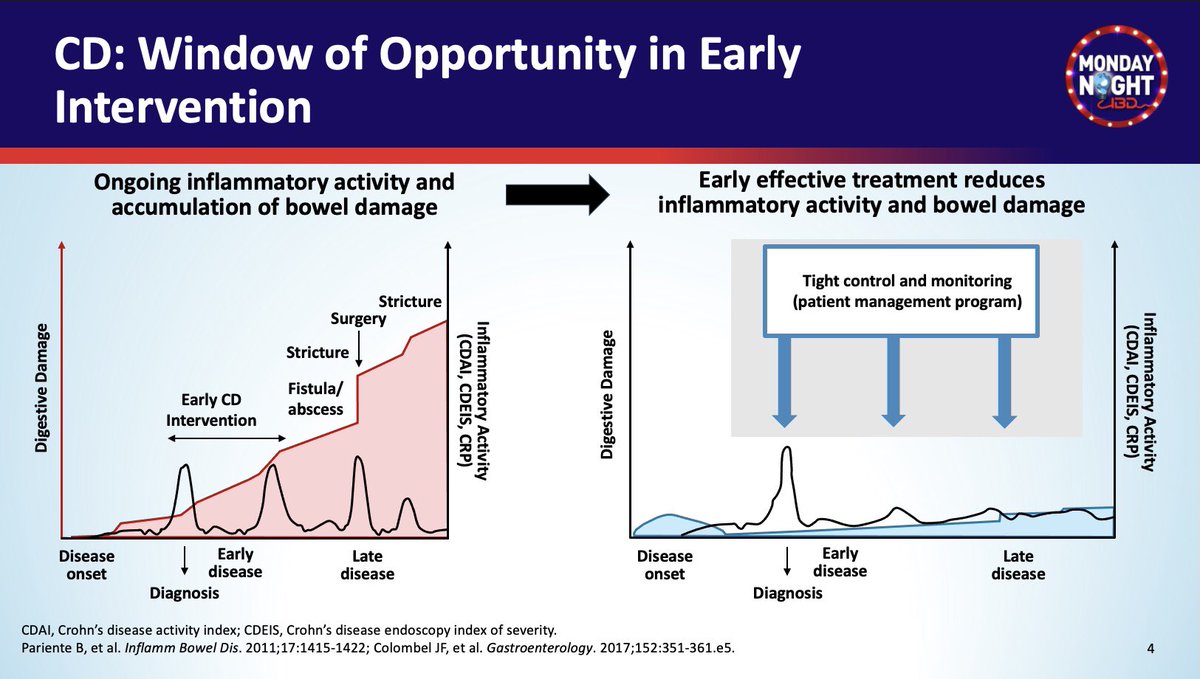
We have a 🪟of opportunity to 🚫 disease progression in #Crohns w
✅ Early intervention
✅ Effective therapies
✅ Tight disease control
✅ Tight monitoring & Treat to target 🎯 strategy
⏰Undertreated Crohn’s ▶️ Progression to stricture/fistula/ ✂️
We have a 🪟of opportunity to 🚫 disease progression in #Crohns w
✅ Early intervention
✅ Effective therapies
✅ Tight disease control
✅ Tight monitoring & Treat to target 🎯 strategy
⏰Undertreated Crohn’s ▶️ Progression to stricture/fistula/ ✂️
#MNIBDWebinar @DCharabaty
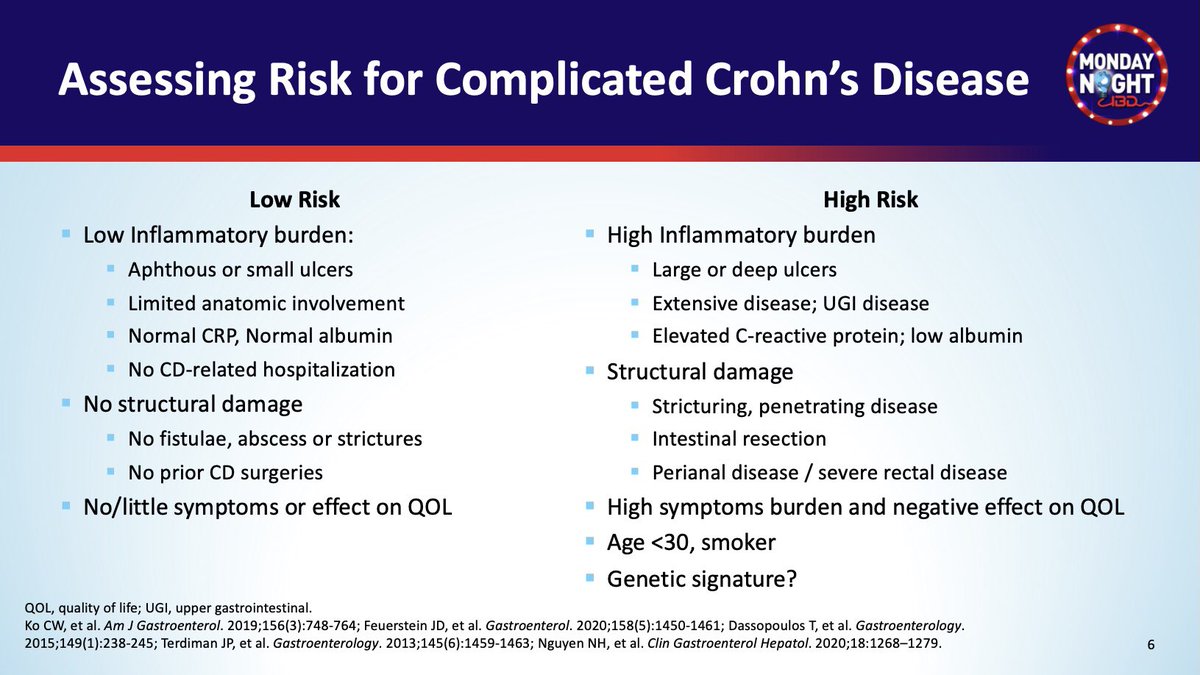
⏰Which pt is at risk of complication from #Crohns
✔️ Age <30, 🚬
✔️ High 🔥 burden on endo
✔️ High CRP, low albumin
✔️ Structural damage
✔️ Perianal disease
✔️ High symptoms burden
✔️ Genetic signature?
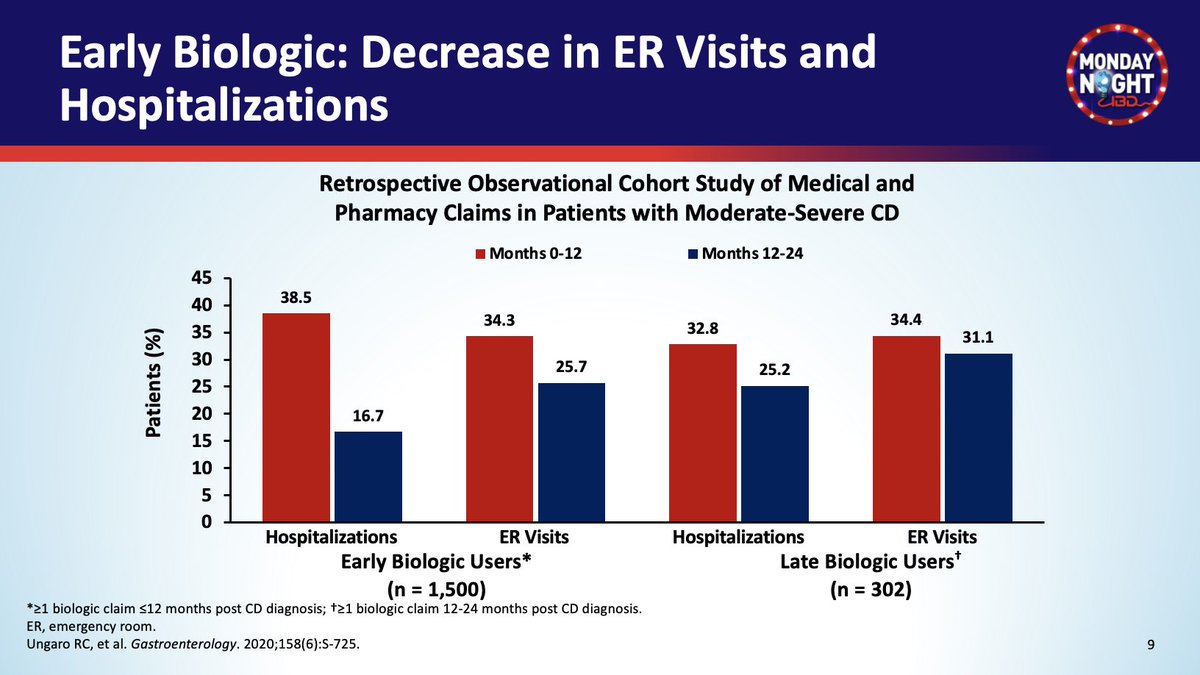
⏰ Early biologic use -> ⬇️ 🏨visits
⏰Which pt is at risk of complication from #Crohns
✔️ Age <30, 🚬
✔️ High 🔥 burden on endo
✔️ High CRP, low albumin
✔️ Structural damage
✔️ Perianal disease
✔️ High symptoms burden
✔️ Genetic signature?
⏰ Early biologic use -> ⬇️ 🏨visits
#MNIBDWebinar @DCharabaty
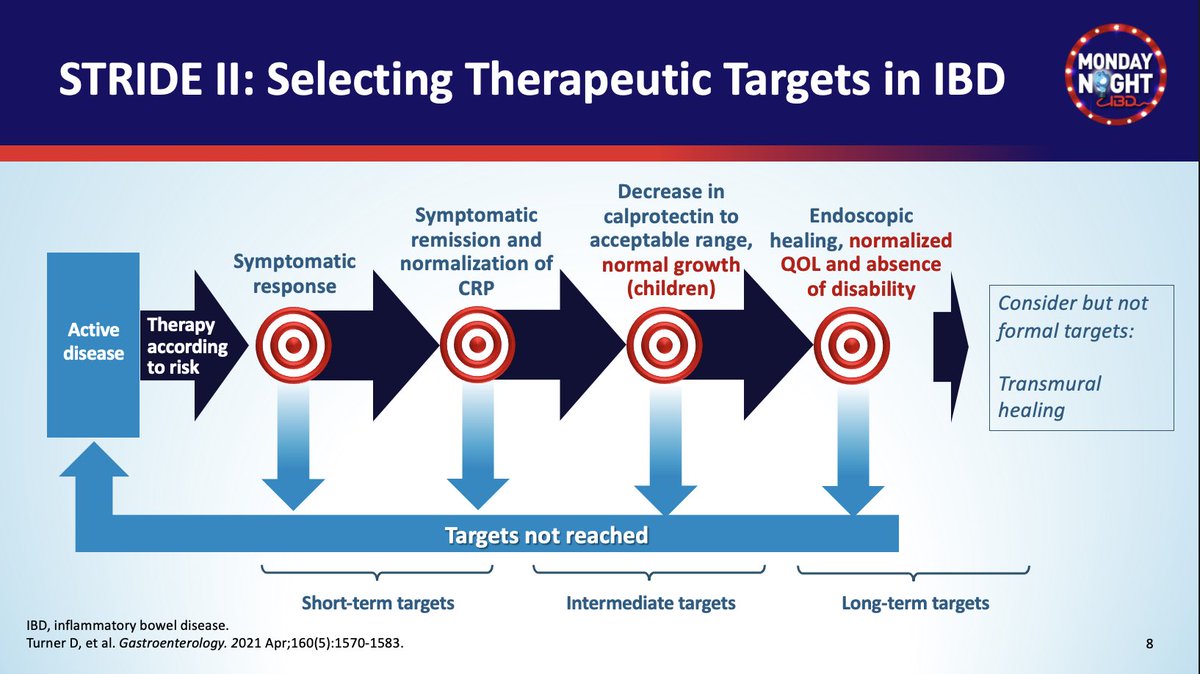
🎯 #STRIDE-II Selecting Therapeutic Targets in #IBD
✔️Symptoms response
✔️Symptoms resolution = Remission
✔️Normalization CRP, FCP⬇️⬇️
✔️Endo🔦healing
🆕 Nml growth in kids
🆕 Restoration of #QOL
🆕 🚫 Disability
@AGA_Gastro doi.org
🎯 #STRIDE-II Selecting Therapeutic Targets in #IBD
✔️Symptoms response
✔️Symptoms resolution = Remission
✔️Normalization CRP, FCP⬇️⬇️
✔️Endo🔦healing
🆕 Nml growth in kids
🆕 Restoration of #QOL
🆕 🚫 Disability
@AGA_Gastro doi.org
#MNIBDWebinar @DCharabaty
🪜Positioning therapies in #Crohns - Take into account
✔️Disease severity: 🔥🔥, structural damage, impact on QOL
✔️EIM
✔️Perianal disease
✔️Patient preferences
✔️Co-morbidities
✔️⚖️Risk - Benefit
👇🏽@AmerGastroAssn 1st & 2nd line Rx👇🏽@AGA_CGH
🪜Positioning therapies in #Crohns - Take into account
✔️Disease severity: 🔥🔥, structural damage, impact on QOL
✔️EIM
✔️Perianal disease
✔️Patient preferences
✔️Co-morbidities
✔️⚖️Risk - Benefit
👇🏽@AmerGastroAssn 1st & 2nd line Rx👇🏽@AGA_CGH

#MNIBDWebinar @DCharabaty
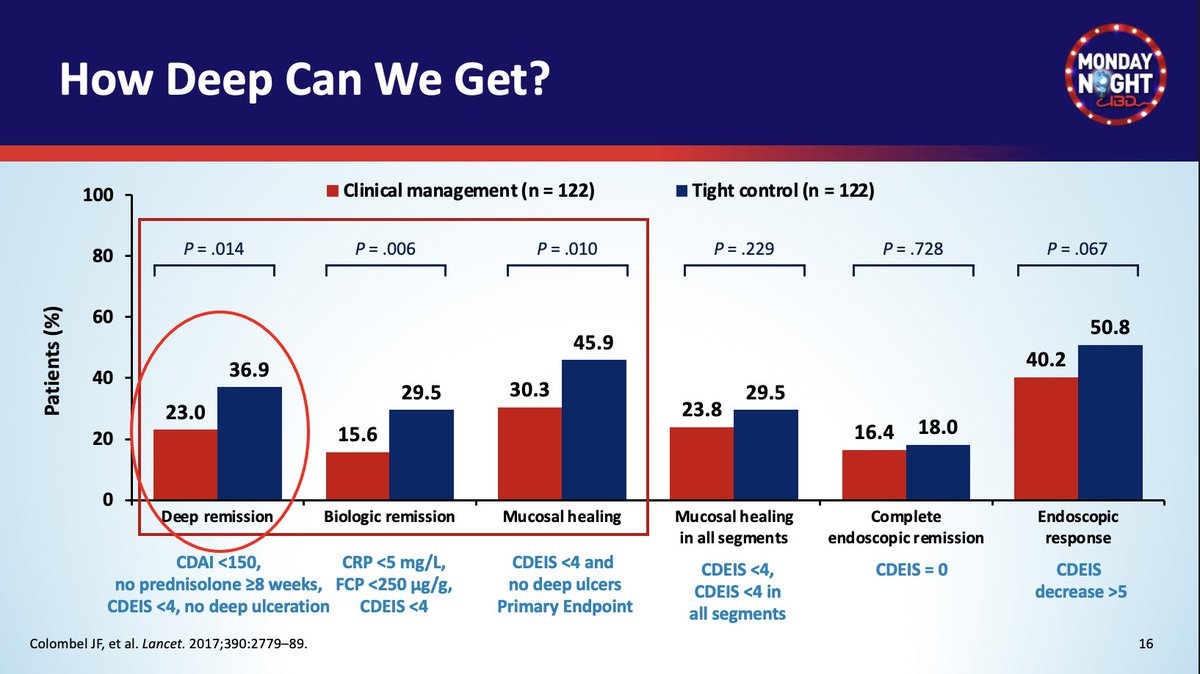
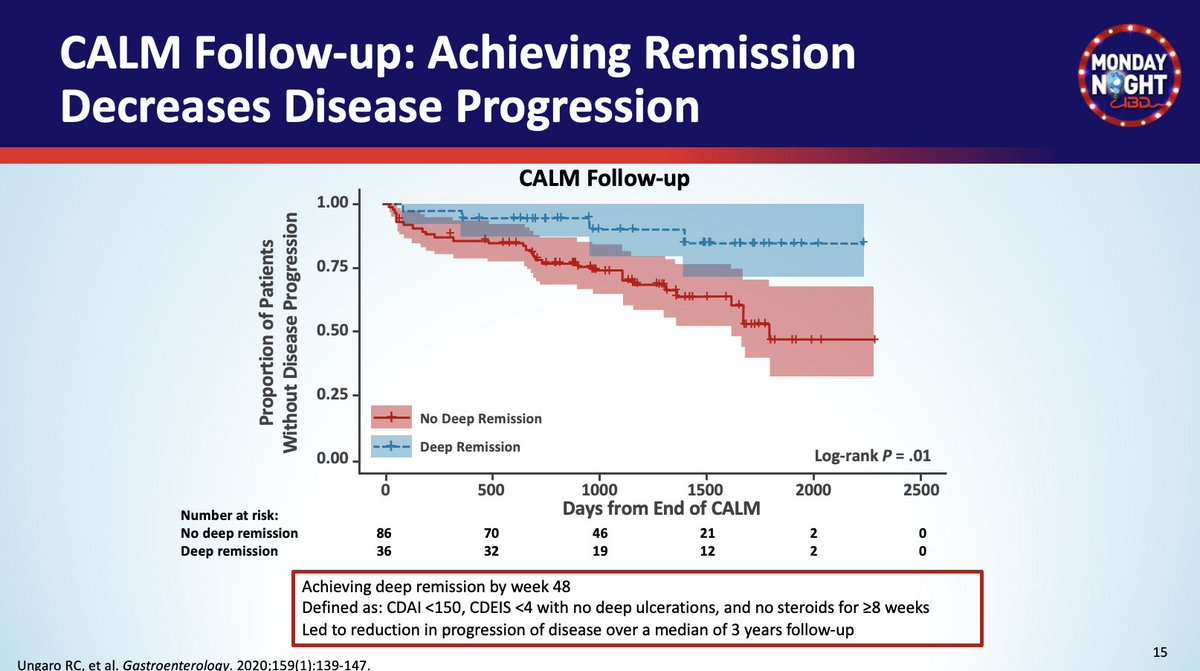
⚖️ Set high🎯but realistic expectation
#CALM 🎯Deep remission on ADAL =
✅ CDAI< 150 off steroids
✅ Mucosal healing: CDEIS< 4, No deep ulcers
✔️Tight control > Clinical management group
✔️But achieved only in 37%
🧘🏽♀️Know when good is good enough
⚖️ Set high🎯but realistic expectation
#CALM 🎯Deep remission on ADAL =
✅ CDAI< 150 off steroids
✅ Mucosal healing: CDEIS< 4, No deep ulcers
✔️Tight control > Clinical management group
✔️But achieved only in 37%
🧘🏽♀️Know when good is good enough
#MNIBDWebinar @EdwardLoftus2
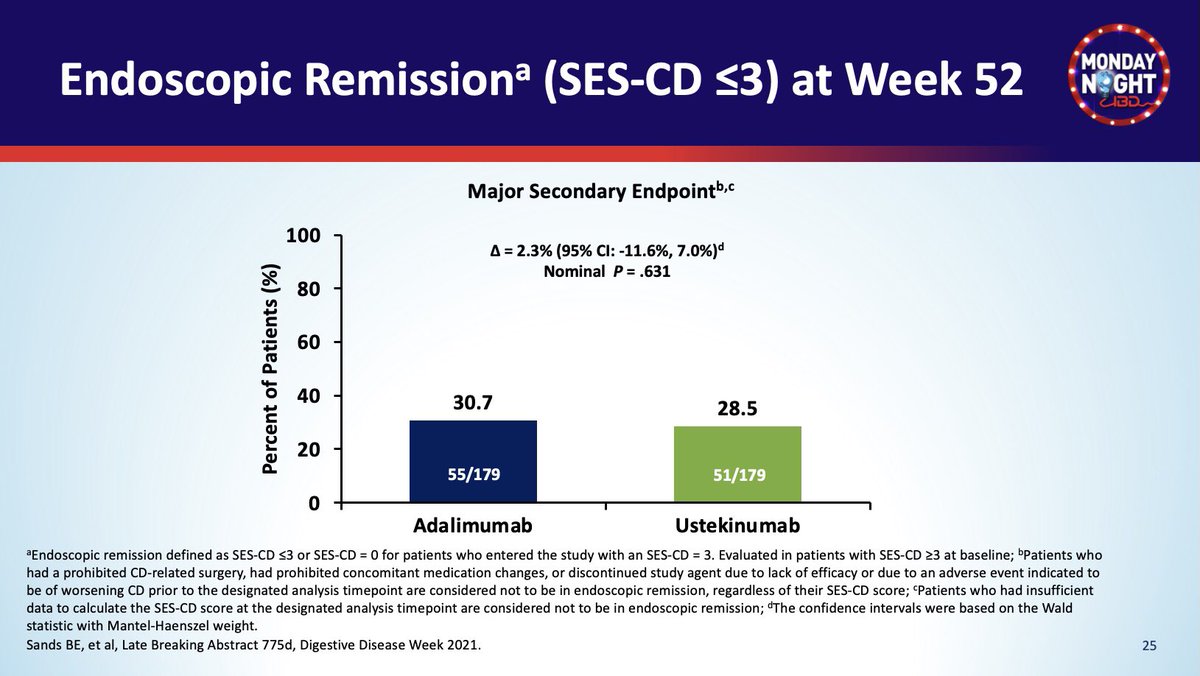
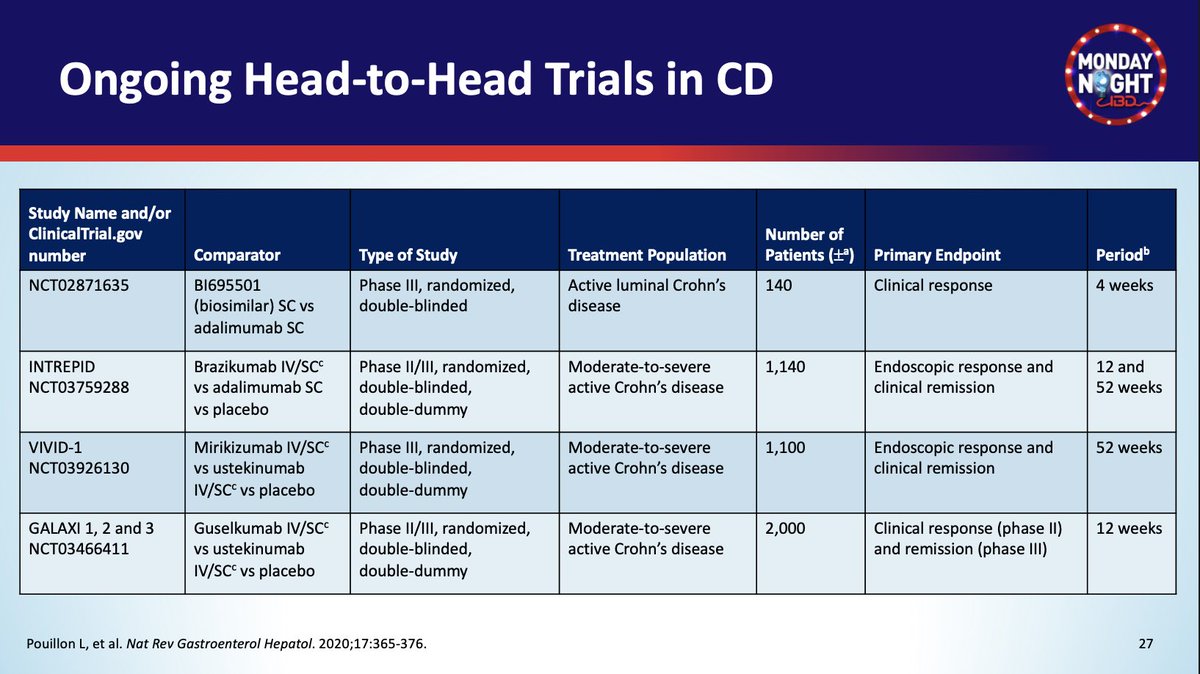
🆕#SEAVUE UST vs ADAL in #Crohns
🔺No difference @ wk52
✅Clinical Remission ~ 60%
✅🔦Endo Remission ~30%
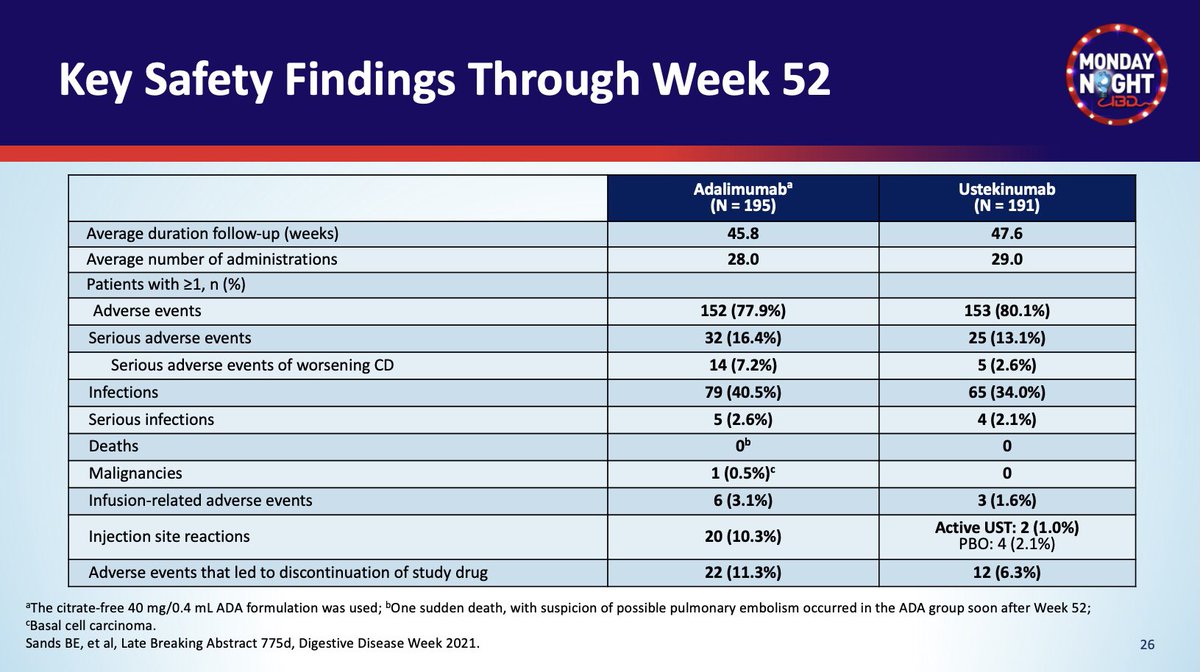
✅Safety profile, except less AE leading to d/c Rx w UST
🔺What are the implications on your practice? @ibddoctor @bruce_sands1
🆕#SEAVUE UST vs ADAL in #Crohns
🔺No difference @ wk52
✅Clinical Remission ~ 60%
✅🔦Endo Remission ~30%
✅Safety profile, except less AE leading to d/c Rx w UST
🔺What are the implications on your practice? @ibddoctor @bruce_sands1
#MNIBDWebinar @EdwardLoftus2
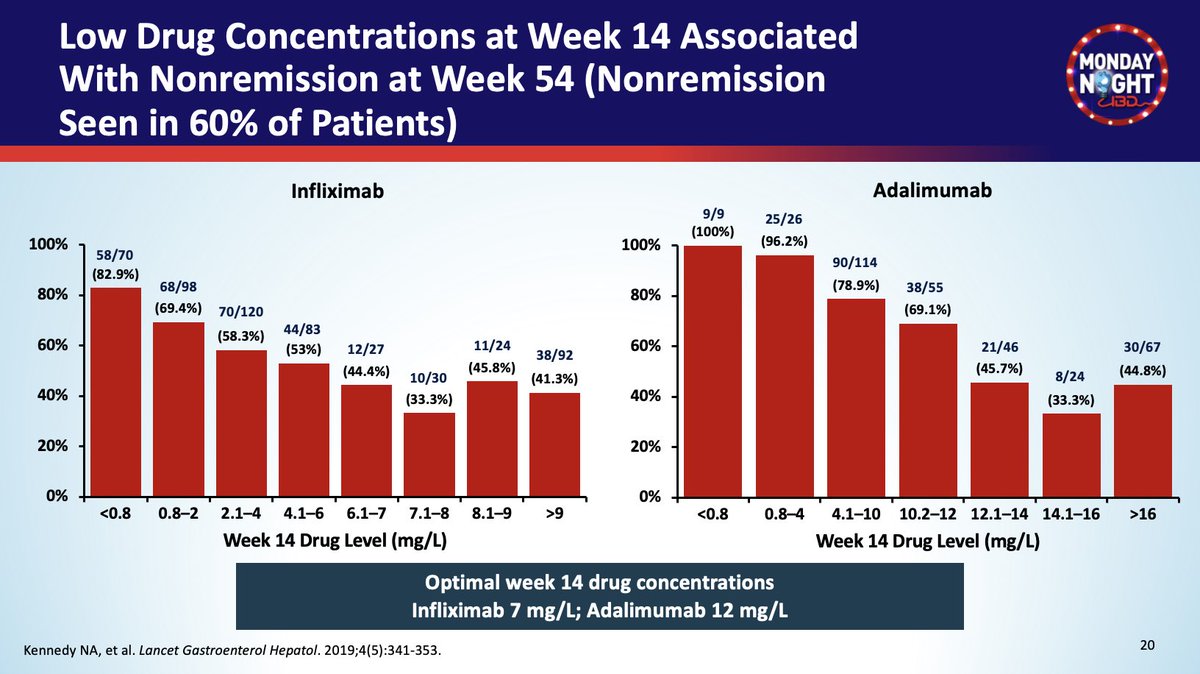
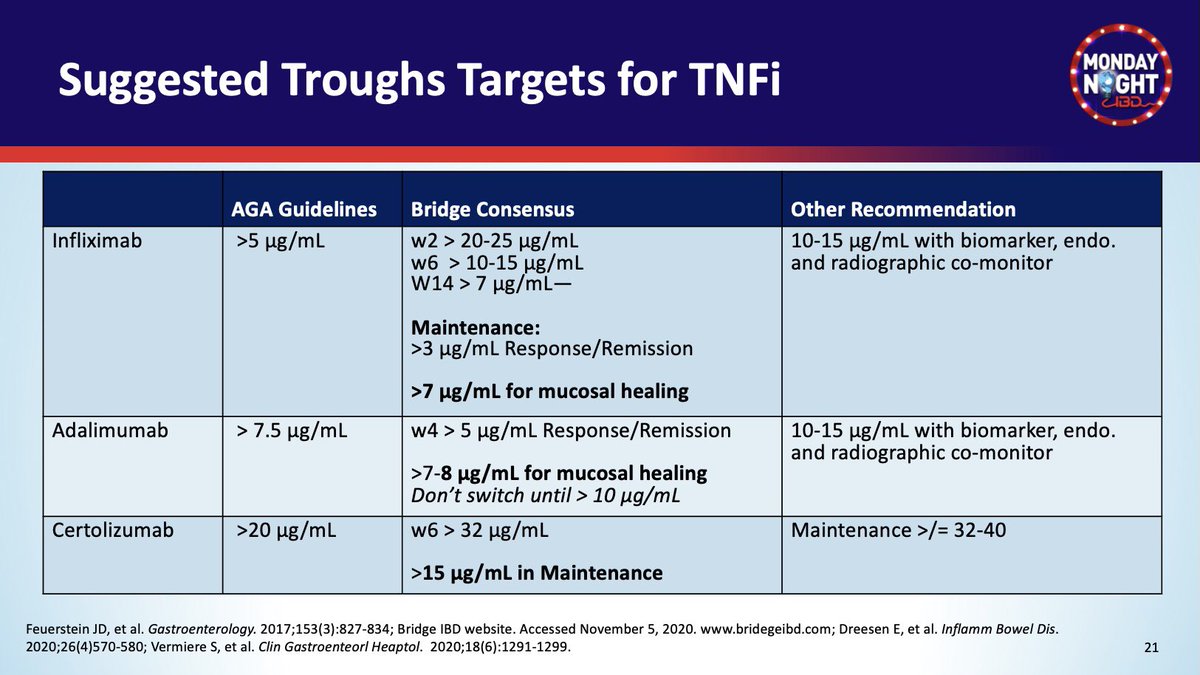
#TDM in #Crohns
🎯Target level of TNFi vary by
✔️Timing: Induction vs maintenance
✔️Rx goals: Clinical remission vs 🔦mucosal healing
✔️@AmerGastroAssn / other consensus
✅Summary table for IFX/ ADAL/ CZP👇🏽
What is your 🎯 in practice?
#TDM in #Crohns
🎯Target level of TNFi vary by
✔️Timing: Induction vs maintenance
✔️Rx goals: Clinical remission vs 🔦mucosal healing
✔️@AmerGastroAssn / other consensus
✅Summary table for IFX/ ADAL/ CZP👇🏽
What is your 🎯 in practice?
#MNIBDWebinar @EdwardLoftus2
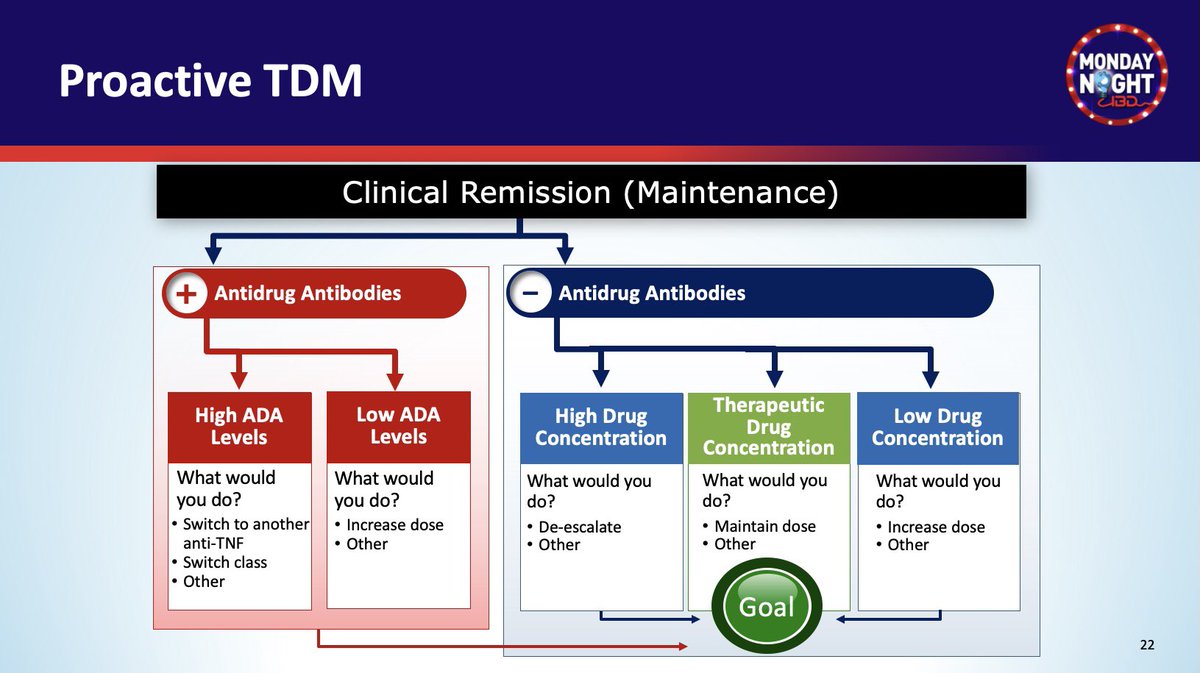
Proactive #TDM in #Crohns
✔️Do you modify Rx based on🧪TNFi & anti-drug antibodies if pt is in remission?
✔️Is any form of close 🔎monitoring (clinically or TDM) followed by Rx adjustment 🎯 effective?
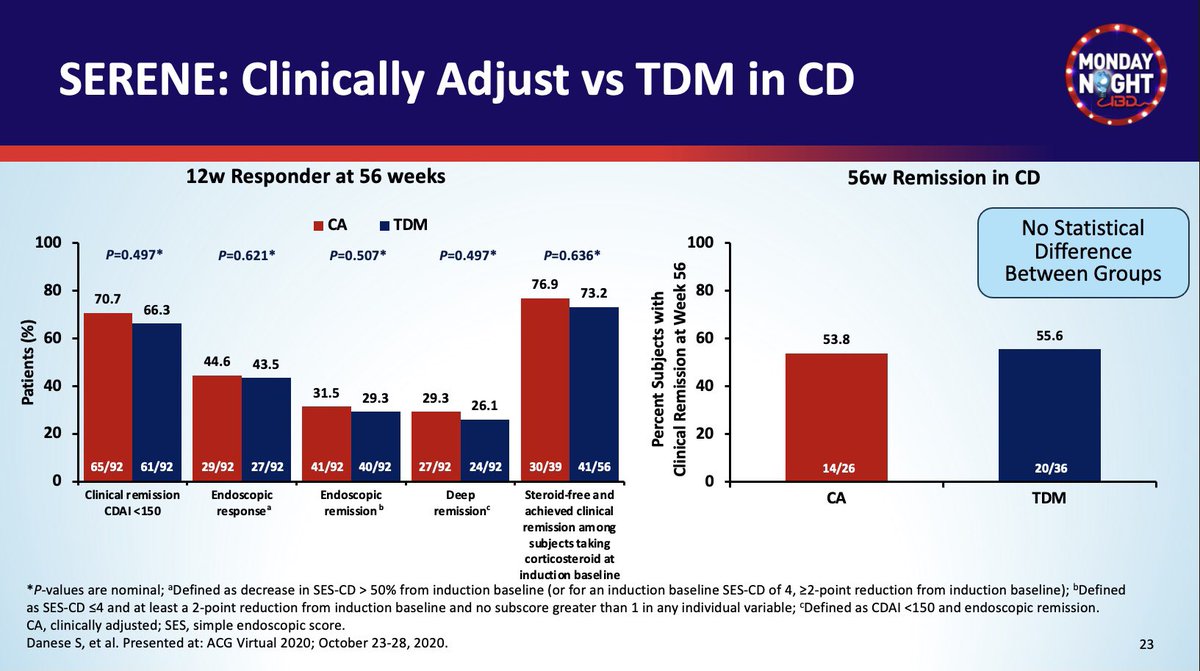
👇🏽It could be #SERENE on ADAL either way
Proactive #TDM in #Crohns
✔️Do you modify Rx based on🧪TNFi & anti-drug antibodies if pt is in remission?
✔️Is any form of close 🔎monitoring (clinically or TDM) followed by Rx adjustment 🎯 effective?
👇🏽It could be #SERENE on ADAL either way
#MNIBDWebinar @EdwardLoftus2
🆕#SEAVUE UST vs ADAL in #Crohns
🔺No difference @ wk52
✅Clinical Remission ~ 60%
✅🔦Endo Remission ~30%
✅Safety profile, except less AE leading to d/c Rx w UST
🔺What are the implications on your practice? @ibddoctor @bruce_sands1
🆕#SEAVUE UST vs ADAL in #Crohns
🔺No difference @ wk52
✅Clinical Remission ~ 60%
✅🔦Endo Remission ~30%
✅Safety profile, except less AE leading to d/c Rx w UST
🔺What are the implications on your practice? @ibddoctor @bruce_sands1
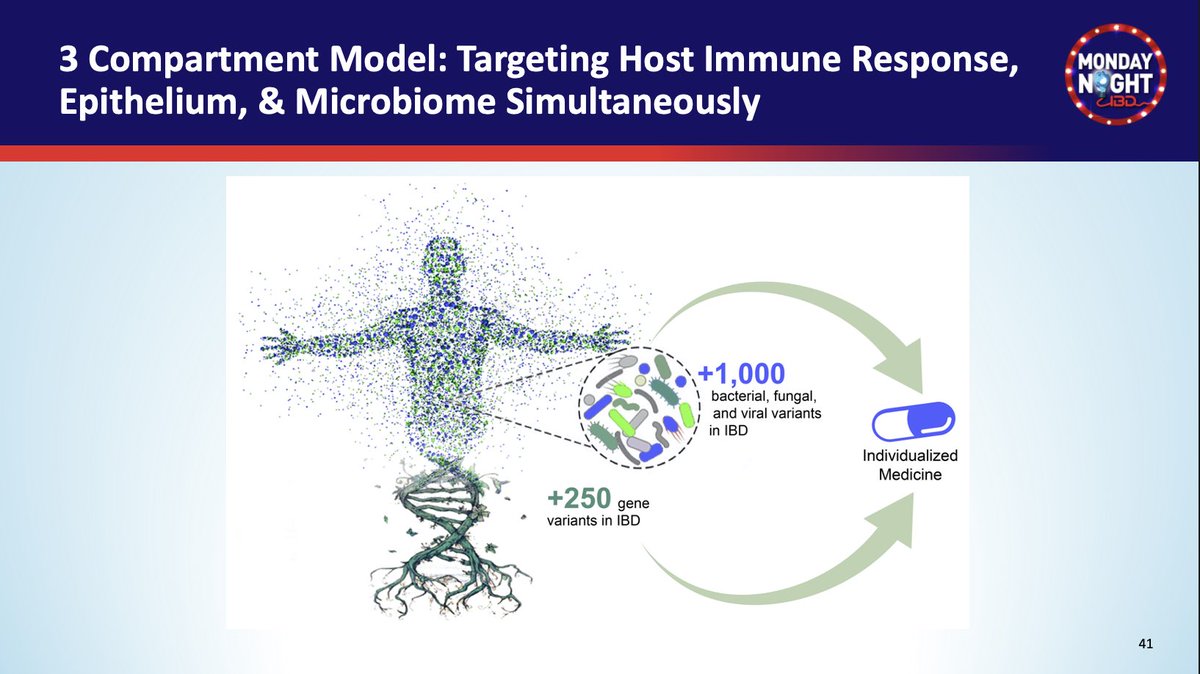
#MNIBDWebinar @ibddocmaria
🔮Future of #IBD care
✅ Personalized care
✔️Biomarkers for dx, prognosis & Rx response
🔺Genetics
🔺Microbiome
🔺Tissue cytokines level
✅Multidimensional approach
🔺Prevention, early dx
🔺Personalized effective Rx
🔺Diet
🔺Lifestyle
🔮Future of #IBD care
✅ Personalized care
✔️Biomarkers for dx, prognosis & Rx response
🔺Genetics
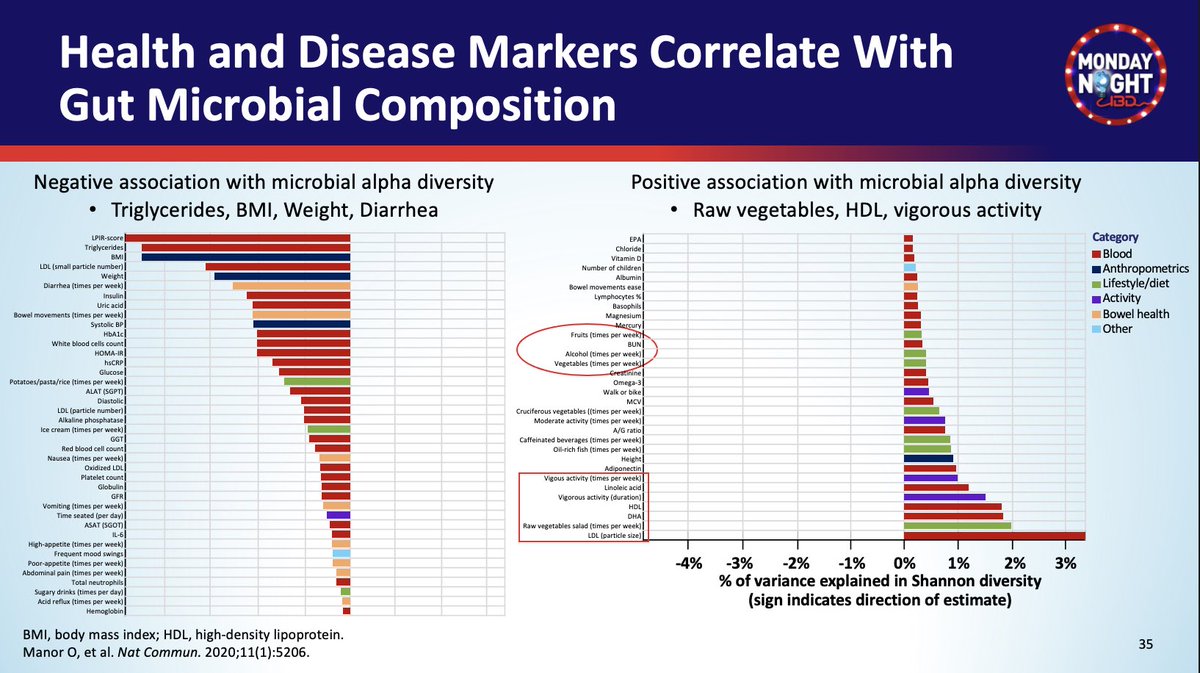
🔺Microbiome
🔺Tissue cytokines level
✅Multidimensional approach
🔺Prevention, early dx
🔺Personalized effective Rx
🔺Diet
🔺Lifestyle

#MNIBDWebinar @ibddocmaria
🔮Personalized medicine in #IBD #Crohns
🧬Genetics factors
✔️HLA-DQA1*05 🔁 anti-TNFi antibodies
✔️NOD2+/+ & 🚬 ▶️ Ileal stricture + Crohns surgery✂️
🔮Personalized medicine in #IBD #Crohns
🧬Genetics factors
✔️HLA-DQA1*05 🔁 anti-TNFi antibodies
✔️NOD2+/+ & 🚬 ▶️ Ileal stricture + Crohns surgery✂️

#MNIBDWebinar @ibddocmaria
🔮Precision medicine #IBD
#Crohns
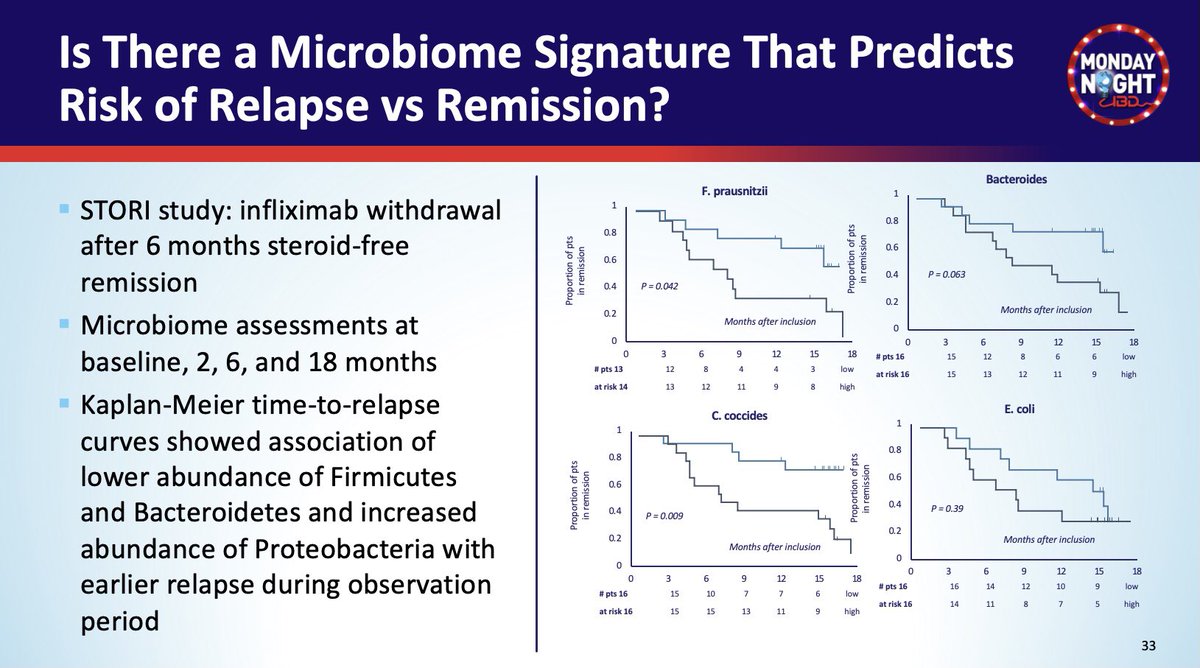
💩Gut #microbiome
✔️💩Function predicts response to anti-Integrin
✔️💩Signature predicts early relapse after stopping IFX #STORI
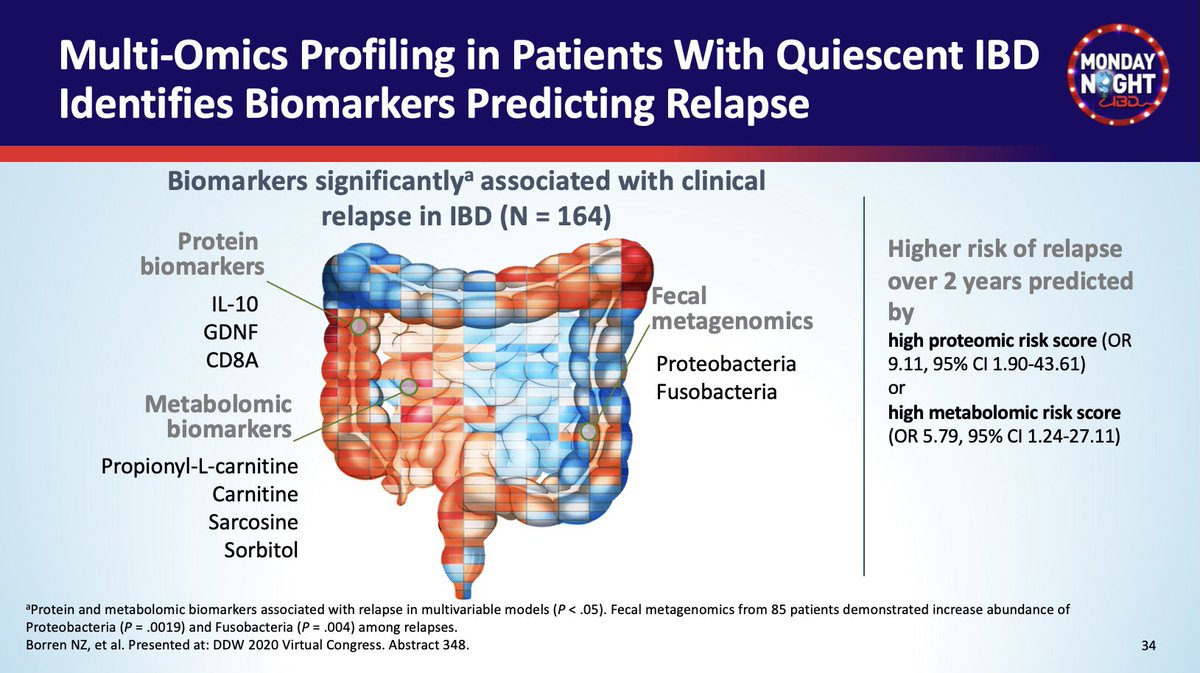
✔️💩Multi-omics Profiling predict relapse in quiescent IBD
🔮Precision medicine #IBD
#Crohns
💩Gut #microbiome
✔️💩Function predicts response to anti-Integrin
✔️💩Signature predicts early relapse after stopping IFX #STORI
✔️💩Multi-omics Profiling predict relapse in quiescent IBD

#MNIBDWebinar @ibddocmaria
🔮Multidimensional approach to #IBD care
🍲#Diet & IBD
🍭⬆️ Fructose
-> Alter microbiome
-> Pro-colitis🔥 effect
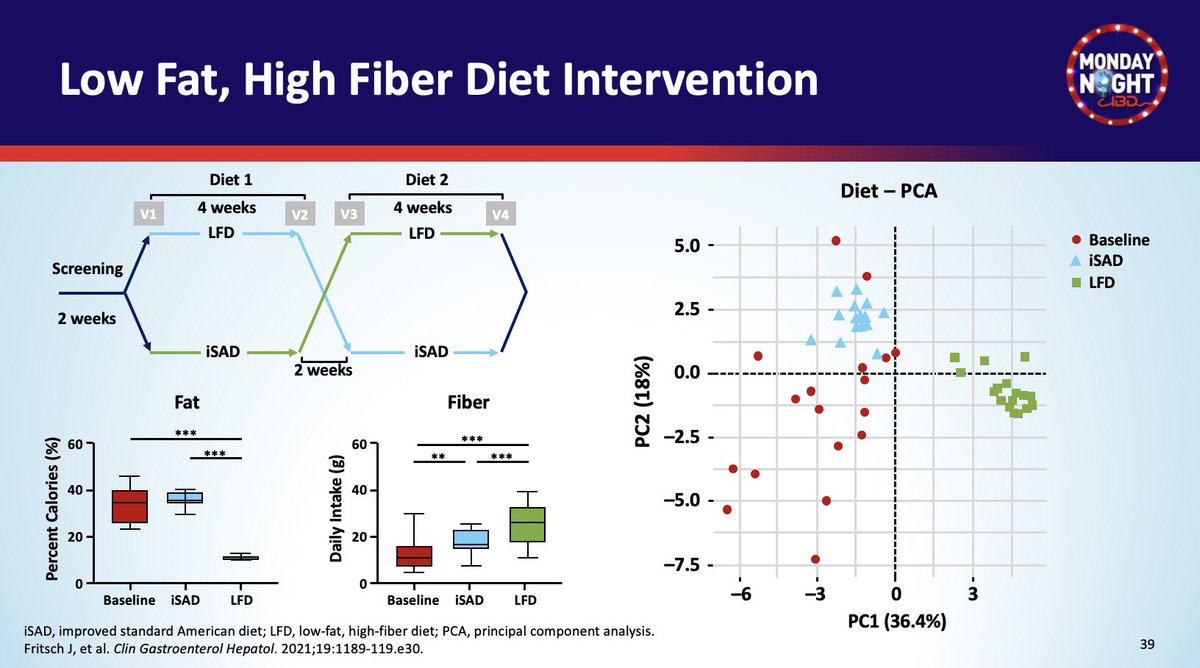
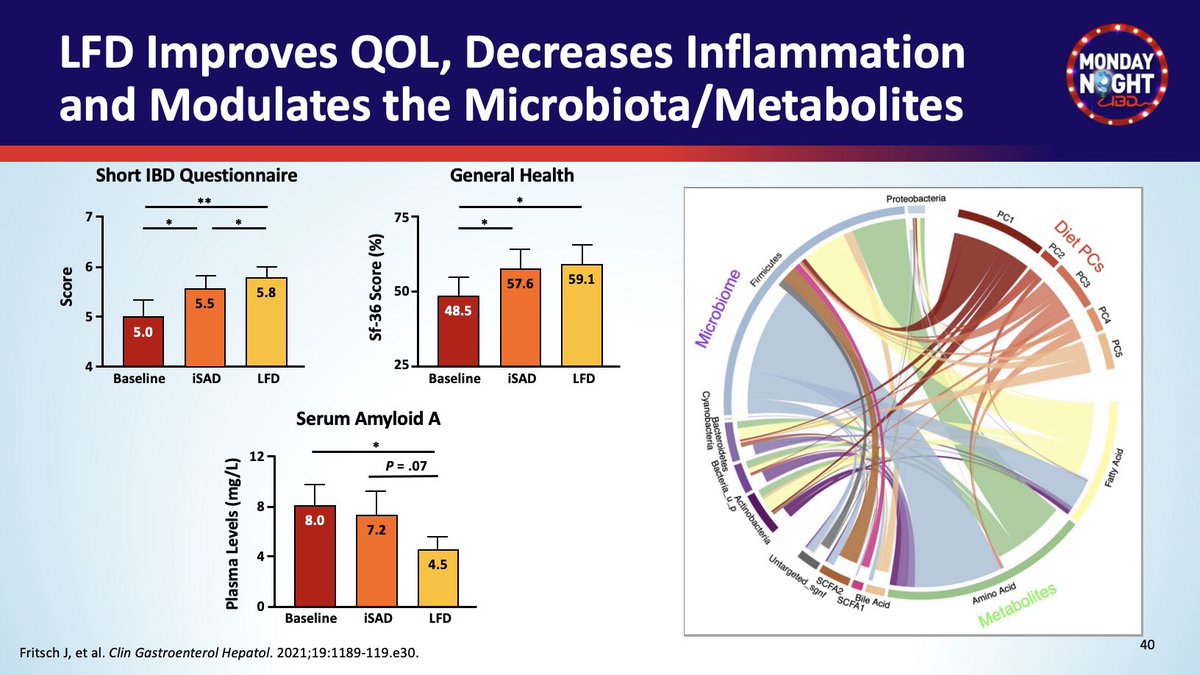
🥗Low Fat & High Fiber diet -> ⬇️ biomarkers of 🔥
-> ⬇️ Dysbiosis
-> ⬆️ QOL
🔮Multidimensional approach to #IBD care
🍲#Diet & IBD
🍭⬆️ Fructose
-> Alter microbiome
-> Pro-colitis🔥 effect
🥗Low Fat & High Fiber diet -> ⬇️ biomarkers of 🔥
-> ⬇️ Dysbiosis
-> ⬆️ QOL
Loading suggestions...