
Today’s Tweetorial is on DVT!
@icmteaching and @ICUltrasonica take you through it.
-5-10% of ICU patients will have a silent one.
-Accounts for 12% of ICU deaths
-It is detectable and preventable!
Use #POCUS to your advantage👍
#FOAMed #FOAMcc #foamus #echofirst #FUSIC
@icmteaching and @ICUltrasonica take you through it.
-5-10% of ICU patients will have a silent one.
-Accounts for 12% of ICU deaths
-It is detectable and preventable!
Use #POCUS to your advantage👍
#FOAMed #FOAMcc #foamus #echofirst #FUSIC

-Clinical examination
*60-96% sensitivity
*20-72% specificity
Wells score 👎validity in the critically ill, as by remit that’s a risk factor itself 🤯
Contrast venography = Standard, but you need to be off the unit for that!
Limited US protocol almost as good as triplex
*60-96% sensitivity
*20-72% specificity
Wells score 👎validity in the critically ill, as by remit that’s a risk factor itself 🤯
Contrast venography = Standard, but you need to be off the unit for that!
Limited US protocol almost as good as triplex

Pop the patient’s leg into the 🐸 leg position.
Scan systematically down the leg, compressing every 2-4cm down the course of the veins. Veins should be squashed shut, reopening on compression release IF patent,
The route shown will pick up most major lower limb DVT’s🤷♂️👍
Scan systematically down the leg, compressing every 2-4cm down the course of the veins. Veins should be squashed shut, reopening on compression release IF patent,
The route shown will pick up most major lower limb DVT’s🤷♂️👍

We describe a ‘Triplex scan’ =
1) 2D ultrasound
2) Colour flow doppler
3) Pulsed wave doppler
Colour discerns artery from vein (pulsatility Vs non)
PWD demonstrates flow pattern, or none🤷♂️😩
My @sono4you_graz talk on DVT is here
fb.watch
1) 2D ultrasound
2) Colour flow doppler
3) Pulsed wave doppler
Colour discerns artery from vein (pulsatility Vs non)
PWD demonstrates flow pattern, or none🤷♂️😩
My @sono4you_graz talk on DVT is here
fb.watch
We describe a ‘Triplex scan’ =
1) 2D ultrasound
2) Colour flow doppler
3) Pulsed wave doppler
Colour discerns artery from vein (pulsatility Vs non)
PWD demonstrates flow pattern, or none🤷♂️😩
My @sono4you_graz talk on DVT is here
fb.watch
1) 2D ultrasound
2) Colour flow doppler
3) Pulsed wave doppler
Colour discerns artery from vein (pulsatility Vs non)
PWD demonstrates flow pattern, or none🤷♂️😩
My @sono4you_graz talk on DVT is here
fb.watch
Let’s look at the venous anatomy of the lower limb.
Here we demonstrate the upper portion of the leg, down to the distal femur. There are a few main veins to focus upon.
👍 to @3D4Medical for the anatomical builds I have made throughout this series.
Here we demonstrate the upper portion of the leg, down to the distal femur. There are a few main veins to focus upon.
👍 to @3D4Medical for the anatomical builds I have made throughout this series.

And now, the portion below the knee.
Some stop scanning above the knee…don’t; scan down, behind and below so as not to miss anything!
Some stop scanning above the knee…don’t; scan down, behind and below so as not to miss anything!

We SHOULD start right up top, where the first large vein is seen!
The IVC - it lies to the right of the aorta, bifurcating alongside its arterial counterpart (iliac veins and iliac arteries).
We don’t often compress here though!!!
Here’s the classic US image we see
The IVC - it lies to the right of the aorta, bifurcating alongside its arterial counterpart (iliac veins and iliac arteries).
We don’t often compress here though!!!
Here’s the classic US image we see

Scan Point 1 - the saphenofemoral junction. Shown here.
And here is one of our classically described US signs! 🐭
You can see how he is formed. People forget this start point…don’t just start at the femoral level, go above🤟
And here is one of our classically described US signs! 🐭
You can see how he is formed. People forget this start point…don’t just start at the femoral level, go above🤟

Scan point 2 - the femoral vein.
People use this for vascath access and it’s easy to see why. Large chunky vein near the artery. Runs down midline + anterior, terminating behind the knee.
Remember from lateral to medial N-A-V-Y:
Nerve
Artery
Vein
Y-fronts (underpants)😂
People use this for vascath access and it’s easy to see why. Large chunky vein near the artery. Runs down midline + anterior, terminating behind the knee.
Remember from lateral to medial N-A-V-Y:
Nerve
Artery
Vein
Y-fronts (underpants)😂

Scan point 3 - the more medial saphenous vein.
This one runs right down the leg, to become the great saphenous vein, terminating above the medial malleolus. Another we sometimes forget to follow down.
This one runs right down the leg, to become the great saphenous vein, terminating above the medial malleolus. Another we sometimes forget to follow down.

Scan point 4 - the popliteal vein.
The femoral terminates behind the knee, becoming the pop. vein.
It is often neglected; therefore silent DVT’s are missed here. Always scan behind the knee - push from the back, supporting the knee from the front.
This one trifurcates.
The femoral terminates behind the knee, becoming the pop. vein.
It is often neglected; therefore silent DVT’s are missed here. Always scan behind the knee - push from the back, supporting the knee from the front.
This one trifurcates.

Here’s the whole lot for you. The 4 points below the IVC, if scanned clearly, give you a fighting chance to rule in / out a lower limb DVT with some certainty.
Sensitivity 90-100%
Specificity 75-99% 👍🍺
Sensitivity 90-100%
Specificity 75-99% 👍🍺

I wanted to demonstrate ‘Augmentation’
This is where an assistant squeezes the leg at points BELOW the point being scanned. IF the vein is patent, a ‘whoosh’ of colour or PWD trace/sound can be observed as blood freely flows back towards the probe. Seen here👇
This is where an assistant squeezes the leg at points BELOW the point being scanned. IF the vein is patent, a ‘whoosh’ of colour or PWD trace/sound can be observed as blood freely flows back towards the probe. Seen here👇

Here is a femoral DVT. ☠️
We see a mere blinking of colour on the outside of the vein, around the obstructing clot. The artery can be seen clearly.
We see a mere blinking of colour on the outside of the vein, around the obstructing clot. The artery can be seen clearly.

Another view of a common femoral vein DVT. It is subtle, but there is a more echogenic, textured mass within the vein, seen a little more clearly with compression.
Don’t over compress a DVT, or repeatedly do so when you are excited you’ve found one!!! 🤦♂️
Don’t over compress a DVT, or repeatedly do so when you are excited you’ve found one!!! 🤦♂️

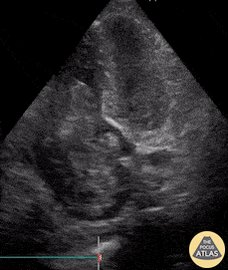
Here’s a popliteal DVT.
The clot becomes far more obvious on compression. The artery is again the star of the show here!
By the way, veins should compress to obliteration point..if not, why not?!
The clot becomes far more obvious on compression. The artery is again the star of the show here!
By the way, veins should compress to obliteration point..if not, why not?!

Now; mimics!
Here is a Baker’s Cyst. Hypoechoic throughout and compressible too. NOT a DVT!
Little to see on colour flow or PWD.
Here is a Baker’s Cyst. Hypoechoic throughout and compressible too. NOT a DVT!
Little to see on colour flow or PWD.

And a lymph node. Looks very similar in echogenicity to a DVT BUT..put power or colour doppler on - swirling starry colours seen as the lymph runs a swirl. Also, normally more superficial and NO flow on PWD!

So:
- It is highly sensitive and specific
- Start at the SFJ and work down, compressing @2cm intervals
- Pop on colour and pulsed wave to make it a triplex series.
You could prevent a PE or worse, death!
- It is highly sensitive and specific
- Start at the SFJ and work down, compressing @2cm intervals
- Pop on colour and pulsed wave to make it a triplex series.
You could prevent a PE or worse, death!

No one wants to see this, when it COULD have been prevented with a basic scan series!
Happy scanning to you all!
@sonophysio @SimonOrlob @iceman_ex @Manoj_Wickram @dr_rajgupta @load_dependent @khaycock2 @POCUSAcademy @IMPOCUSFocus @POCUSClub @kyliebaker888 @GEHealthcare
Happy scanning to you all!
@sonophysio @SimonOrlob @iceman_ex @Manoj_Wickram @dr_rajgupta @load_dependent @khaycock2 @POCUSAcademy @IMPOCUSFocus @POCUSClub @kyliebaker888 @GEHealthcare
Loading suggestions...