

Interesting ICU case!
74 female recently discharged 1 week ago following stroke and Afib, now presenting to the ED bradycardic HR 34, hypotensive 70/42 and obtunded hence intubated, Temp 33C
74 female recently discharged 1 week ago following stroke and Afib, now presenting to the ED bradycardic HR 34, hypotensive 70/42 and obtunded hence intubated, Temp 33C

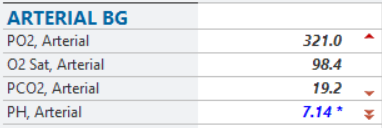
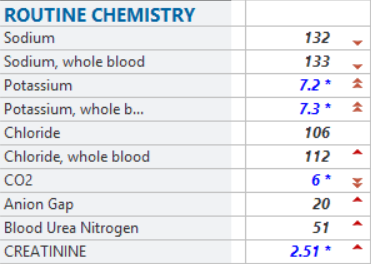
Initial blood gas and BMP following intubation
Significant metabolic acidosis with inadequate respiratory compensation
AKI (no history of renal disease) with significant hyperkalemia
Significant metabolic acidosis with inadequate respiratory compensation
AKI (no history of renal disease) with significant hyperkalemia
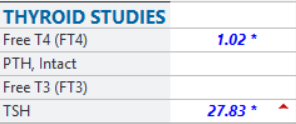
Due to hypothermia (covered with antibiotics) additional work up was performed
-Highly elevated TSH and low Free T4
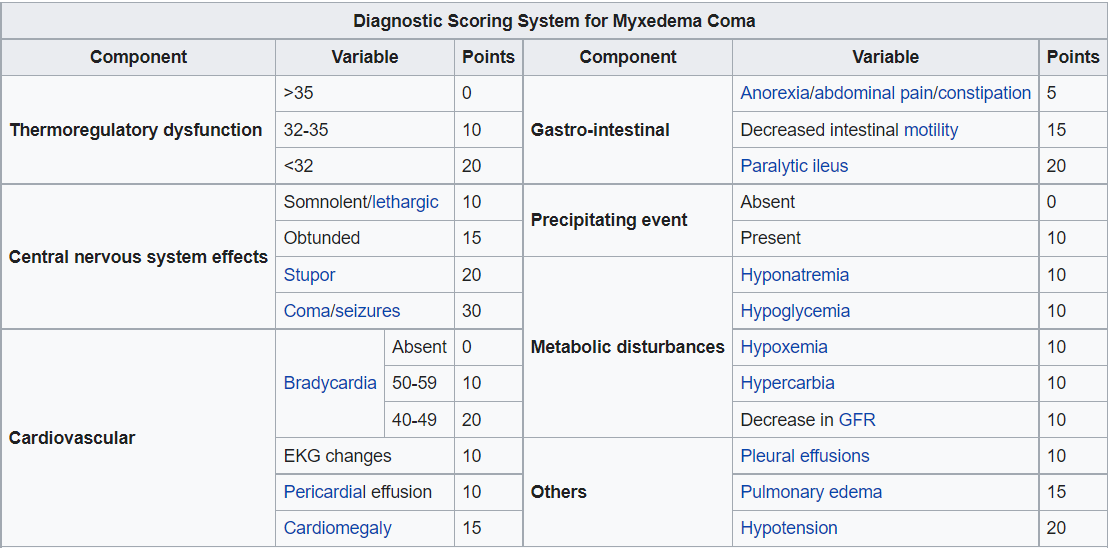
-Myxedema coma score of 100!
(Score obtained from Popoveniuc G, Wartofsky L (2014). "A diagnostic scoring system for myxedema coma". Endocr Pract. 20 (8): 808–17
-Highly elevated TSH and low Free T4
-Myxedema coma score of 100!
(Score obtained from Popoveniuc G, Wartofsky L (2014). "A diagnostic scoring system for myxedema coma". Endocr Pract. 20 (8): 808–17
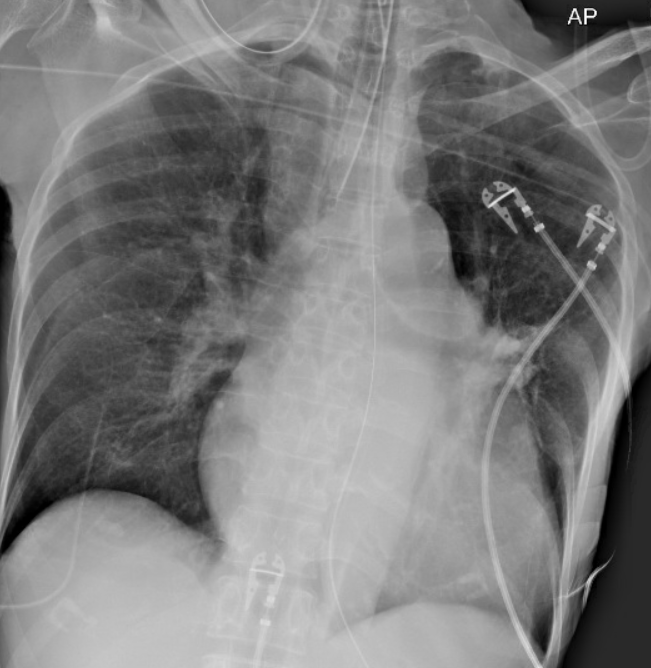
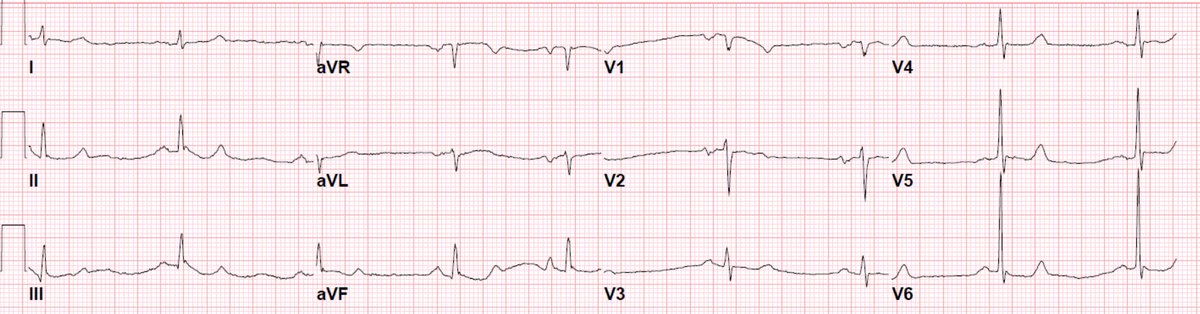
Chest Xray with EKG before and after gradual rewarming:
-No pleural effusions, suggestion of hilar vessel enlargement
-Osborn waves with odd sagging of ST segments
-No pleural effusions, suggestion of hilar vessel enlargement
-Osborn waves with odd sagging of ST segments
At this point what are you thinking?
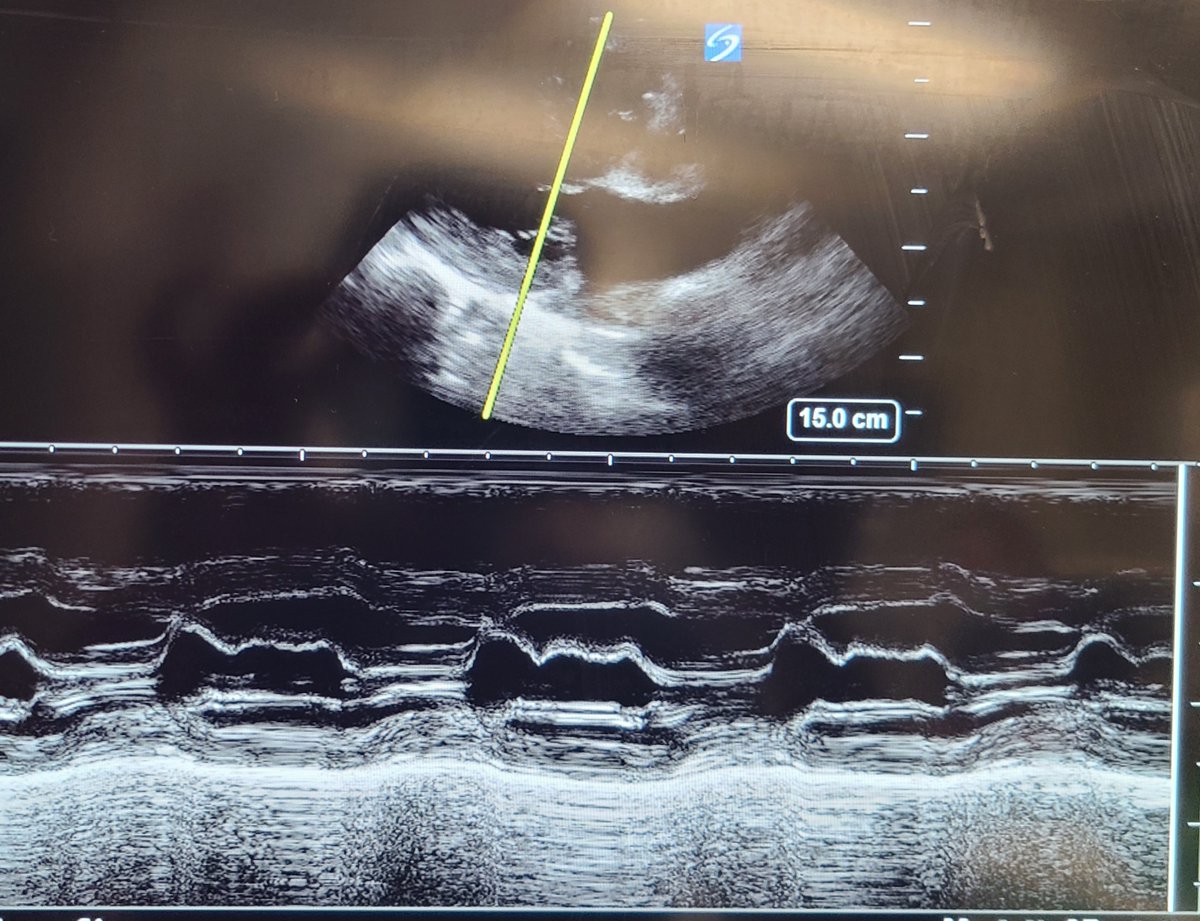
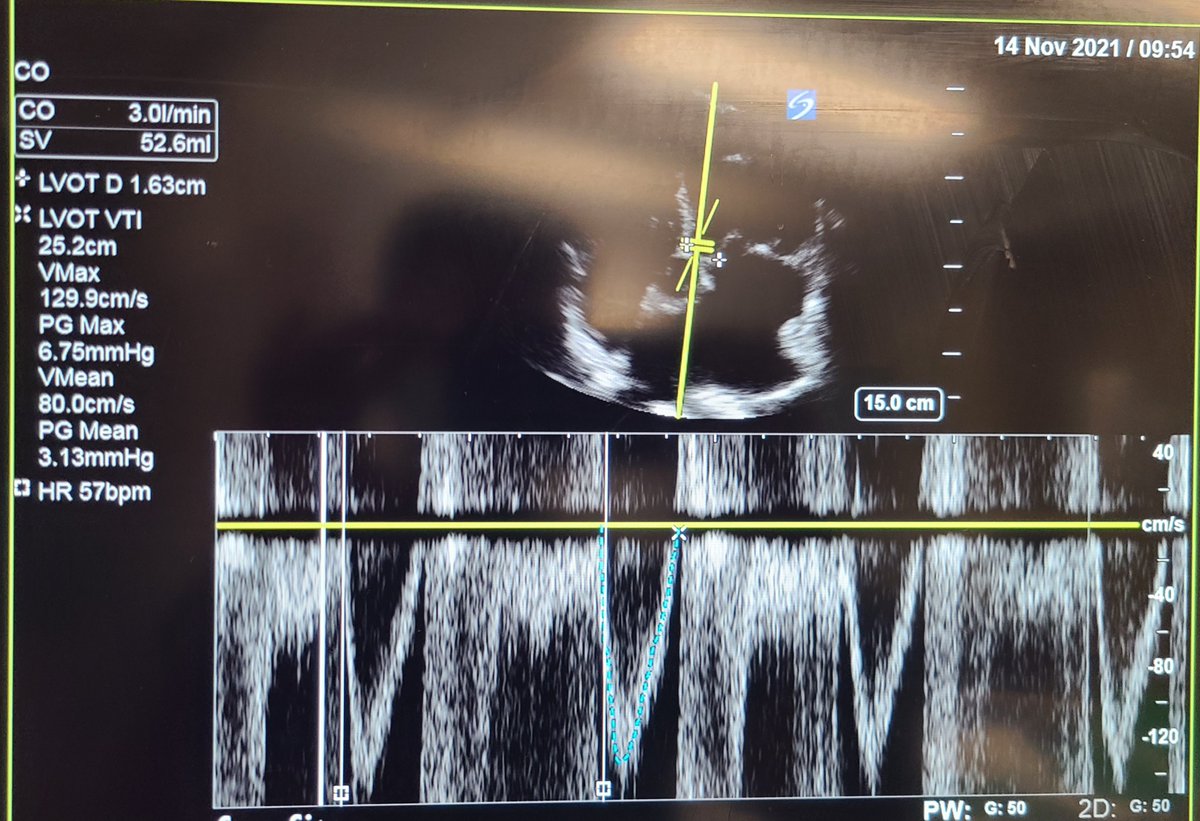
Bedside echo performed in MICU:
Parasternal long axis
Parasternal long axis

Apical 4 chamber:

EPSS and LVOT VTI
Echocardiogram demonstrates preserved EF without evidence of RV pressure overload, no overt pericardial or pleural effusion but confirms low cardiac output driven by bradycardia (CO calculated 3L/min)
Echocardiogram demonstrates preserved EF without evidence of RV pressure overload, no overt pericardial or pleural effusion but confirms low cardiac output driven by bradycardia (CO calculated 3L/min)
Images were obtained following administration of IV levothyroxine and further history taken revealed patient was recently placed on digoxin!
Hence was placed on dopamine infusion at 5mcg/kg/min
-Following administration of +ve chronotropic agent pt's blood pressure normalized
Hence was placed on dopamine infusion at 5mcg/kg/min
-Following administration of +ve chronotropic agent pt's blood pressure normalized
-Noted with rapid correction of metabolic acidosis (largely driven by lactic acidosis) as cardiac output improved
-Pt began to produce >0.5cc/kg urine output and hence dialysis was deferred
-Pt began to produce >0.5cc/kg urine output and hence dialysis was deferred
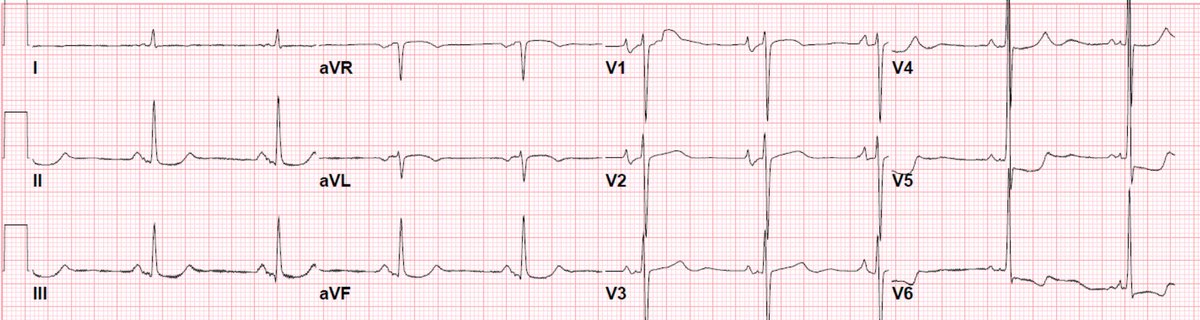
Looking back at the 12 lead EKGs and demonstrated once more on telemetry here, we note the sagging of the ST segments once more
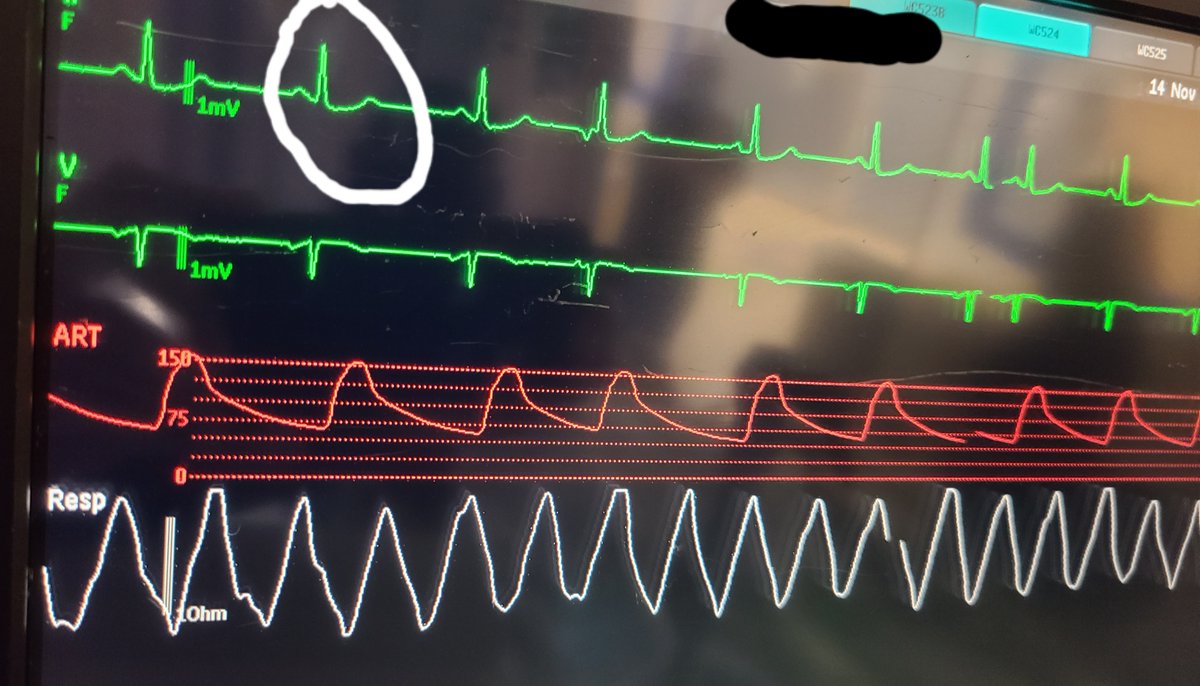
Digoxin levels returned within normal limits but remember digoxin has a narrow therapeutic index! normal levels do not rule out digoxin toxicity
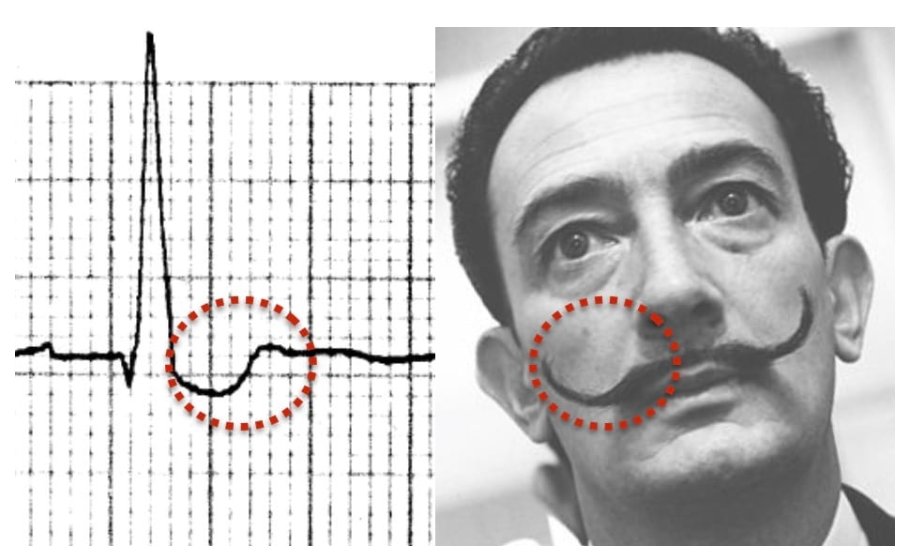
-EKG concerning for digoxin effect (images obtained from litfl.com)
-EKG concerning for digoxin effect (images obtained from litfl.com)
Pt's family reported low PO intake recently and maelstrom of AKI could have precipitated medication toxicity here
-Digoxin immune Fab therapy not pursued as acidosis and hemodynamics normalized
-Digoxin immune Fab therapy not pursued as acidosis and hemodynamics normalized
Interesting points:
-Hyperkalemia here likely precipitated by digoxin as cardiac glycosides inhibit intracellular shifting of potassium
-Increased serum digoxin levels can be noted in coexisting hypothyroidism!
-Hyperkalemia here likely precipitated by digoxin as cardiac glycosides inhibit intracellular shifting of potassium
-Increased serum digoxin levels can be noted in coexisting hypothyroidism!
Learning points:
-Broad differential for bradycardia
-Rapid bedside diagnostics can allow for choice of optimal vasopressor or inotropic/chronotropic agent
-Complex interplay in thyroid disease and digoxin serum levels
-Interesting EKG findings associated with digoxin toxicity
-Broad differential for bradycardia
-Rapid bedside diagnostics can allow for choice of optimal vasopressor or inotropic/chronotropic agent
-Complex interplay in thyroid disease and digoxin serum levels
-Interesting EKG findings associated with digoxin toxicity
Loading suggestions...