

🧵
A brief 🧵 about the role of A-Fib in modifying outcomes after stroke, IV tPA complications, and thrombectomy, and new data about how bridging may increase risk for these patients, from @EmoryNeurosurg @EmoryNeuroCrit @EmoryNeurology
1/
jnis.bmj.com
A brief 🧵 about the role of A-Fib in modifying outcomes after stroke, IV tPA complications, and thrombectomy, and new data about how bridging may increase risk for these patients, from @EmoryNeurosurg @EmoryNeuroCrit @EmoryNeurology
1/
jnis.bmj.com
In the bad old days before any reperfusion therapy, AF stroke was associated with:
↑ infarct size
↑rates of hemorrhagic conversion
Worse outcomes
Cause?
-?larger emboli
-No ischemic pre-conditioning
-What we now think of as fast progressing patients.
↑ infarct size
↑rates of hemorrhagic conversion
Worse outcomes
Cause?
-?larger emboli
-No ischemic pre-conditioning
-What we now think of as fast progressing patients.
In the thrombolysis era, AF patients still at ↑risk of hemorrhagic conversion and worse outcomes after tPA, likely because of large infarcts that were lysed in a population enriched for fast progressors.
PMID: 22084129
PMID: 22084129
So that begs the question:
Is there an AF penalty for stroke in the endovascular era? Do AF patients still have more complications and worse outcomes with mechanical thrombectomy, or is MT somehow different?
Is there an AF penalty for stroke in the endovascular era? Do AF patients still have more complications and worse outcomes with mechanical thrombectomy, or is MT somehow different?
Nope, AF patients respond differently to MT than IVT.
After MT, there is no difference in either outcomes or hemorrhagic complications with respect to AF status.
Interestingly, anecdote about AF clots held true, big AF clots come out faster too!
jnis.bmj.com
After MT, there is no difference in either outcomes or hemorrhagic complications with respect to AF status.
Interestingly, anecdote about AF clots held true, big AF clots come out faster too!
jnis.bmj.com
So based on old and recent data, AF patients have:
-Higher risk for bleed and bad outcomes
-Higher risk for IVT complications
-But do better with MT with more first pass reperfusion and overall faster thrombectomy times
-Higher risk for bleed and bad outcomes
-Higher risk for IVT complications
-But do better with MT with more first pass reperfusion and overall faster thrombectomy times

So...what about IVT + MT?
While the debate rages about bridging therapy, we really haven’t talked about patient selection in trying to identify high risk groups.
So let’s talk about AF and bridging therapy.
While the debate rages about bridging therapy, we really haven’t talked about patient selection in trying to identify high risk groups.
So let’s talk about AF and bridging therapy.

Working with @MUSC_STAR, @AliAlawiehmdphd,@BrianHoward_MD, @alex_spiotta, @JAGrossbergMD, we reviewed >6000 MT patients to ask whether AF modified the effect of bridging therapy, now out in JNIS.
jnis.bmj.com
jnis.bmj.com
Consistent with many recent RCT observations (in unselected patients), non-AF patients exposed to bridging therapy did not have increased hemorrhagic complications. They also had improved outcomes at 90days post stroke.
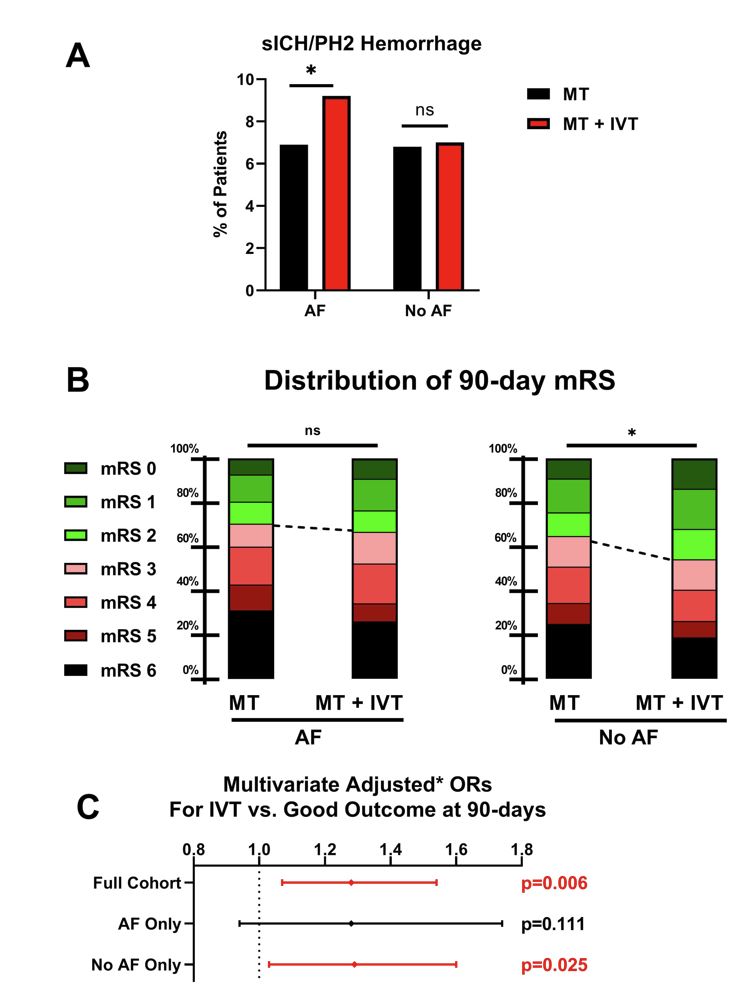
AF patients were another story.
Using multivariable and propensity matched analyses, AF patients who underwent IVT+MT (as compared to MT) had:
-More hemorrhagic complications
-No clinical benefit at 90d
Using multivariable and propensity matched analyses, AF patients who underwent IVT+MT (as compared to MT) had:
-More hemorrhagic complications
-No clinical benefit at 90d

Why?
Not sure, but likely enriching for fast progressors (no preconditioning with AF) and thus more infarcted territory prone to bleed.
2 corroborating pieces of evidence to support this idea.
1) A similar finding has has been reported in ICA-T clots
jnis.bmj.com
Not sure, but likely enriching for fast progressors (no preconditioning with AF) and thus more infarcted territory prone to bleed.
2 corroborating pieces of evidence to support this idea.
1) A similar finding has has been reported in ICA-T clots
jnis.bmj.com
2) Interestingly, SHRINE meta-analysis of DEVT and SKIP RCTs reported similarly increased ICH (and inc mortality at 90d) for bridging therapy in AF patients (and ICA T occlusions). Manuscript pending.
professional.heart.org
professional.heart.org
⚠️Lack of AC data is a key limitation in our dataset.
But think about who gets IVT: The AF patient on vs. not on AC? Clearly, the one not on AC.
So, AF patients getting IVT, those LEAST likely to be on AC, are those who are bleeding most in the @musc_star experience.
But think about who gets IVT: The AF patient on vs. not on AC? Clearly, the one not on AC.
So, AF patients getting IVT, those LEAST likely to be on AC, are those who are bleeding most in the @musc_star experience.
We’re working to externally validate these observations with collaborators, but perhaps we need to reframe the bridging therapy debate.
It’s not bridging good or bad, but specific patients at risk for benefit or harm. Maybe consider fast progressors, bigger strokes, etc
It’s not bridging good or bad, but specific patients at risk for benefit or harm. Maybe consider fast progressors, bigger strokes, etc
The work continues to externally validate our findings and identify patients at risk, but this couldn’t have been done without key @musc_star partners @PascalJabbourMD, @Starkeneurosurg, @Ansaar_Rai, @rdeleacymd, @PeterKa80460001, @AdamArthurMD, @JMoccoMD, @rocrossa, @wchrisfox.
Loading suggestions...