
Can Cerebellum be affected in seizures??
Can cerebellar perfusion predict outcome of cerebral hemispheric stroke??
Find out more below !!
Can cerebellar perfusion predict outcome of cerebral hemispheric stroke??
Find out more below !!
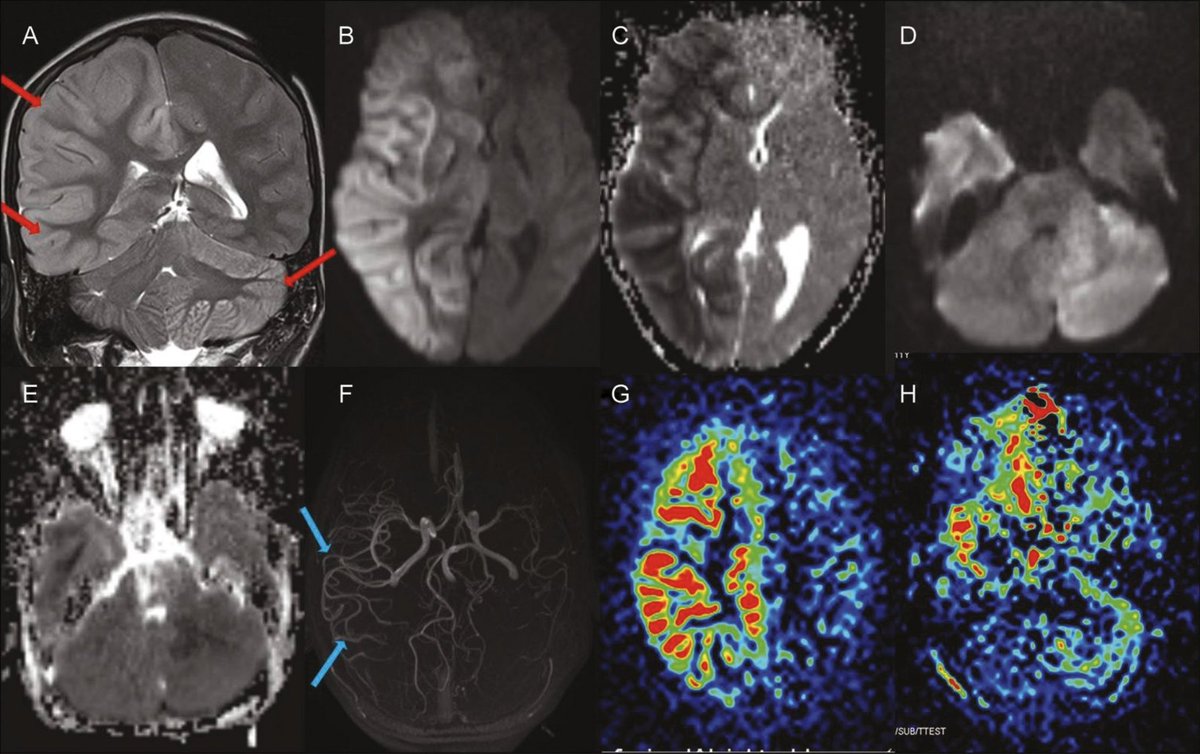
A patient🤕h/o refractory Epilepsy is admitted with status epileptics. Semiology:Rt sided focal onset with 2ndary generalization. Progresses to refractory status epilepticus & burst suppression is achieved. CSF unremarkable except protein 90, 4 nucl cells. So got MRI Brain.

DWI ⬆️ and FLAIR ⬇️

Shows DWI and FLAIR hyper intensity in the left hemisphere and right cerebellum..
Have a look again if missed the first time..
What’s your thought about origin of the patient’s seizures based on this MRI brain above?
Have a look again if missed the first time..
What’s your thought about origin of the patient’s seizures based on this MRI brain above?
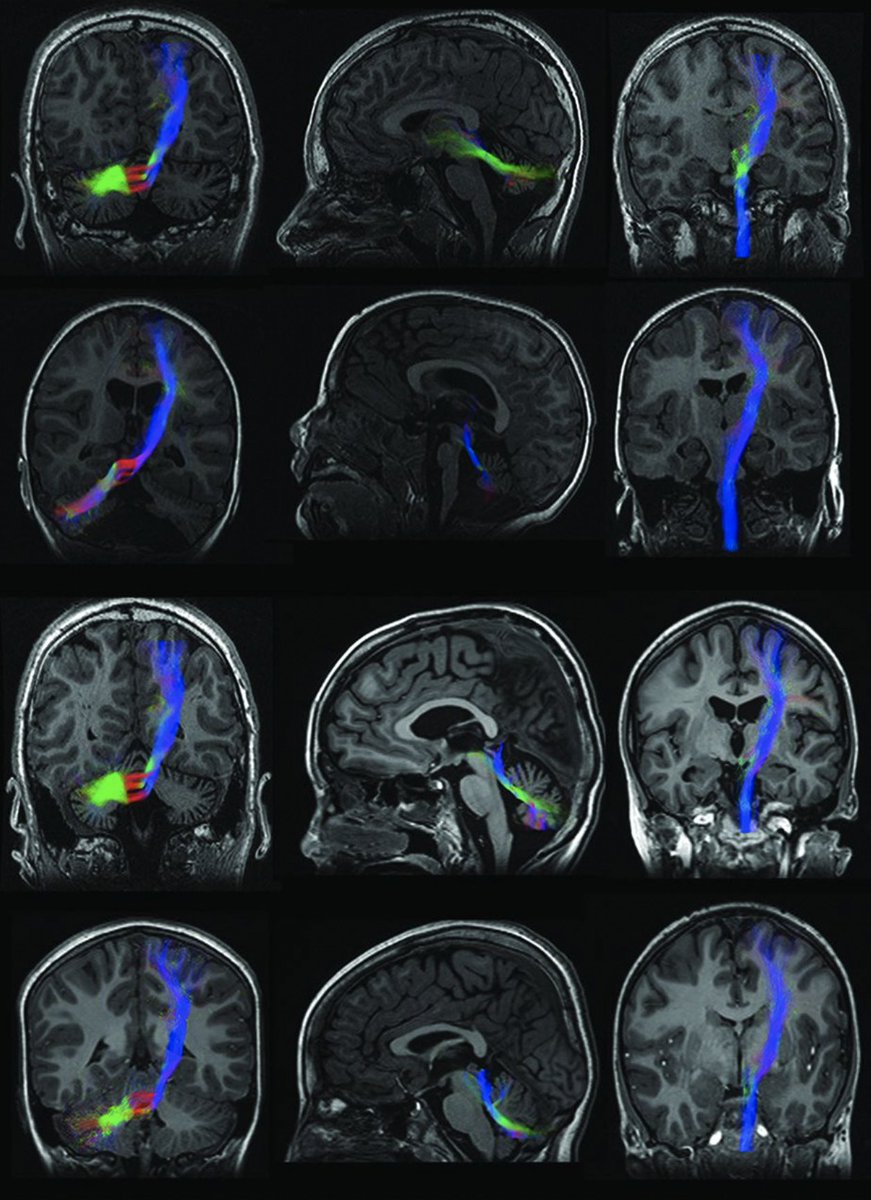
If you correctly answered first question, congrats! Here’s your second chance if you didn’t. If we divide the images BELOW⬇️ in 3 columns, column 1, 2 and 3 from left to right, which column you think will provide the answer of the above question?
Column 1, 2 and 3.
Image source 26659337
MR tractography
Image source 26659337
MR tractography
Term “diaschisis” was used by Von-Monakov in 1914 in his book. He noticed hypoplasia of the contralateral cerebellar hemisphere following experimental cortical ablation in 1885.
This amazing phenomenon is called Crossed Cerebellar Diaschisis (CCD). In neurology, diaschisis refers to reduction of function of a part of the brain following the interruption of afferent pathway at a remote site.
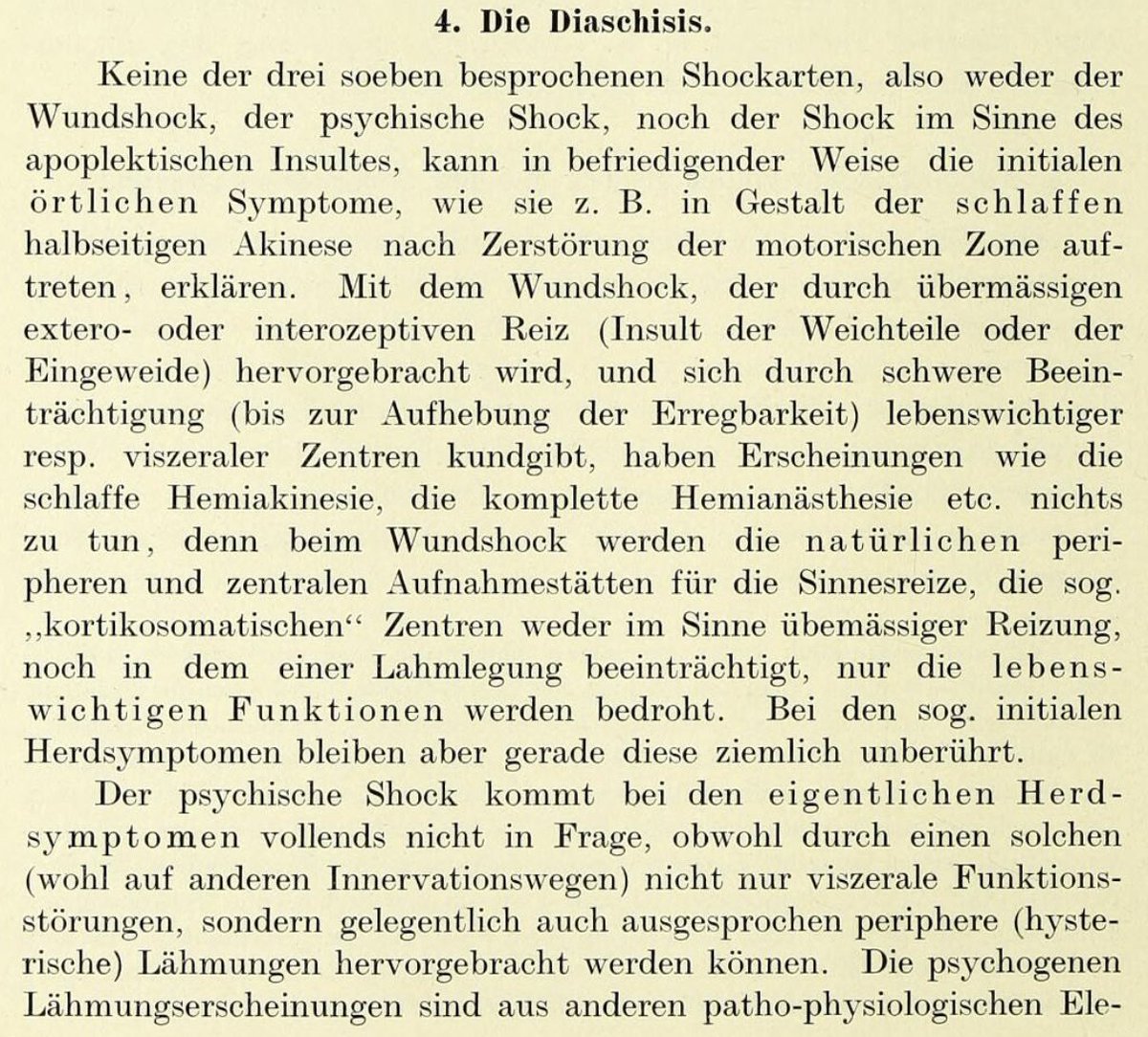
Here’s the book he wrote in 1914 mentioning about Diaschisis.
Here’s the book he wrote in 1914 mentioning about Diaschisis.
So why does this happen?
-Ischemic/hemorrhagic stroke
-Epilepsy/Focal status
-Tumors/Diffuse gliomas-32737798
-Alzheimer’s disease-33622918
-CJD-30308445
-NMDA encephalitis-32061394/Rasmussen encephalitis-20473513
-Sturge-Weber-2288389
-Familial hemiplegic migraine(FHM)-9385760
-Ischemic/hemorrhagic stroke
-Epilepsy/Focal status
-Tumors/Diffuse gliomas-32737798
-Alzheimer’s disease-33622918
-CJD-30308445
-NMDA encephalitis-32061394/Rasmussen encephalitis-20473513
-Sturge-Weber-2288389
-Familial hemiplegic migraine(FHM)-9385760
Did you recognize the pattern here?
Every etiology includes cortical involvement (Tumors, too) & are mostly unilateral supratentorial cerebral pathologies. So in order to have contralateral cerebellar involvement, there has to be some connection between the two.
Every etiology includes cortical involvement (Tumors, too) & are mostly unilateral supratentorial cerebral pathologies. So in order to have contralateral cerebellar involvement, there has to be some connection between the two.
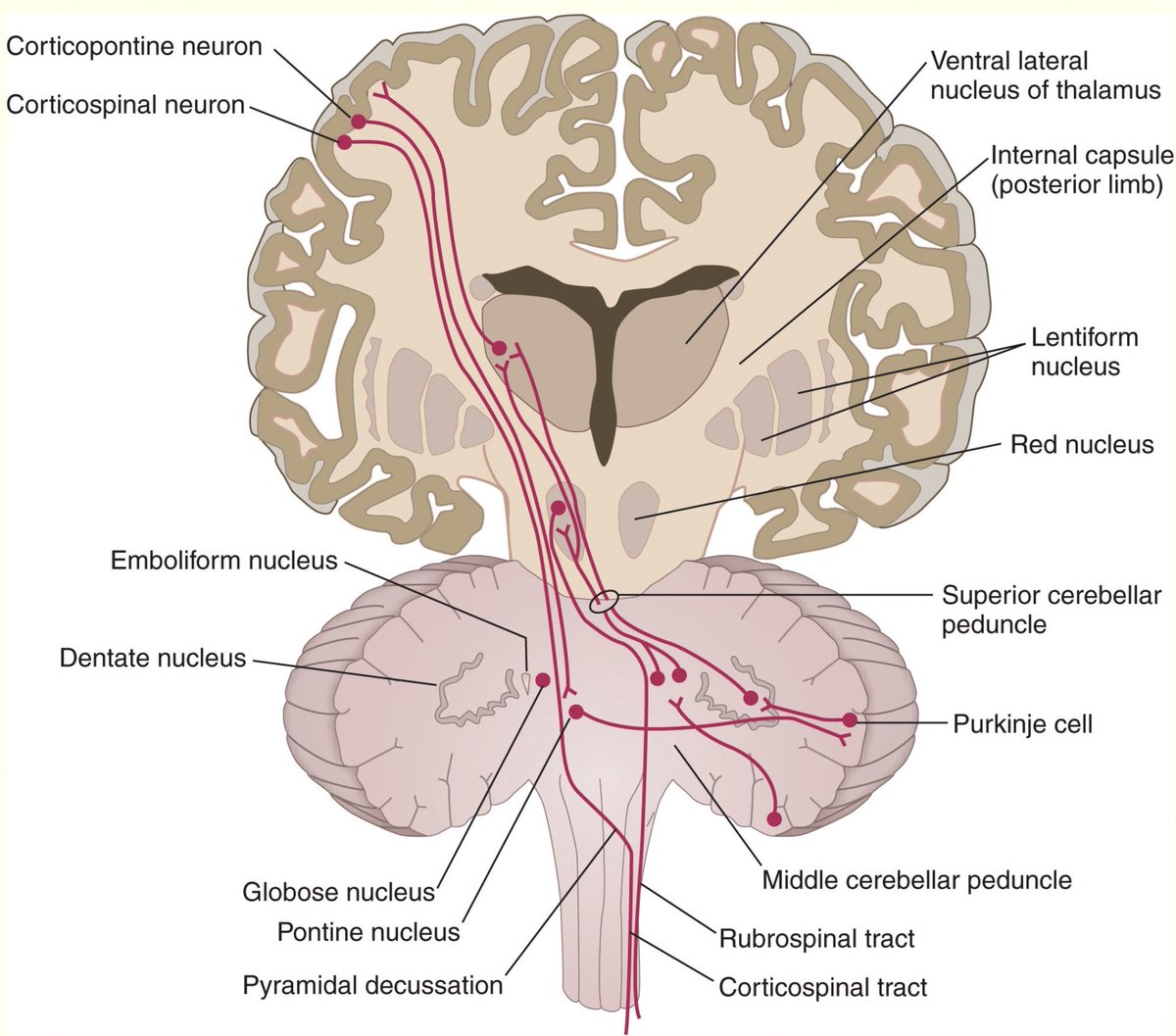
So there it is- Cortico-ponto-cerebellar (CPC) pathway.
For a plot twist, basal ganglia hemorrhagic strokes have also been found to cause CCD! (Brain isn’t always straight forward friends. If so, we - neurologists wouldn’t exist!)
Image source: humanphysiology.academy
For a plot twist, basal ganglia hemorrhagic strokes have also been found to cause CCD! (Brain isn’t always straight forward friends. If so, we - neurologists wouldn’t exist!)
Image source: humanphysiology.academy
So how this happens in the first place?
🤔
The cerebellum has a significant input from the cerebral hemispheres, the bulk of which is contained in the CPC pathway. The densest cortico-ponto-cerebellar projections arise from the precentral and prefrontal cortical areas-22473241
🤔
The cerebellum has a significant input from the cerebral hemispheres, the bulk of which is contained in the CPC pathway. The densest cortico-ponto-cerebellar projections arise from the precentral and prefrontal cortical areas-22473241
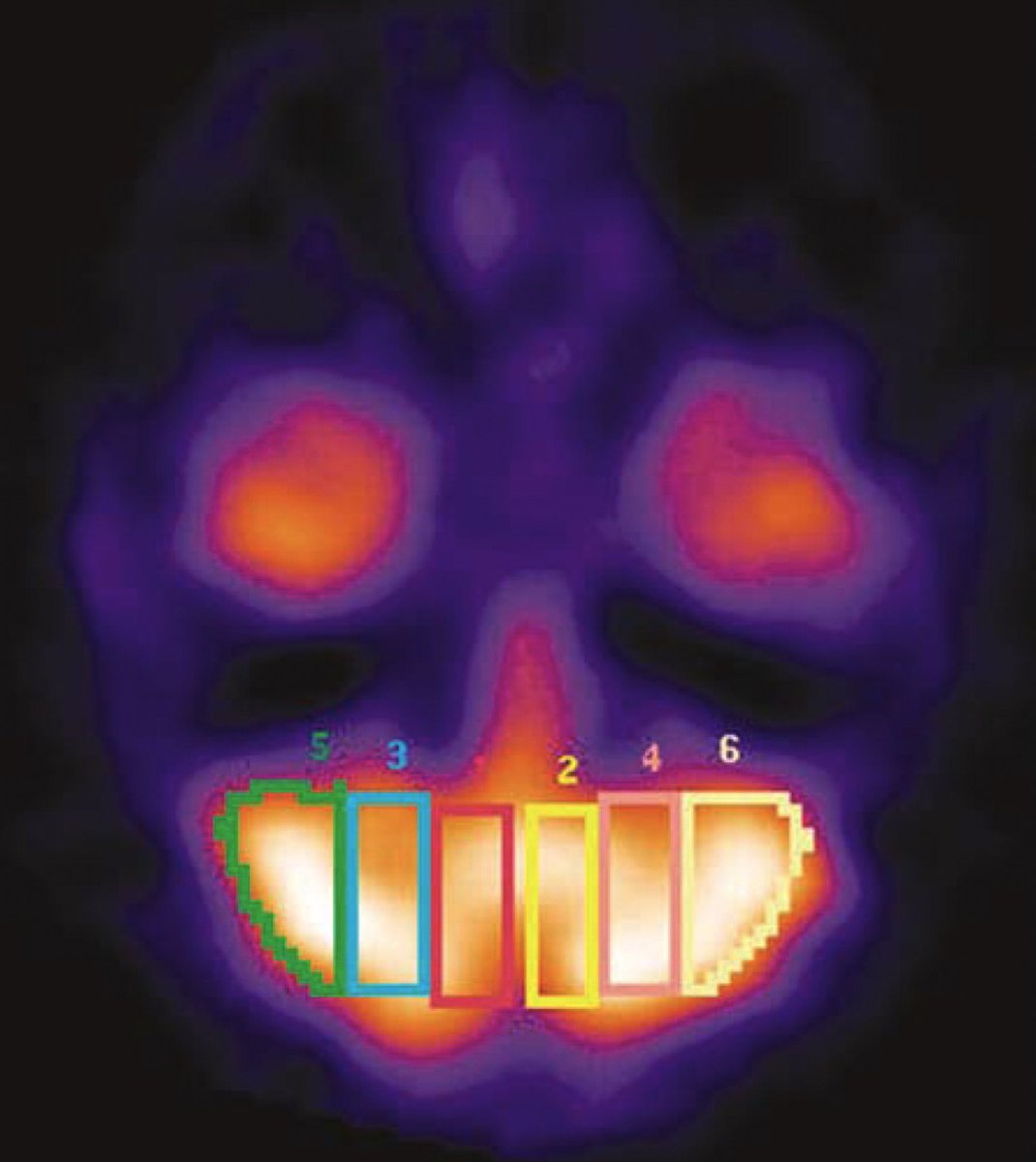
Reference image below:
The area of the cerebellum receiving most of those cortical input is intermediate area 3 and 4.
The areas 1 and 2 receive main input from spin-cerebella tract.
The areas 5 and 6 receive inputs mainly from cortico-olivo-cerebellar tract.
17311077
The area of the cerebellum receiving most of those cortical input is intermediate area 3 and 4.
The areas 1 and 2 receive main input from spin-cerebella tract.
The areas 5 and 6 receive inputs mainly from cortico-olivo-cerebellar tract.
17311077
Other cerebro-cerebellar connections are relayed through the inferior olive and reticular formation.
Other pathways postulated in pathophysiology are:
-cerebello-thalamo-cortical (CTC) pathway
-Spinocerebellar tract-2396276
-dentato-rubro-thalamic tract-10929283
Other pathways postulated in pathophysiology are:
-cerebello-thalamo-cortical (CTC) pathway
-Spinocerebellar tract-2396276
-dentato-rubro-thalamic tract-10929283
Now we know the pathway connecting the cerebrum with contralateral cerebellum, let’s understand the mechanism, which depends on the etiology only!!
1.Excitotoxicity(Epilepsy,ICH,CJD,encephalitis,SWS)
2.⬇️ blood flow due to cortical neuronal death (stroke,tumors,Alzheimer,FHM)
1.Excitotoxicity(Epilepsy,ICH,CJD,encephalitis,SWS)
2.⬇️ blood flow due to cortical neuronal death (stroke,tumors,Alzheimer,FHM)
Excitotoxicity:
Described to occur in ACUTE stage foll neurological🤕, often REVERSIBLE.
Status epilepticus 👉🏻⬆️perfusion in epileptogenic cortex to supply ⬆️metabolic demands. Seen radiologically as both vascular dilatation+⬆️ cerebral blood flow-31316646
Described to occur in ACUTE stage foll neurological🤕, often REVERSIBLE.
Status epilepticus 👉🏻⬆️perfusion in epileptogenic cortex to supply ⬆️metabolic demands. Seen radiologically as both vascular dilatation+⬆️ cerebral blood flow-31316646
Cortical neuronal hyper excitability also causes “hyper activation-deafferentation phenomenon”.
In acute stroke, deactivation of Purkinje cells caused by reduced excitatory input from the cerebral cortex and occurs immediately as response to reduced afferent input-22473241.
In acute stroke, deactivation of Purkinje cells caused by reduced excitatory input from the cerebral cortex and occurs immediately as response to reduced afferent input-22473241.
⬇️blood flow due to cortical neuronal death:
Described in SUBACUTE-CHRONIC phase, often IRREVERSIBLE. The proposed mechanism- Cortical neuronal degeneration following insult (stroke, Alzheimer’s) causes transsynaptic neuronal degeneration 2/2 ⛔️of CPC pathway.
Described in SUBACUTE-CHRONIC phase, often IRREVERSIBLE. The proposed mechanism- Cortical neuronal degeneration following insult (stroke, Alzheimer’s) causes transsynaptic neuronal degeneration 2/2 ⛔️of CPC pathway.
Now since we have understood this amazing phenomenon, what’s the practical implication? Or this is just a cool neurology talk with nothing to offer clinically? - like many used to think?
Well, not quite. Knowing CCD progression & mechanism can help with prognostication.
Read⬇️
Well, not quite. Knowing CCD progression & mechanism can help with prognostication.
Read⬇️
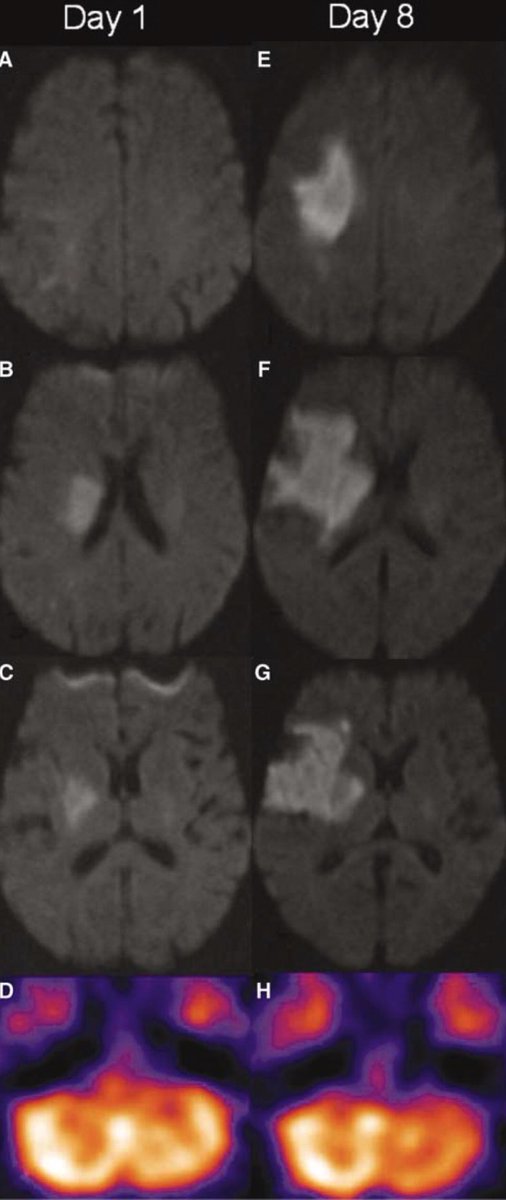
When CCD is due to seizure, imaging findings of persistent restricted diffusion & edema in chronic post-octal period predicts irreversible neuronal injury & poor outcome-26063348
Earlier the resolution of CCD, better the outcome.
Our patient above had reversible CCD on DWI.
Earlier the resolution of CCD, better the outcome.
Our patient above had reversible CCD on DWI.

When CCD is due to stroke,
-🤕with ICH or ICA/MCA territory stroke showed⬆️ incidence of CCD than those with other strokes
-not just cortical,but subcortical strokes ✂️CPC pathway can cause CCD
-⬆️stroke volume👉🏻⬆️chance of CCD
-🤕with CCD ⬆️ functional impairment
28084869
-🤕with ICH or ICA/MCA territory stroke showed⬆️ incidence of CCD than those with other strokes
-not just cortical,but subcortical strokes ✂️CPC pathway can cause CCD
-⬆️stroke volume👉🏻⬆️chance of CCD
-🤕with CCD ⬆️ functional impairment
28084869
Moral:
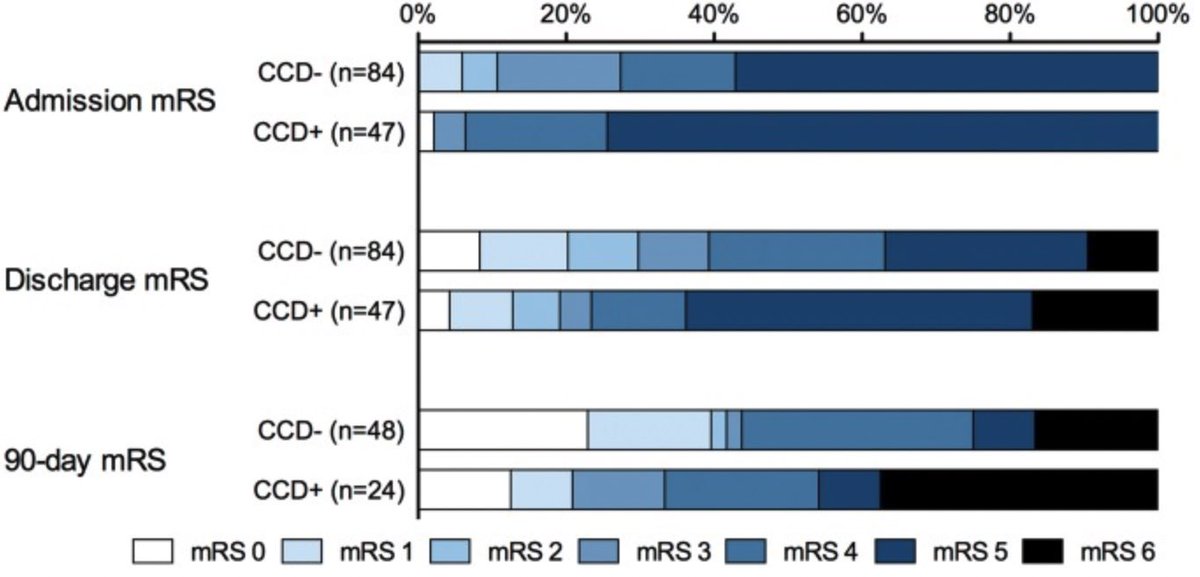
1. Mere presence of CCD in acute phase has no impact on functional outcome in ischemic stroke patients but persistence of CCD is associated with poor mRS-8126499
2. Occurrence of CCD with ICH;not hemorrhagic infarction = poor outcome compared to hemorrhagic infarct.
1. Mere presence of CCD in acute phase has no impact on functional outcome in ischemic stroke patients but persistence of CCD is associated with poor mRS-8126499
2. Occurrence of CCD with ICH;not hemorrhagic infarction = poor outcome compared to hemorrhagic infarct.
I find CCD an exceptional phenomenon revealing secrets of the brain that needs to be looked at closely! It offers an understanding of not only neuroanatomy but also clinical significance in terms of neurological outcome.
Who knows, one could use reverse physiology and gain control of intractable seizures through cerebellum using the same pathway or could stimulate neuroplasticity in cerebral cortex through cerebellum! Imagination has no limits.
Loading suggestions...