

@phlegmfighter posted an excellent thread on ventilation on asthma (linked below). He goes through the findings of a landmark study from 1987 by Tuxen and Lane. An interesting point raised in this thread is the TV you should start with in asthma
@phlemfighter eloquently demonstrates using data from the study & some calculations that gas trapping and alveolar ventilation is better with longer expiratory times and larger TVs. This makes perfect sense.
With increased resistance to expiration it takes longer to get gas out of the lung and larger lung volumes reduce resistance by making the airways bigger, helping expiratory flow.
When alveolar ventilation is maximised (and dead space ventilation minimised) by using higher tidal volumes, CO2 is controlled more efficiently.
He therefore calls in to question (perfectly reasonably) whether we should be using smaller tidal volumes in asthma
I’d like to offer a counter argument based on the same data. Figure 3 & 6 (see 🧵) demonstrate a few points. @phlemgmfighter rightly points out that larger TVs do not increase air trapping much & in fact if TV is adjusted to maintain normocapnia then larger TVs ⬇️ gas trapping.
BUT….lets take a step back. What kills ventilated asthmatics? They don’t die of hypercapnoea. It’s tamponade and CVS collapse as a result of TOTAL lung volume (sometimes including tension PTX). Let’s look at figure 3 again
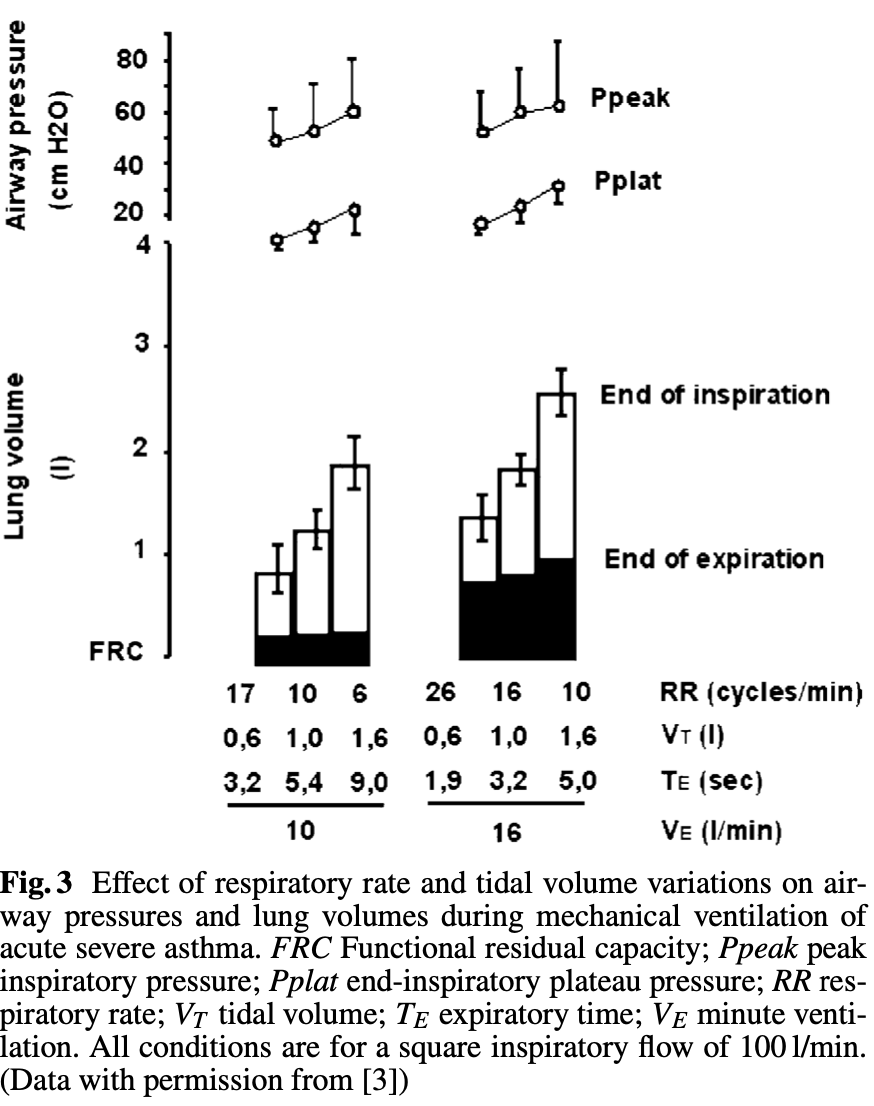
While trapping does not ⬆️ much with bigger TVs, total lung volume (TLV) increases greatly. What in fact this image shows us is that for a given minute volume, TLV (the really dangerous thing) is minimised with a low volume & high rate as opposed to a high volume and low rate.
Yes gas trapping, dead space ventilation and CO2 clearance will be better with larger volumes and low rates but again it is total lung volume that kills patients, not CO2.
@phlegmfigher ’s 🧵 links to a podcast by Tuxen. He presents a case of a young lady who was ventilated with a starting TV of 10mls/kg and RR of 12. She arrests in a matter of minutes (and regains an output after being declared dead and disconnected from the ventilator)
My approach based on Tuxen and Lane’s data would be to start at a TV of 6mls/kg and a rate of 16. It would be incredibly unusual for this to lead to CVS collapse in even the most severe asthmatic.
This may not be enough for adequate alveolar ventilation (even with permissive hypercapnoea). By all means increase the volume if the Pplat is <25 but start small and work up, not the other way around.
And in fact @phlegmfighter advocates at the end of his thread to start at 6-8mls/kg and only consider increasing TV if 'stuck between a rock and a hard place'.
Thankfully needing to ventilate asthmatics is now rare. But this lack of experience makes it all the more important to get it right.
And please follow @phlegmfighters advice to ignore peak pressure (reflects airway resistance not alveolar pressure), maximise expiratory time with a high flow rate/prolonged I:E ratio/short inspiratory time (these are all the same thing).
Summary: Volume control, TV 6mls/kg, RR 16, set pressure alarms to high (so ventilation not cut short), square or decelerating does not matter as long as I:E ratio set correctly (start with 1:3). PEEP 0-5.
Measure Pplat and keep it <25. TV can be increased if necessary for CO2 clearance if Pplat <25. Steps to minimise CO2 production are sensible.
Finally NEVER bag (hand ventilate) asthmatics. You need a ventilator to do it safely. And if there is CVS collapse disconnect the ventilator to allow the lungs to empty.
Good artilcle adding to Tuxen and Lane's paper here
link.springer.com
link.springer.com
Loading suggestions...