
1/
PEMPHIGUS FOLIACEOUS (PF), a #dermtwitter/#medtwitter #tweetorial!
How is this different than Pemphigus Vulgaris (PV)? Why do we not see blisters often? What's the desmoglein compensation theory?!
Read this #MedEd/#FOAMEd #thread & get your learn on!
PEMPHIGUS FOLIACEOUS (PF), a #dermtwitter/#medtwitter #tweetorial!
How is this different than Pemphigus Vulgaris (PV)? Why do we not see blisters often? What's the desmoglein compensation theory?!
Read this #MedEd/#FOAMEd #thread & get your learn on!

2/
The "pemphigus" part of the name means we are similarly dealing with an EPIDERMAL blistering disease, much like it's better known cousin, "pemphigus vulgaris" (PV).
If you haven't had a chance yet, take a look at my prior #tweetorial on PV:
The "pemphigus" part of the name means we are similarly dealing with an EPIDERMAL blistering disease, much like it's better known cousin, "pemphigus vulgaris" (PV).
If you haven't had a chance yet, take a look at my prior #tweetorial on PV:
3/
Before we get into the nitty gritty details of PF vs PV, a reminder that in pemphiguS, we're dealing with a SUPERFICIAL desmosome antigen target, so compared with pemphigoiD (that's DEEP), you're still going to get the + nikolsky, flaccid bullae, etc.
Before we get into the nitty gritty details of PF vs PV, a reminder that in pemphiguS, we're dealing with a SUPERFICIAL desmosome antigen target, so compared with pemphigoiD (that's DEEP), you're still going to get the + nikolsky, flaccid bullae, etc.

4/
BUT, it's not that simple. There are key differences BETWEEN PF and PV. As I always say here, the exam is everything.
PV (1) tends to make flaccid blisters with a + Nikolsky.
PF (2) theoretically does too, but in real life, blisters are rarely seen because they're so fragile!
BUT, it's not that simple. There are key differences BETWEEN PF and PV. As I always say here, the exam is everything.
PV (1) tends to make flaccid blisters with a + Nikolsky.
PF (2) theoretically does too, but in real life, blisters are rarely seen because they're so fragile!


5/
Instead, in PF, we often identify it by the scale. A great example was the first tweet of the #thread. It's a good example of the "cornflake" scale seen in PF.
Why do you think there is this difference in exam between PF and PV?
Instead, in PF, we often identify it by the scale. A great example was the first tweet of the #thread. It's a good example of the "cornflake" scale seen in PF.
Why do you think there is this difference in exam between PF and PV?
6/
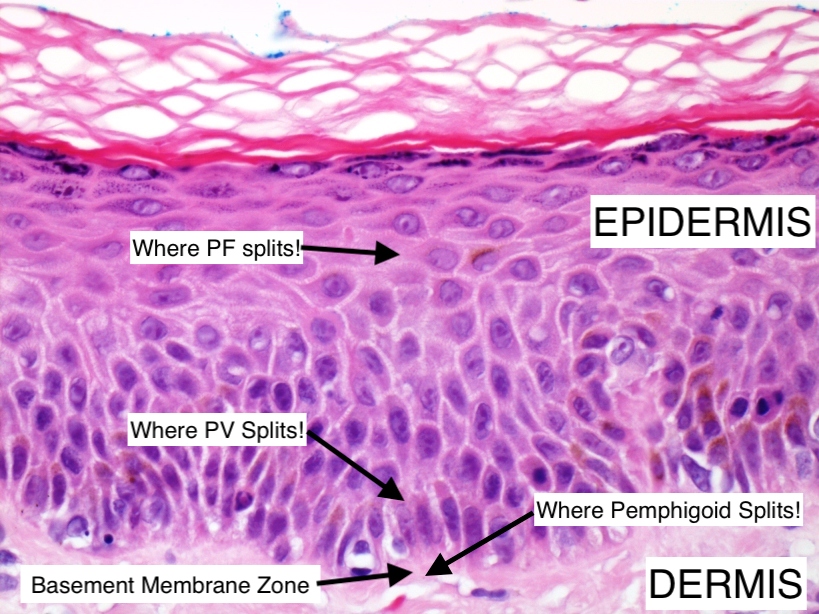
The split in PF is HIGHER than PV. But...I just told me all pemphigus is higher/more superficial than pemphigoid, right?
Yes, that's true, but WITHIN the pemphigus family, the epidermal level at which the split happens is different👀👇
(pc:tissupath.com.au)
The split in PF is HIGHER than PV. But...I just told me all pemphigus is higher/more superficial than pemphigoid, right?
Yes, that's true, but WITHIN the pemphigus family, the epidermal level at which the split happens is different👀👇
(pc:tissupath.com.au)
7/
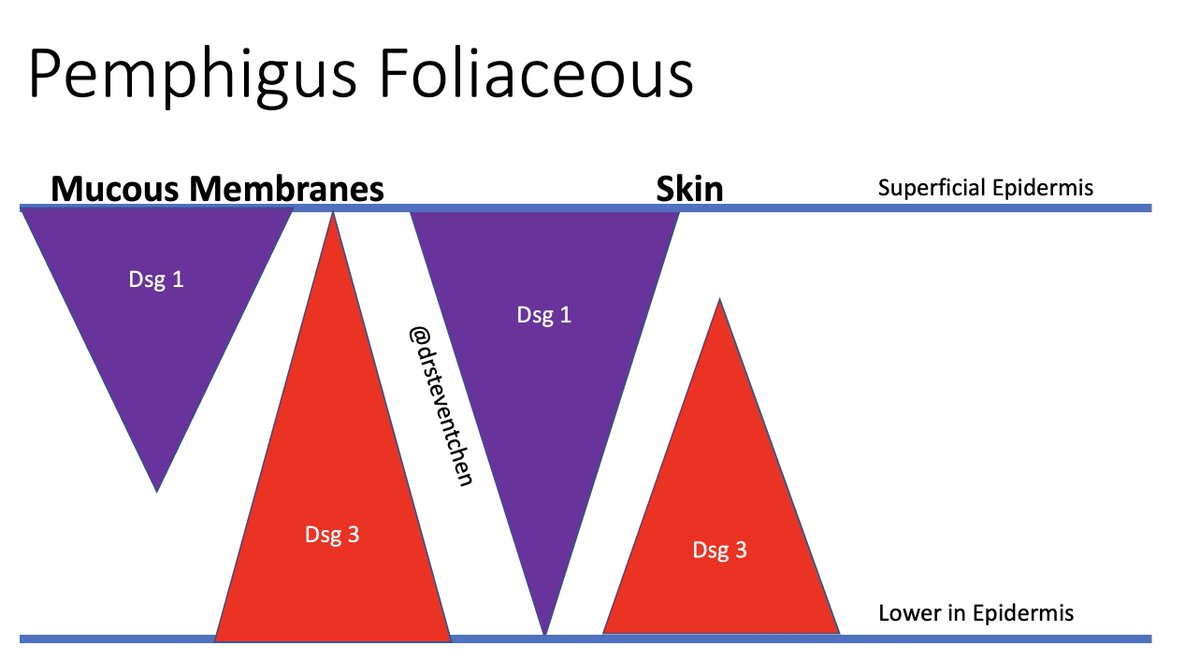
This is because the autoantibody target in PF is different than in PV.
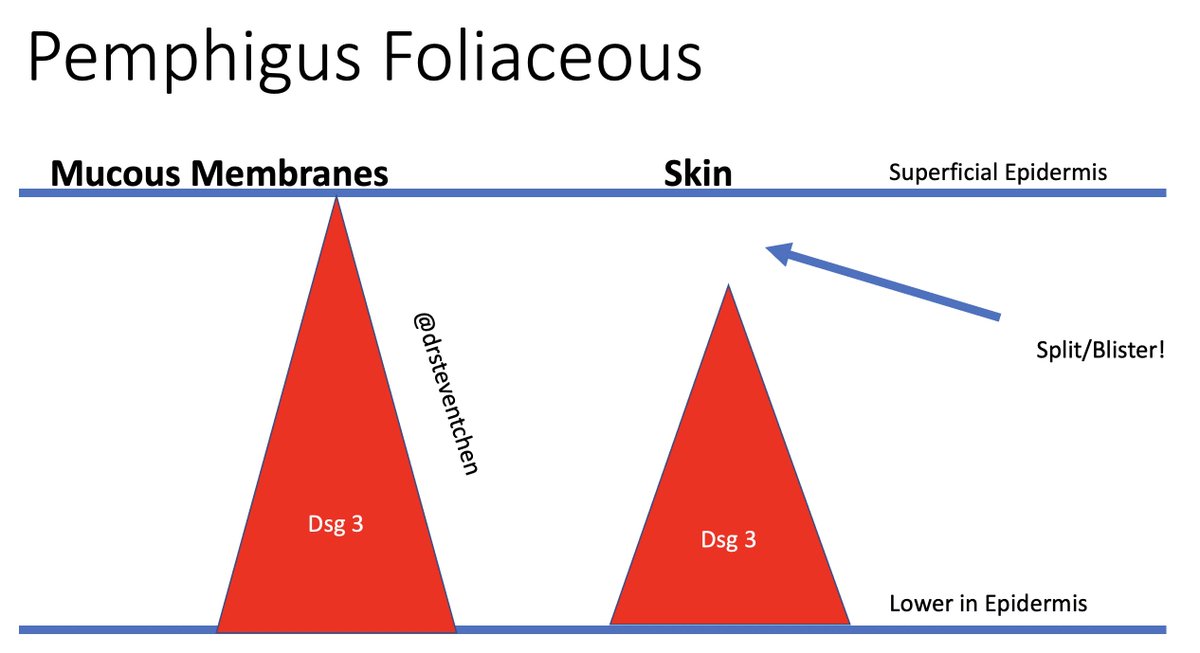
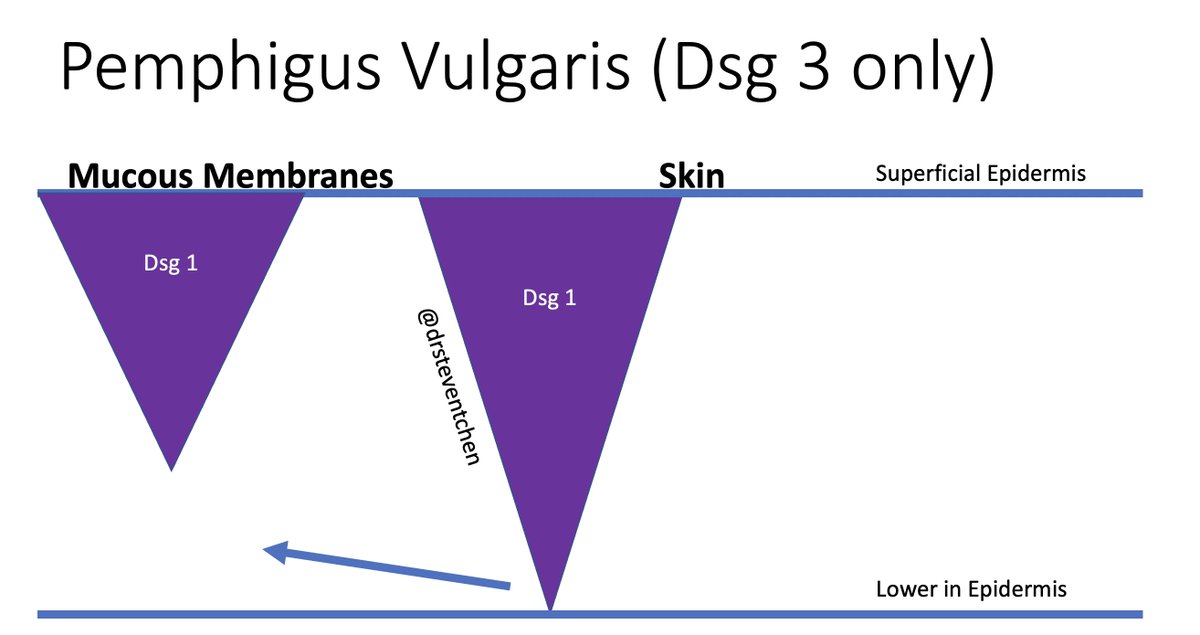
PF = Desmoglein (Dsg) 1
PV = Dsg 3 (+/- Dsg 1)
While it's all desmosome, the level of expression depends on the epidermal level! There's more Dsg 1 up top, more Dsg 3 below (width of the triangles👇).
This is because the autoantibody target in PF is different than in PV.
PF = Desmoglein (Dsg) 1
PV = Dsg 3 (+/- Dsg 1)
While it's all desmosome, the level of expression depends on the epidermal level! There's more Dsg 1 up top, more Dsg 3 below (width of the triangles👇).
8/
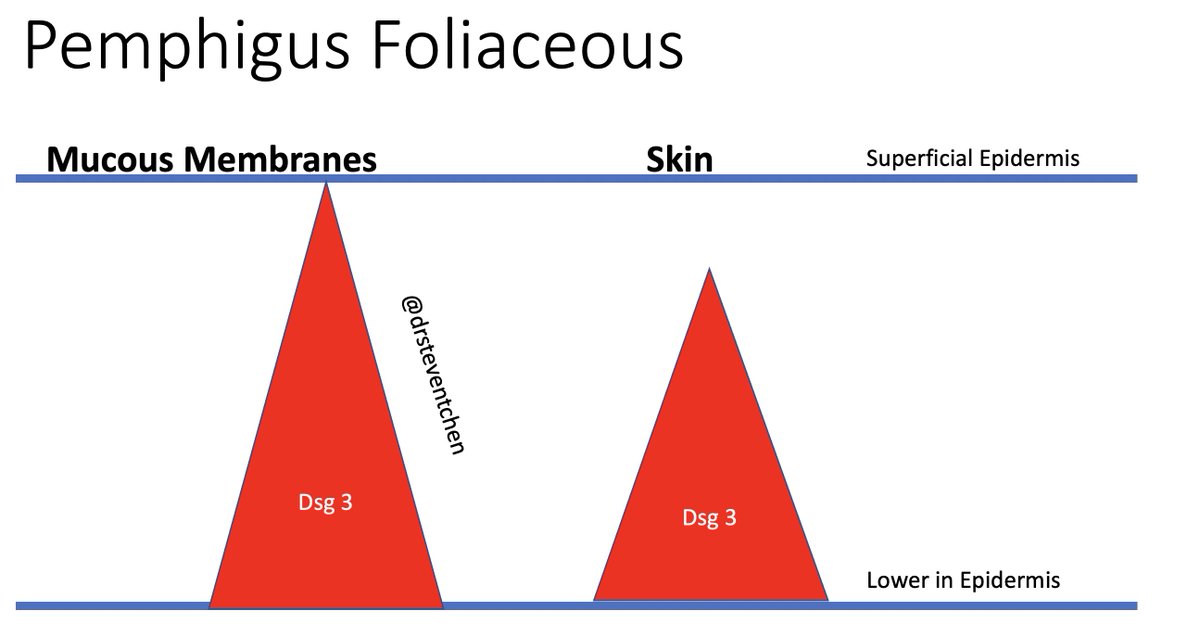
Okay, so let's say you're Abs mess up all your Dsg 1. Then the Dsg1 goes away. That means you're left with just the red Dsg3👇
Do you see how the Dsg 3 spans the entirety of the mucous membrane epidermis (left)? That means mucosal skin has enough Dsg 3 to stay intact!
Okay, so let's say you're Abs mess up all your Dsg 1. Then the Dsg1 goes away. That means you're left with just the red Dsg3👇
Do you see how the Dsg 3 spans the entirety of the mucous membrane epidermis (left)? That means mucosal skin has enough Dsg 3 to stay intact!
9/
But on the Skin side, you don't have enough Dsg3 to span the entire epidermis, so a split occurs where the arrow is pointing, leading to a blister!
This is also why in PF, you DON'T see lesions in the mouth, because the Dsg3 will always hold things together!
But on the Skin side, you don't have enough Dsg3 to span the entire epidermis, so a split occurs where the arrow is pointing, leading to a blister!
This is also why in PF, you DON'T see lesions in the mouth, because the Dsg3 will always hold things together!
10/
Ok, let's work through PV. If all the Dsg 3 is gone, but you still have Dsg1, there is enough Dsg 1 to hold the skin together, but not in the mucous membranes. So you ALWAYS should get mucosal lesions in PV!
This is the DESMOGLEIN COMPENSATION THEORY! It's it beautiful?😍
Ok, let's work through PV. If all the Dsg 3 is gone, but you still have Dsg1, there is enough Dsg 1 to hold the skin together, but not in the mucous membranes. So you ALWAYS should get mucosal lesions in PV!
This is the DESMOGLEIN COMPENSATION THEORY! It's it beautiful?😍
11/
That was a longwinded way to show why in PF, you DON'T get mucosal lesions, and why you get a higher split.
And what this translates too is very fragile blisters that often break so quickly that all you see is the scale/crust afterward.
pc: scielo.br
That was a longwinded way to show why in PF, you DON'T get mucosal lesions, and why you get a higher split.
And what this translates too is very fragile blisters that often break so quickly that all you see is the scale/crust afterward.
pc: scielo.br


12/
For that reason, PF is often misdiagnosed as psoriasis, pityriasis, eczema, etc.
A quick note to say that there is one other disease entity that has the same pathophysiology (targeting Dsg1), but is not autoantibody mediated. What do you think it is?
For that reason, PF is often misdiagnosed as psoriasis, pityriasis, eczema, etc.
A quick note to say that there is one other disease entity that has the same pathophysiology (targeting Dsg1), but is not autoantibody mediated. What do you think it is?
13/
Staphylococcal Scalded Skin Syndrome (SSSS) is from Staph toxin that cleaves the Dsg 1, so you get a similar superficial eroded blister! Check out my previous #tweetorial on SSSS if you'd like:
Staphylococcal Scalded Skin Syndrome (SSSS) is from Staph toxin that cleaves the Dsg 1, so you get a similar superficial eroded blister! Check out my previous #tweetorial on SSSS if you'd like:
14/
Interestingly, PF is also hypothesized to be related to the bite of the black fly, Simulium nigrimanum.
Fogo Selvagem, endemic in South America, occurs in patients with certain HLA after a fly's bite, maybe related to the fly's salivary protein!
pc: fogoselvagem.org
Interestingly, PF is also hypothesized to be related to the bite of the black fly, Simulium nigrimanum.
Fogo Selvagem, endemic in South America, occurs in patients with certain HLA after a fly's bite, maybe related to the fly's salivary protein!
pc: fogoselvagem.org

15/
Let's talk treatment. Basically, it's similar to PV.
In a pre-COVID world, Rituximab was used freely to induce a remission by targeting the Ab producing B-cells. With COVID implications, we're using more mycophenolate, azathioprine, etc.
See my PV #tweetorial for more!
Let's talk treatment. Basically, it's similar to PV.
In a pre-COVID world, Rituximab was used freely to induce a remission by targeting the Ab producing B-cells. With COVID implications, we're using more mycophenolate, azathioprine, etc.
See my PV #tweetorial for more!
16/
But PF often is more recalcitrant and harder to treat than PV. I don't know why exactly, but it does make the rituximab decision tough because we don't want to miss an opportunity treat the patient aggressively, but we have to balance that in the setting of a pandemic.
But PF often is more recalcitrant and harder to treat than PV. I don't know why exactly, but it does make the rituximab decision tough because we don't want to miss an opportunity treat the patient aggressively, but we have to balance that in the setting of a pandemic.
17/
Summary:
✔️PF is from Ab targeting Dsg 1, expressed higher up in the epidermis
✔️"Dsg Compensation Theory" explains the lack of mucosal lesions
✔️There might not be blisters, just scale/crust, since it's so superficial
✔️Treatment is immunosuppression, but it's complicated.
Summary:
✔️PF is from Ab targeting Dsg 1, expressed higher up in the epidermis
✔️"Dsg Compensation Theory" explains the lack of mucosal lesions
✔️There might not be blisters, just scale/crust, since it's so superficial
✔️Treatment is immunosuppression, but it's complicated.
18/18
Thanks for joining on this slightly longer #tweetorial! I hope everyone took a little something away from it! As always, if you have more tips/tricks/info you'd like to share, please feel free to jump in!
Thanks for joining on this slightly longer #tweetorial! I hope everyone took a little something away from it! As always, if you have more tips/tricks/info you'd like to share, please feel free to jump in!

Loading suggestions...