

What's going on with the intra-aortic balloon pump (IABP)?
Here's a practical🧵 for all residents and fellows during their time on rotation in the cardiac ICU.
Learning objectives
🎈 basics of the IABP
🎈 IABP alarms
🎈 ways to fix them
#CardioTwitter #Medtwitter #tweetorial
Here's a practical🧵 for all residents and fellows during their time on rotation in the cardiac ICU.
Learning objectives
🎈 basics of the IABP
🎈 IABP alarms
🎈 ways to fix them
#CardioTwitter #Medtwitter #tweetorial
Let's start with the basics.
Developed in the 1950s by the Kantrowitz brothers, IABPs have been in clinical practice since the first implant in 1967 at @MaimonidesMC Currently, it is still widely used as modest temporary mechanical circulatory support for cardiogenic shock
Developed in the 1950s by the Kantrowitz brothers, IABPs have been in clinical practice since the first implant in 1967 at @MaimonidesMC Currently, it is still widely used as modest temporary mechanical circulatory support for cardiogenic shock
The mechanism of IABP begins with rapid deflation of the helium filled balloon (helium moves faster than air) at the onset of systole. This creates a vacuum effect which reduces the work load of the heart during all of systole thereby reducing afterload
To understand this phenomenon, imagine pushing open a heavy door only to realize that someone happens to be simultaneously pulling the door open on the other side
This is followed by inflation of the balloon during all of diastole starting at the moment of aortic valve closure. This displaces blood from the thoracic aorta to peripheral tissues including the coronary arteries.
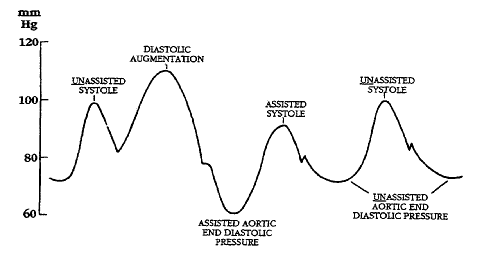
This produces the following hemodynamic changes:
⬇️ systolic blood pressure following diastolic augmentation due to ⬇️ afterload and
⬆️ diastolic blood pressure that facilitates ⬆️ coronary blood flow (called diastolic augmentation)
⬇️ systolic blood pressure following diastolic augmentation due to ⬇️ afterload and
⬆️ diastolic blood pressure that facilitates ⬆️ coronary blood flow (called diastolic augmentation)
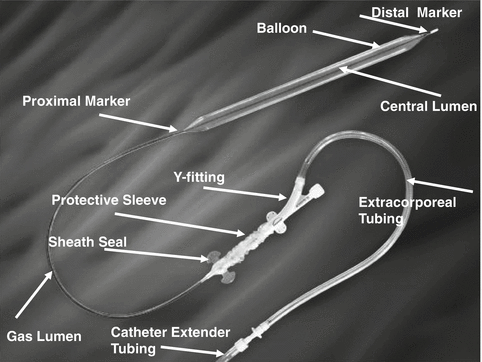
So what are the important components of an IABP?
Central lumen: for placement of the IABP over a wire, transducing a continuous arterial waveform (newer models use fiberoptics).
Gas lumen: supplies helium to balloon around central lumen
Markers: radiopaque for positioning
Central lumen: for placement of the IABP over a wire, transducing a continuous arterial waveform (newer models use fiberoptics).
Gas lumen: supplies helium to balloon around central lumen
Markers: radiopaque for positioning
IABPs are properly positioned in the aorta below the left subclavian artery (have traditionally been placed transfemorally, but a common alternative is transaxillary which allows for easier ambulation if used for longer periods of time)
pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
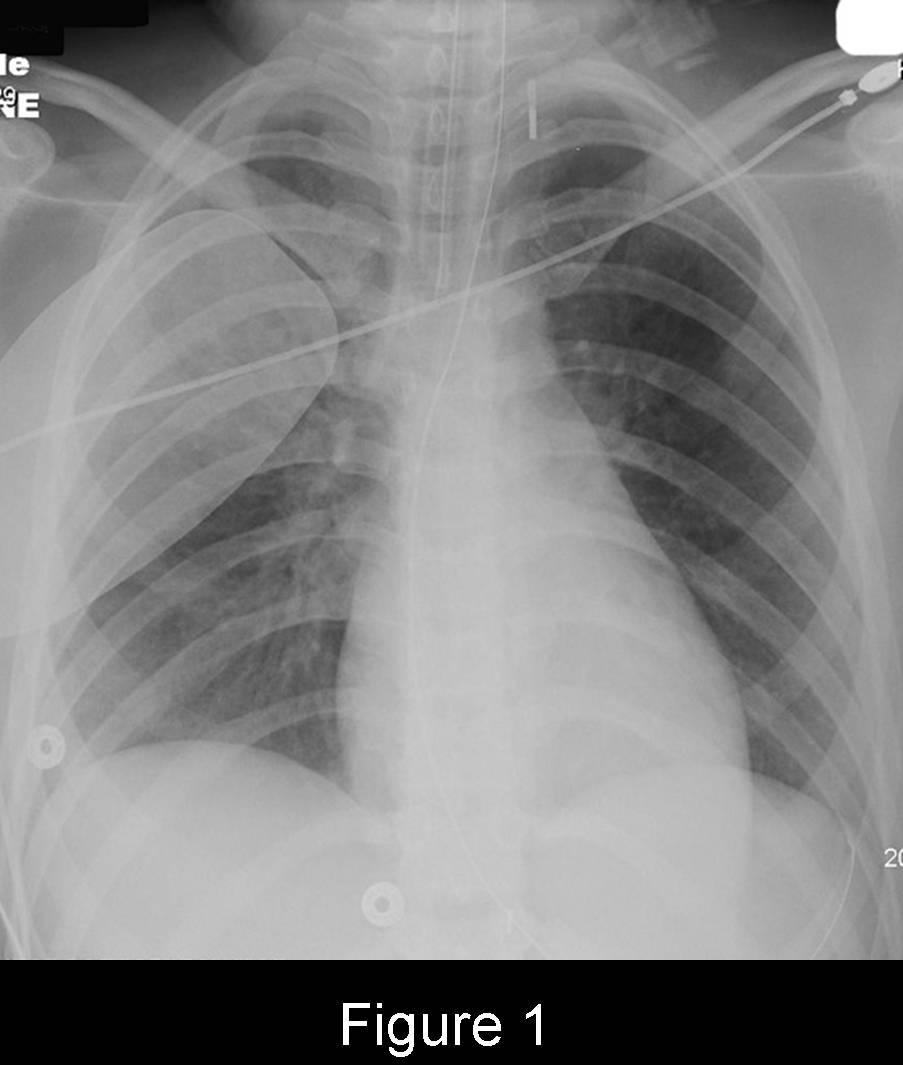
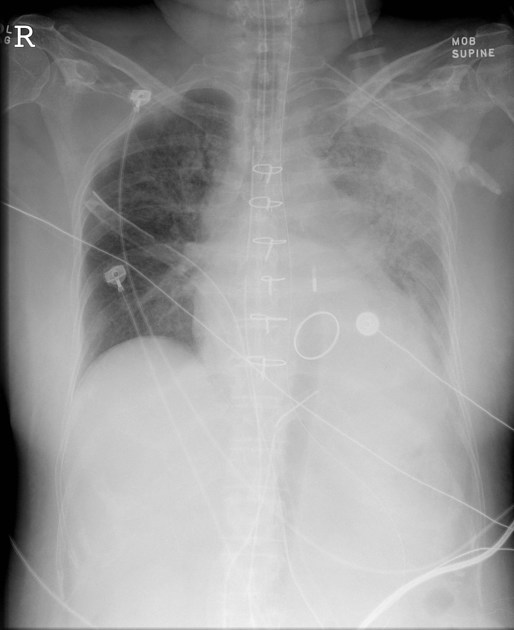
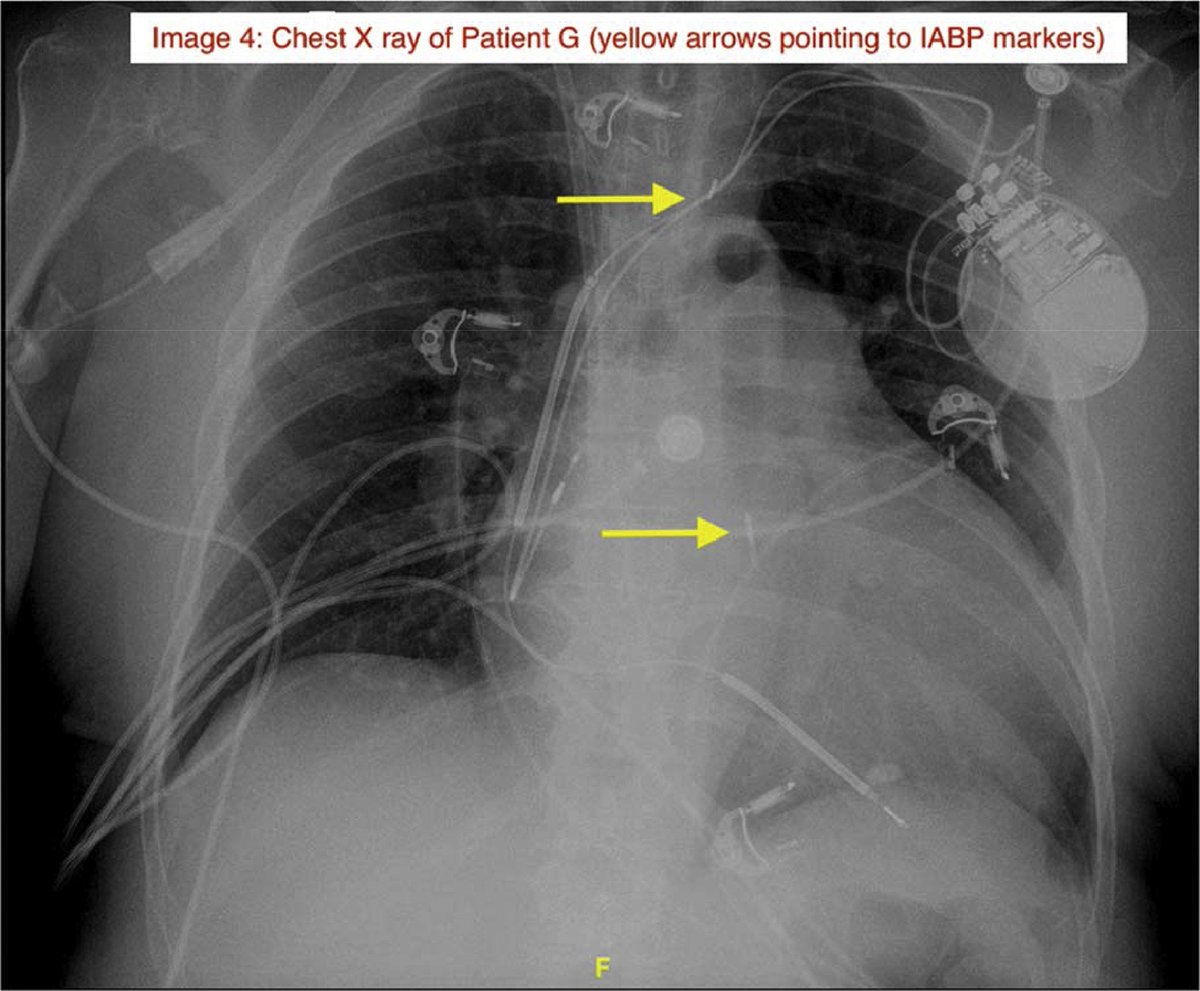
How do we know the IABP is in the right position? Check the markers!
Proximal marker should be located 2cm above the carina in aortic knob (see 👇)
Sometimes you can see distal marker inferiorly (should be 22-26cm apart depending on size of IABP and curvature of the aorta)
Proximal marker should be located 2cm above the carina in aortic knob (see 👇)
Sometimes you can see distal marker inferiorly (should be 22-26cm apart depending on size of IABP and curvature of the aorta)

What if the proximal IABP is not in the correct position? Let's start with it being too high:
⬆️ risk of obstruction of L subclavian, embolization of aortic arch atherosclerosis and stroke
if axillary - advance the catheter to desired length
if femoral - retract the catheter
⬆️ risk of obstruction of L subclavian, embolization of aortic arch atherosclerosis and stroke
if axillary - advance the catheter to desired length
if femoral - retract the catheter
What if the IABP marker is too low?
⬇️ diastolic augmentation, ⬇️ afterload reduction and ⬆️ risk of obstruction of splanchnic vessels (think new severe abdominal pain)
if axillary - retract the catheter to desired length
if femoral - advance the catheter
⬇️ diastolic augmentation, ⬇️ afterload reduction and ⬆️ risk of obstruction of splanchnic vessels (think new severe abdominal pain)
if axillary - retract the catheter to desired length
if femoral - advance the catheter
What if the IABP markers are too close?
Unlikely to occur in femoral position, can rarely occur in axillary position due to 🚶🚶
Can be due to coiling, folding, and migration into ascending aorta
Often only way to fix it is to exchange the 🎈 or place femorally
Unlikely to occur in femoral position, can rarely occur in axillary position due to 🚶🚶
Can be due to coiling, folding, and migration into ascending aorta
Often only way to fix it is to exchange the 🎈 or place femorally
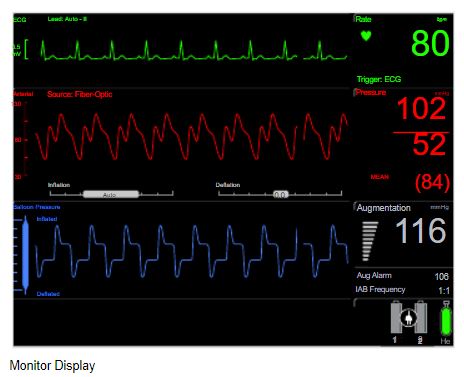
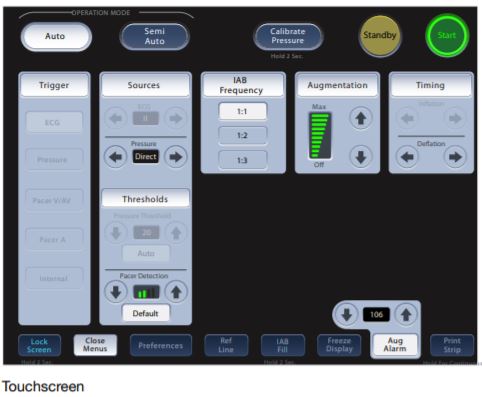
This is a typical IABP monitor. A few important points to note:
Arterial waveform source: fiberoptics vs arterial line
Trigger source (what identifies next cardiac cycle): ECG vs arterial waveform vs pacer spikes (only use if 100% paced)
IAB frequency: 1:1 (augment every beat)
Arterial waveform source: fiberoptics vs arterial line
Trigger source (what identifies next cardiac cycle): ECG vs arterial waveform vs pacer spikes (only use if 100% paced)
IAB frequency: 1:1 (augment every beat)
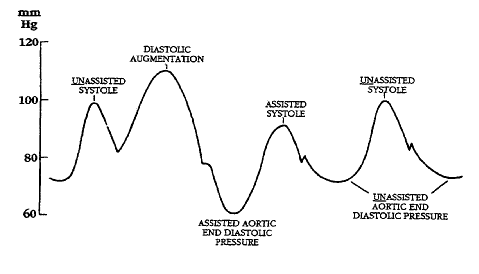
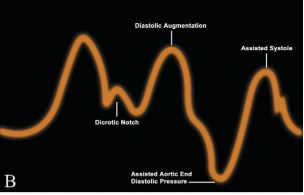
Proper timing of the IABP must follow a set of rules:
1️⃣ inflation occurs at the dicrotic notch (forming a sharp "v")
2️⃣ augmented DBP exceeds or equals SBP
3️⃣ assisted SBP is < unassisted SBP by at least 5mmHg
4️⃣ assisted DBP is < unassisted DBP by 15-20mmHg
1️⃣ inflation occurs at the dicrotic notch (forming a sharp "v")
2️⃣ augmented DBP exceeds or equals SBP
3️⃣ assisted SBP is < unassisted SBP by at least 5mmHg
4️⃣ assisted DBP is < unassisted DBP by 15-20mmHg
There are a number of scenarios that can occur as a result of mistiming of the IABP
⏲️ early inflation
⏲️ late inflation
⏲️ early deflation
⏲️ late deflation
Let's first start with the case of early inflation...
⏲️ early inflation
⏲️ late inflation
⏲️ early deflation
⏲️ late deflation
Let's first start with the case of early inflation...
In early inflation,
Inflation occurs before the dicrotic notch (rule 1 is broken).
Effects include premature closure of aortic valve, ⬇️ CO, and ⬆️ myocardial oxygen consumption
Inflation occurs before the dicrotic notch (rule 1 is broken).
Effects include premature closure of aortic valve, ⬇️ CO, and ⬆️ myocardial oxygen consumption
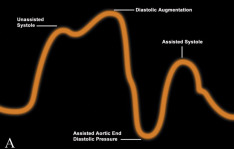
In late inflation,
Inflation occurs far enough after dicrotic notch causing loss of the sharp "v" (rule 1 is broken)
Effects include ⬇️ diastolic augmentation (rule 2 is broken) and ⬇️ coronary perfusion
Inflation occurs far enough after dicrotic notch causing loss of the sharp "v" (rule 1 is broken)
Effects include ⬇️ diastolic augmentation (rule 2 is broken) and ⬇️ coronary perfusion
In early deflation,
Deflation occurs before isovolumetric contraction resulting in sharp descent on waveform
Effects include no reduction in assisted SBP (rule 3 is broken), ⬇️ coronary perfusion, and ⬆️ myocardial oxygen consumption
Deflation occurs before isovolumetric contraction resulting in sharp descent on waveform
Effects include no reduction in assisted SBP (rule 3 is broken), ⬇️ coronary perfusion, and ⬆️ myocardial oxygen consumption
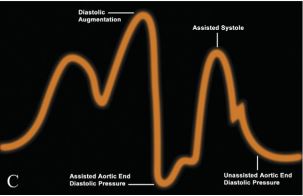
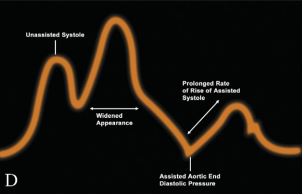
In late deflation,
Deflation is occurring during contraction resulting in prolonged rise in assisted SBP on waveform
Effects include ⬆️ afterload, ⬆️ myocardial oxygen consumption, ⬆️ assisted DBP (rule 4 is broken)
Deflation is occurring during contraction resulting in prolonged rise in assisted SBP on waveform
Effects include ⬆️ afterload, ⬆️ myocardial oxygen consumption, ⬆️ assisted DBP (rule 4 is broken)
So what happens when things go awry? Let's break it down into the major categories of IABP malfunction
🎈 balloon may not be adequately augmenting cardiac output (CO)
🎈 ECG trigger may not be functioning properly
🎈 flow of helium may be impaired or absent
🎈 balloon may not be adequately augmenting cardiac output (CO)
🎈 ECG trigger may not be functioning properly
🎈 flow of helium may be impaired or absent
Augmentation alarms can occur for many reasons:
⬇️ SVR or CO (sepsis, worsening cardiogenic shock, new arrhythmia)
⬇️ helium delivery to balloon (leak in catheter or gas circuit, 🎈rupture/tear)
⬇️ balloon function (incorrect timing, impaired 🎈 opening)
⬇️ SVR or CO (sepsis, worsening cardiogenic shock, new arrhythmia)
⬇️ helium delivery to balloon (leak in catheter or gas circuit, 🎈rupture/tear)
⬇️ balloon function (incorrect timing, impaired 🎈 opening)
How do we address augmentation alarms?
💔See the patient! How do they look?
💔Confirm correct placement with CXR (marker 2cm above carina within aortic knob and 22-26cm apart)
💔Evaluate waveform, is it appropriate?
💔Address underlying cause (abx, inotropes, antiarrhythmics)
💔See the patient! How do they look?
💔Confirm correct placement with CXR (marker 2cm above carina within aortic knob and 22-26cm apart)
💔Evaluate waveform, is it appropriate?
💔Address underlying cause (abx, inotropes, antiarrhythmics)
Failure of ECG triggering can occur due to:
💔Poor lead placement
💔Low ECG voltage
💔New arrhythmia (irregular R wave intervals make it difficult to trigger especially at ⬆️ heart rates )
💔Poor lead placement
💔Low ECG voltage
💔New arrhythmia (irregular R wave intervals make it difficult to trigger especially at ⬆️ heart rates )
How do we address issues with ECG triggering?
💔Check electrode placement and tracing for low voltage or new dysrhythmia (replace leads if needed)
💔Consider switching to arterial pressure triggering temporarily
💔if extreme tachycardia, reduce timing from 1:1 to 1:2 or 1:3
💔Check electrode placement and tracing for low voltage or new dysrhythmia (replace leads if needed)
💔Consider switching to arterial pressure triggering temporarily
💔if extreme tachycardia, reduce timing from 1:1 to 1:2 or 1:3
Impaired or absent helium flow indicates a non-functioning 🎈 and represents an emergency! Some causes are:
💔Restriction (in catheter or tubing, during inflation/deflation)
💔Helium loss from circuit
💔All out of helium
💔Restriction (in catheter or tubing, during inflation/deflation)
💔Helium loss from circuit
💔All out of helium
How should we address issues with impaired helium flow?
💔Check circuit, if blood (see 👇) then STOP 🎈 as it must be replaced now
💔If no blood, check all sites of connection as any kink can cause restriction
💔Check helium supply
💔Check CXR to confirm proper position
💔Check circuit, if blood (see 👇) then STOP 🎈 as it must be replaced now
💔If no blood, check all sites of connection as any kink can cause restriction
💔Check helium supply
💔Check CXR to confirm proper position

Remember, do not touch the IABP panel if you are not familiar and trained with the IABP and only if and when you have approval from your attending. If you are a resident, call your fellow and/or attending immediately if these issues arise.
Special thanks to @AHajduczok, Gregary Marhefka MD, Indranee Rajapreyar MD, and @YevgeniyBr for help with this🧵.
Recommendations for further reading:
pubmed.ncbi.nlm.nih.gov
jcvaonline.com
#relatedArticles" target="_blank" rel="noopener" onclick="event.stopPropagation()">onlinejcf.com
Recommendations for further reading:
pubmed.ncbi.nlm.nih.gov
jcvaonline.com
#relatedArticles" target="_blank" rel="noopener" onclick="event.stopPropagation()">onlinejcf.com
Loading suggestions...