

1/
Hello #NeuroTwitter
Ready for our next case?
A 40 year old woman presents with back pain and unsteady gait.
One week ago, she had a mild viral URI.
Over the coming days, she developed progressive lower extremity weakness and urinary retention.
Hello #NeuroTwitter
Ready for our next case?
A 40 year old woman presents with back pain and unsteady gait.
One week ago, she had a mild viral URI.
Over the coming days, she developed progressive lower extremity weakness and urinary retention.
2/
Neurologic exam:
▶️Flaccid paraparesis
▶️Numbness from the knees down
▶️Flexor plantar responses
MRI below:
Neurologic exam:
▶️Flaccid paraparesis
▶️Numbness from the knees down
▶️Flexor plantar responses
MRI below:

3/
What do we do next?
What do we do next?
4/
Let's begin with our basics:
Our time to neurologic nadir in this case fits a subacute onset (1 - 21 days)...
Which if you remember suggests a myelitis with a potential inflammatory or infectious cause.
Let's begin with our basics:
Our time to neurologic nadir in this case fits a subacute onset (1 - 21 days)...
Which if you remember suggests a myelitis with a potential inflammatory or infectious cause.
5/
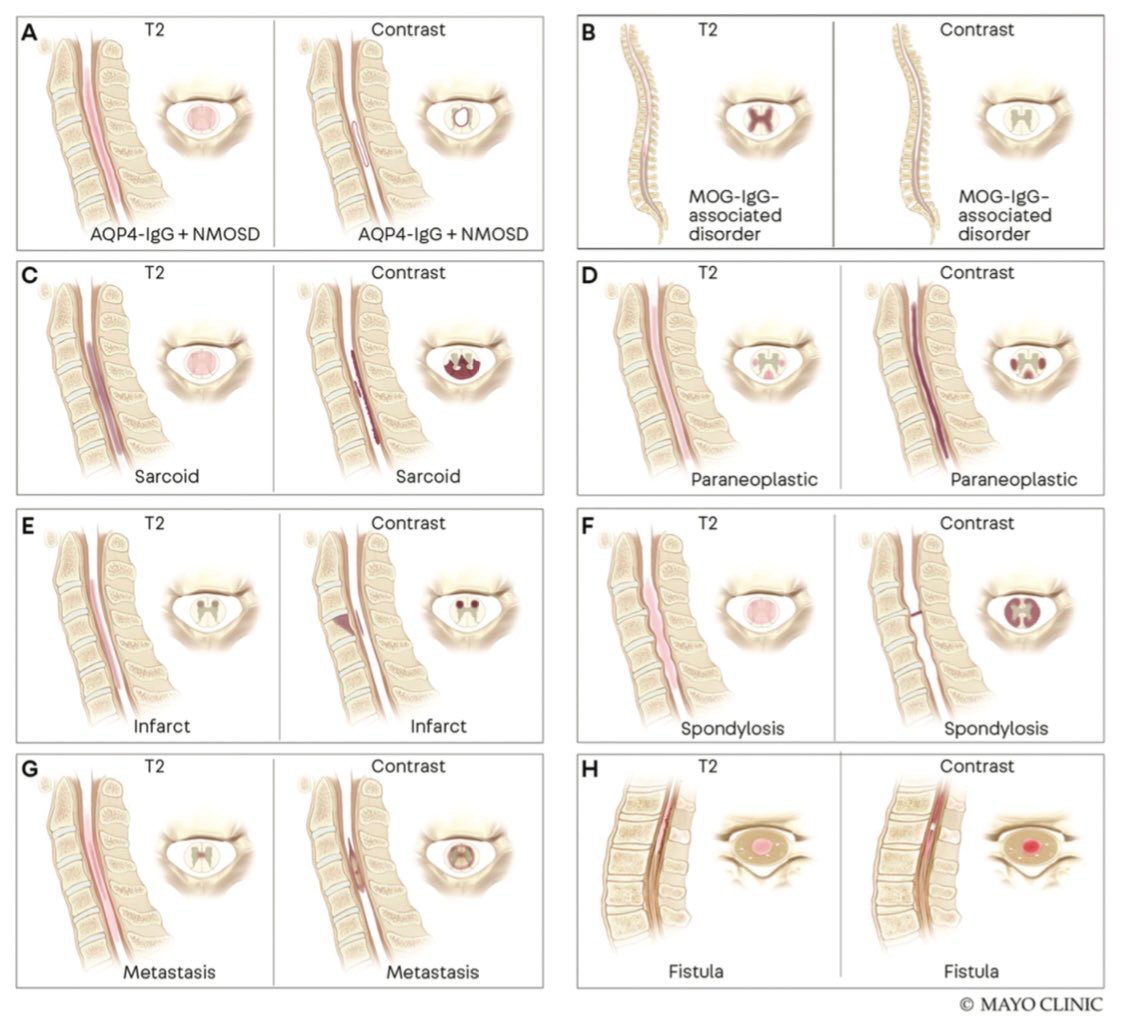
At this point I'd highly recommend reading @mdsebaslopez's & @EoinFlanagan14's @ContinuumAAN article on myelitis:
journals.lww.com
At this point I'd highly recommend reading @mdsebaslopez's & @EoinFlanagan14's @ContinuumAAN article on myelitis:
journals.lww.com
6/
Their article highlights some imaging patterns of longitudinally extensive transverse myelitis (LETM), as in our case, that can be quite helpful with making the diagnosis.
Their article highlights some imaging patterns of longitudinally extensive transverse myelitis (LETM), as in our case, that can be quite helpful with making the diagnosis.
7/
You may have noticed in our images, on axial T2, that the gray matter was predominantly affected forming an "H" sign or mimicking some of the fun images below.
The gadolinium enhancement pattern was pretty nonspecific.
This can be seen commonly in MOG-IgG myelitis
You may have noticed in our images, on axial T2, that the gray matter was predominantly affected forming an "H" sign or mimicking some of the fun images below.
The gadolinium enhancement pattern was pretty nonspecific.
This can be seen commonly in MOG-IgG myelitis
8/
In such cases, it can be helpful to obtain CSF studies which typically shows a lymphocytic pleocytosis and absence of oligoclonal bands, unlike MS in which upwards of 85% of patients will have elevated CSF oligoclonal bands.
In such cases, it can be helpful to obtain CSF studies which typically shows a lymphocytic pleocytosis and absence of oligoclonal bands, unlike MS in which upwards of 85% of patients will have elevated CSF oligoclonal bands.
9/
Most importantly, though, when there's clinical and imaging suspicion for MOG-IgG-associated disease (MOGAD) or alternatively suspicion for AQP4-IgG-NMOSD, specific laboratory biomarkers (e.g., AQP4-IgG and MOG-IgG) can be incredibly helpful.
Most importantly, though, when there's clinical and imaging suspicion for MOG-IgG-associated disease (MOGAD) or alternatively suspicion for AQP4-IgG-NMOSD, specific laboratory biomarkers (e.g., AQP4-IgG and MOG-IgG) can be incredibly helpful.
10/
I'd recommend obtaining these biomarkers in SERUM, as cell-based assays for these antibody biomarkers are the most reliable and sensitive (more so than CSF) in serum.
I'd recommend obtaining these biomarkers in SERUM, as cell-based assays for these antibody biomarkers are the most reliable and sensitive (more so than CSF) in serum.
11/
Important to keep in mind that MOG-IgG testing frequently has false positives at low titers...
So be a good clinician and follow your gut if the clinical presentation isn't classic for MOGAD.
jamanetwork.com
Important to keep in mind that MOG-IgG testing frequently has false positives at low titers...
So be a good clinician and follow your gut if the clinical presentation isn't classic for MOGAD.
jamanetwork.com
12/
Treatment wise,
Expert consensus recommends prompt initiation of high-dose IV corticosteroids.. and in cases with severe neurologic deficits that persist despite steroids, plasma exchange should be considered.. Alternatively in MOGAD you can consider IVIG too.
Treatment wise,
Expert consensus recommends prompt initiation of high-dose IV corticosteroids.. and in cases with severe neurologic deficits that persist despite steroids, plasma exchange should be considered.. Alternatively in MOGAD you can consider IVIG too.
13/
In our practice, we tend to wait until two clinical attacks before initiating long-term attack-prevention immunotherapy with steroid-sparing agents in MOGAD though prospective randomized trials will be helpful to better guide the chronic treatment approach.
In our practice, we tend to wait until two clinical attacks before initiating long-term attack-prevention immunotherapy with steroid-sparing agents in MOGAD though prospective randomized trials will be helpful to better guide the chronic treatment approach.
14/
Note patients with MOGAD tend to respond better to treatment than those with AQP4-IgG-NMOSD.
Imaging can help identify AQP4-IgG-NMOSD LETM too as this also often shows a ring like pattern of enhancement on gadolinium sequences.
cp.neurology.org
Note patients with MOGAD tend to respond better to treatment than those with AQP4-IgG-NMOSD.
Imaging can help identify AQP4-IgG-NMOSD LETM too as this also often shows a ring like pattern of enhancement on gadolinium sequences.
cp.neurology.org

15/
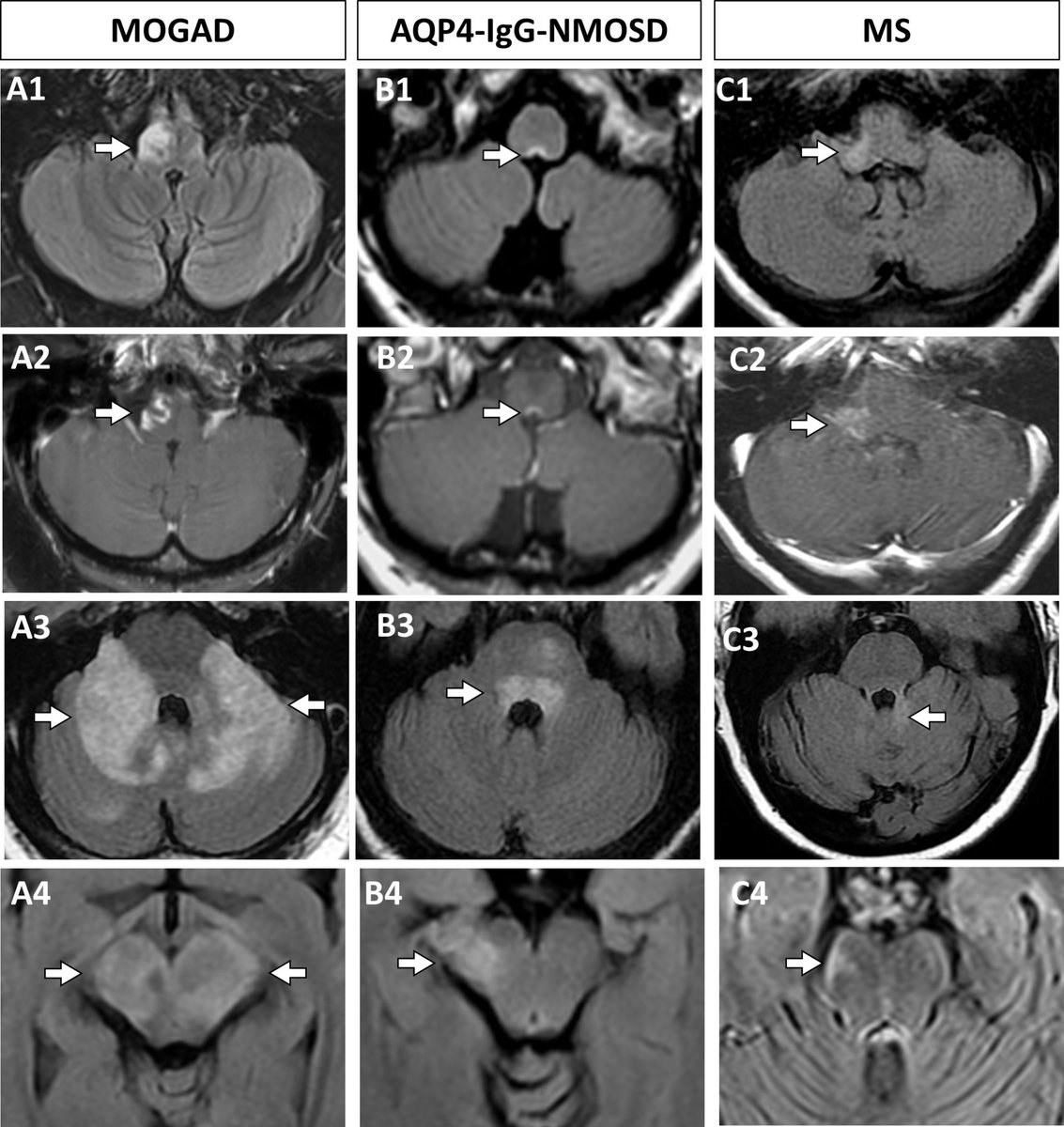
In the posterior fossa, imaging can help distinguish these disorders too.
In the posterior fossa, imaging can help distinguish these disorders too.
16/
@SamanthaBanksMD's study below showed lesions diffusely involving the middle cerebellar peduncle favor MOGAD over AQP4-IgG-NMOSD (which more often affects the area postrema) and MS (where short peripheral lesions are more common).
jnnp.bmj.com
@SamanthaBanksMD's study below showed lesions diffusely involving the middle cerebellar peduncle favor MOGAD over AQP4-IgG-NMOSD (which more often affects the area postrema) and MS (where short peripheral lesions are more common).
jnnp.bmj.com
17/
Final takeaways:
▶️Subacute LETM➡️think inflammatory, like MOGAD or AQP4-NMOSD
▶️Remember H sign for MOGAD and Ring enhancement for AQP4
▶️Serum cell based antibody assays for both of the above is the way to go for dx
▶️tx: Steroids; PLEX/IVIG if severe, persistent deficits
Final takeaways:
▶️Subacute LETM➡️think inflammatory, like MOGAD or AQP4-NMOSD
▶️Remember H sign for MOGAD and Ring enhancement for AQP4
▶️Serum cell based antibody assays for both of the above is the way to go for dx
▶️tx: Steroids; PLEX/IVIG if severe, persistent deficits
18/
As always, hope this was helpful and thanks for joining 🙂
See you next time!
As always, hope this was helpful and thanks for joining 🙂
See you next time!

Loading suggestions...