

@Rajiv_Sinanan @NephroP @katiewiskar @khaycock2 Awesome, now it makes sense. As you say increased total body sodium with decreased total body water.
Now I agree with you. You need natriuresis. Proximal diuretics are more aquaretic than distal. But to maximize natriuresis I forze every nephron segment 1/
Now I agree with you. You need natriuresis. Proximal diuretics are more aquaretic than distal. But to maximize natriuresis I forze every nephron segment 1/
@Rajiv_Sinanan @NephroP @katiewiskar @khaycock2 Acetazolamide, Furosemide, Clorthalidone and Amiloride. This while giving enough free water to correct and acunt for electrolite free water clearance (fron urine lytes). As for the cause of edema WITHOUT congestion there are 3 mechanisms: 2/
@Rajiv_Sinanan @NephroP @katiewiskar @khaycock2 1) There used congestion, edeme developed, then congestion went away. Intersticial edema takes time to distribute.
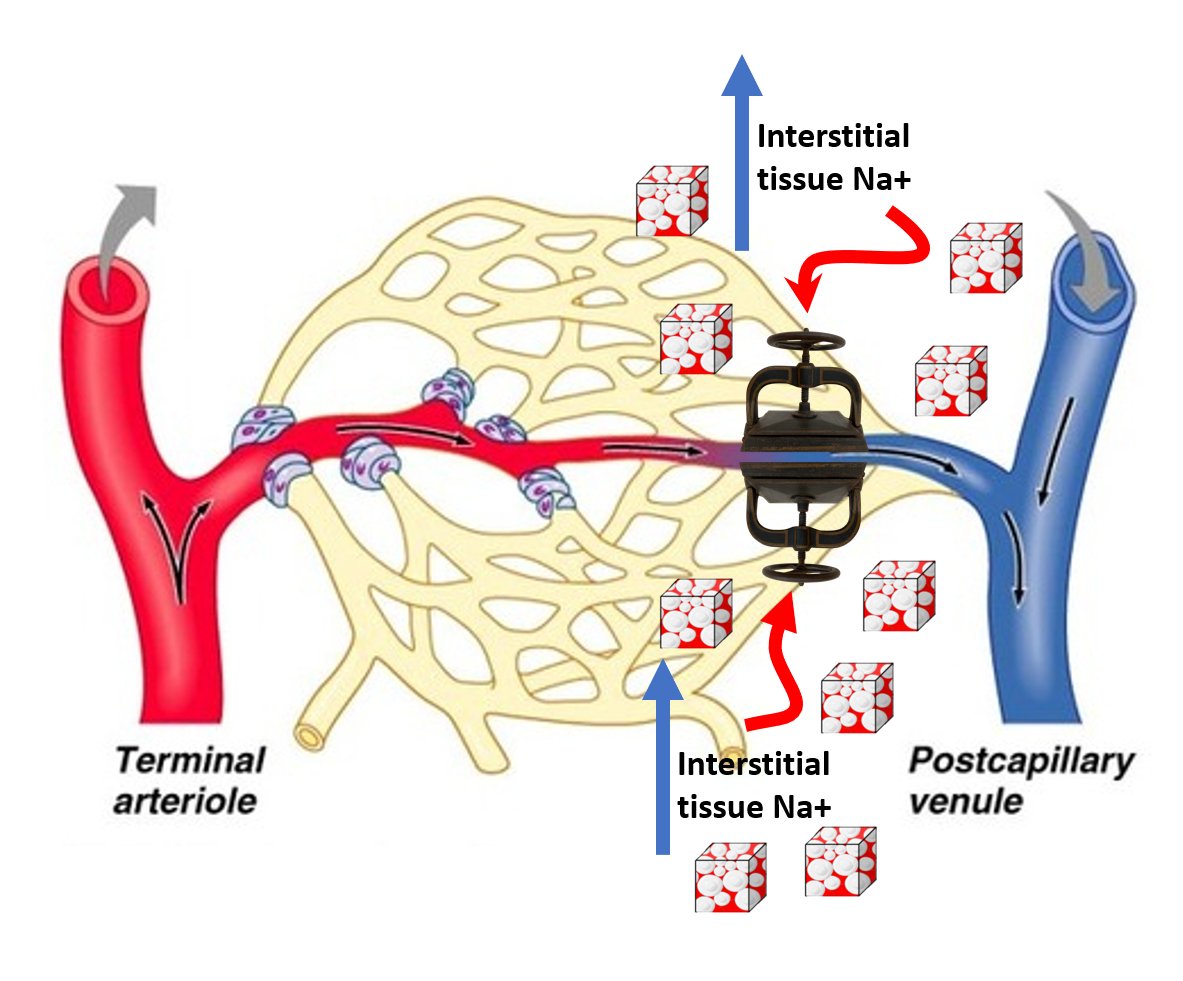
2) Sepsis induced increased permeability and pre-capilary sphincter vasodilation (this last one similar to amlodipine)
3) Increased tissue sodium..... 3/
2) Sepsis induced increased permeability and pre-capilary sphincter vasodilation (this last one similar to amlodipine)
3) Increased tissue sodium..... 3/
@Rajiv_Sinanan @NephroP @katiewiskar @khaycock2 This last one is BANANAS. There is a very good hypothesis suporting the role of interstitial tissue sodium (from excess total body sodium) casing compression of the post-capilary venules. This leads to increased hydraulic capillary pressure even without increased CVP! 4/END
Loading suggestions...