

Some notes on Hepatic encephalopathy taught to me by @DelviseF and @KhushbooSGala
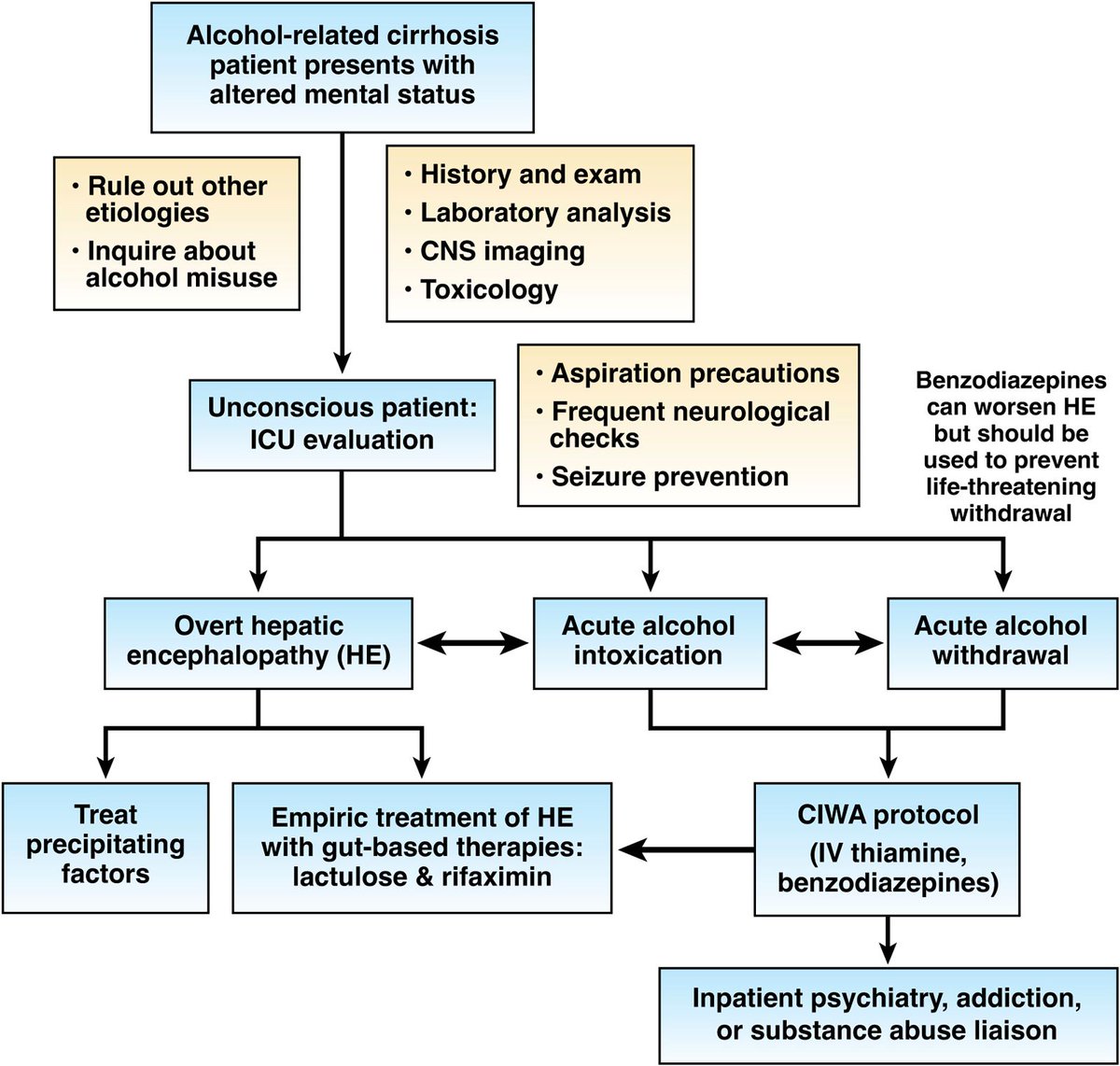
#1: HE is a sedated state. If hyperactive, suspect acute withdrawal (impt because Ativan worsens HE but should be used to prevent life-threatening withdrawals); PMID: PMID: 35598629
#1: HE is a sedated state. If hyperactive, suspect acute withdrawal (impt because Ativan worsens HE but should be used to prevent life-threatening withdrawals); PMID: PMID: 35598629

#2: West Haven Criteria
0: no encephalopathy
1: short attention span, euphoria/depression, sleep-wake disturbance ± asterixis (Ddx: OSA)
2: lethargy/apathy, disorientation, asterixis
3: somnolent but responsive to verbal commands, severe disorientation, no asterixis
4: coma
0: no encephalopathy
1: short attention span, euphoria/depression, sleep-wake disturbance ± asterixis (Ddx: OSA)
2: lethargy/apathy, disorientation, asterixis
3: somnolent but responsive to verbal commands, severe disorientation, no asterixis
4: coma
#3: Diagnosis is clinical; serum ammonia limited role ammonia in cirrhosis-associated HE (may have a role in acute liver failure); brain imaging (e.g., CT, MRI) if diagnosis uncertain or other causes for AMS suspected
#4: Workup for triggers of HE
@DelviseF taught me importance of checking for portosystemic shunting in patients with refractory HE who are compliant with lactulose/rifaximin and have 3-4 soft stools daily.
@DelviseF taught me importance of checking for portosystemic shunting in patients with refractory HE who are compliant with lactulose/rifaximin and have 3-4 soft stools daily.
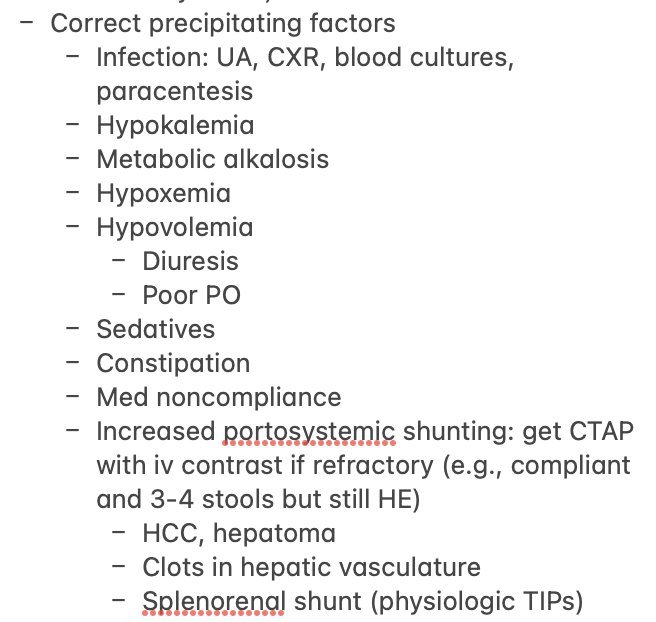
#5. Management of triggers
- Lactulose titrated to 3-4 soft stools daily
- Rifaximin if condition does not improve within 48H or 2nd episode of HE
- Correct hypokalemia, metabolic alkalosis, zinc deficiency
- Reduce intracranial pressure (especially in ALF-HE)
- Correct shunts
- Lactulose titrated to 3-4 soft stools daily
- Rifaximin if condition does not improve within 48H or 2nd episode of HE
- Correct hypokalemia, metabolic alkalosis, zinc deficiency
- Reduce intracranial pressure (especially in ALF-HE)
- Correct shunts
#6. Apparently PEG may be effective as well
Meta-analysis of 7 RCT comparing PEG versus lactulose shows more rapid HE resolution during first 24 hours and shortened length of stay in patients who received PEG.
Would love input from experts on whether this changes practice
Meta-analysis of 7 RCT comparing PEG versus lactulose shows more rapid HE resolution during first 24 hours and shortened length of stay in patients who received PEG.
Would love input from experts on whether this changes practice
Loading suggestions...