

🧵👇
70 y F, affected by GPA (granulomatosis with poliangiitis called Wegener's), referred to our centre for SOB, swelling lower limb and plethoric IVC.
Are u thinking Constrictive Pericarditis ⚡️? Let's try to confirm this diagnosis step by step #echofirst @AJamilTajik @jaekoh2
70 y F, affected by GPA (granulomatosis with poliangiitis called Wegener's), referred to our centre for SOB, swelling lower limb and plethoric IVC.
Are u thinking Constrictive Pericarditis ⚡️? Let's try to confirm this diagnosis step by step #echofirst @AJamilTajik @jaekoh2
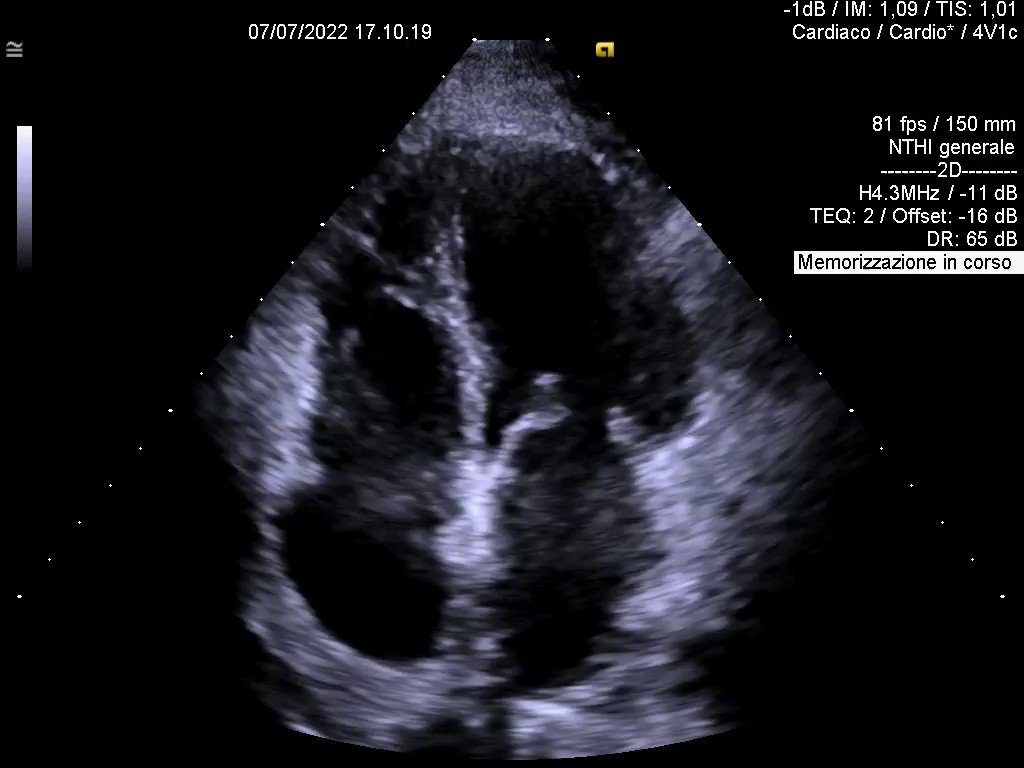
1⃣ SEPTAL BOUNCE
Paradoxical bouncing motion of IVS in early diastole, at the beginning directed towards LV and then away from LV ➡️ Sign of increased ventricular interdipendence
Paradoxical bouncing motion of IVS in early diastole, at the beginning directed towards LV and then away from LV ➡️ Sign of increased ventricular interdipendence

2⃣ E/A variation at the level of MV inflow.
Respiratory variation of peak E wave velocity should be at least >15%.
Inspiratory decrease and expiratory increase of E wave vel. (not so prominent here)
Respiratory variation of peak E wave velocity should be at least >15%.
Inspiratory decrease and expiratory increase of E wave vel. (not so prominent here)

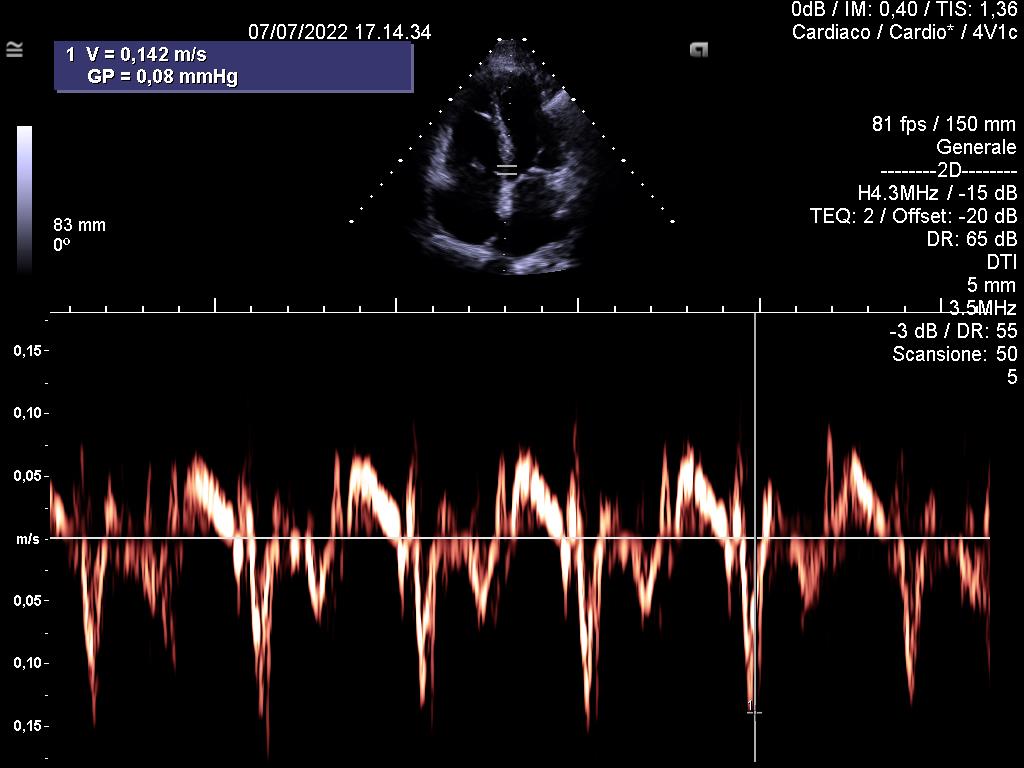
3⃣ ANNULUS REVERSUS
Increased early relaxation velocity (e'), with medial velocity greater than lateral
Increased early relaxation velocity (e'), with medial velocity greater than lateral
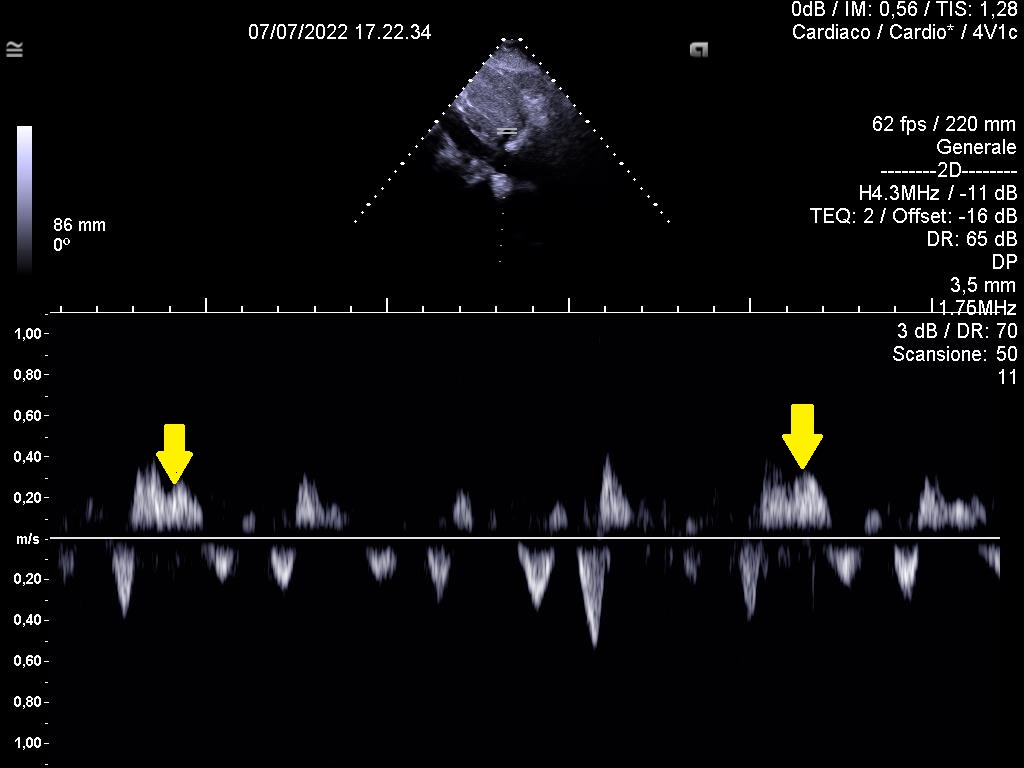
4⃣ DIASTOLIC FLOW REVERSAL IN EXPIRATION
Always look for this sign with PW whitin hepatic vein.
PS (i apologize for EKG and respirometric traces, but i don 't why in my original clips i can see them and here not)
Always look for this sign with PW whitin hepatic vein.
PS (i apologize for EKG and respirometric traces, but i don 't why in my original clips i can see them and here not)
5⃣ SUBCOSTAL VIEW (don't forget it)
Used to identify tethering of the right ventricular free wall at its interface with the liver and also to measure maximum pericardium thickness
Used to identify tethering of the right ventricular free wall at its interface with the liver and also to measure maximum pericardium thickness

6⃣ CT scan.
One of the most important issue to don't miss constrictive pericarditis is that calcium is NOT a necessary condition
One of the most important issue to don't miss constrictive pericarditis is that calcium is NOT a necessary condition

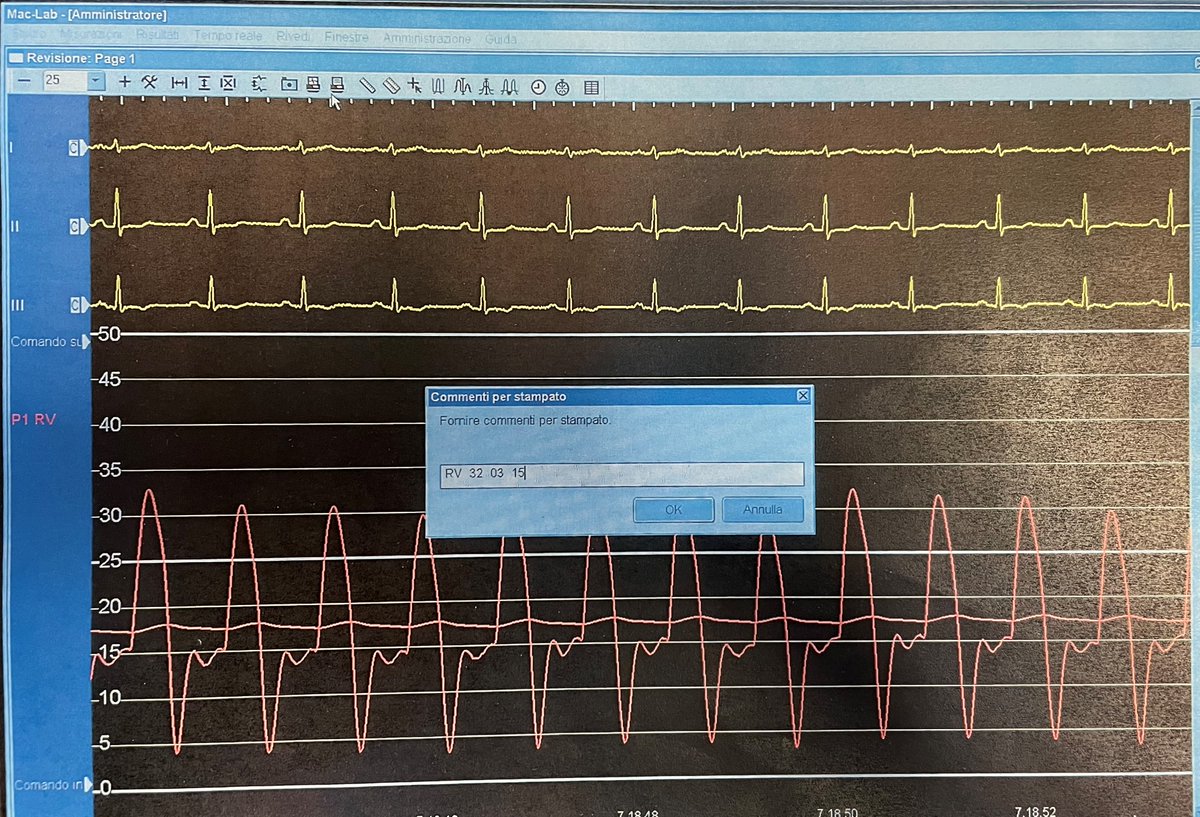
7⃣ ‘Dip & plateau pattern’ or ‘SQUARE ROOT SIGN"
Cath Lab ➡️Early diastolic filling of the ventricles is unimpeded and abnormally rapid, but late diastolic filling is abbreviated and halts abruptly when total cardiac volume expands to the volume limit set by the stiff pericardium
Cath Lab ➡️Early diastolic filling of the ventricles is unimpeded and abnormally rapid, but late diastolic filling is abbreviated and halts abruptly when total cardiac volume expands to the volume limit set by the stiff pericardium
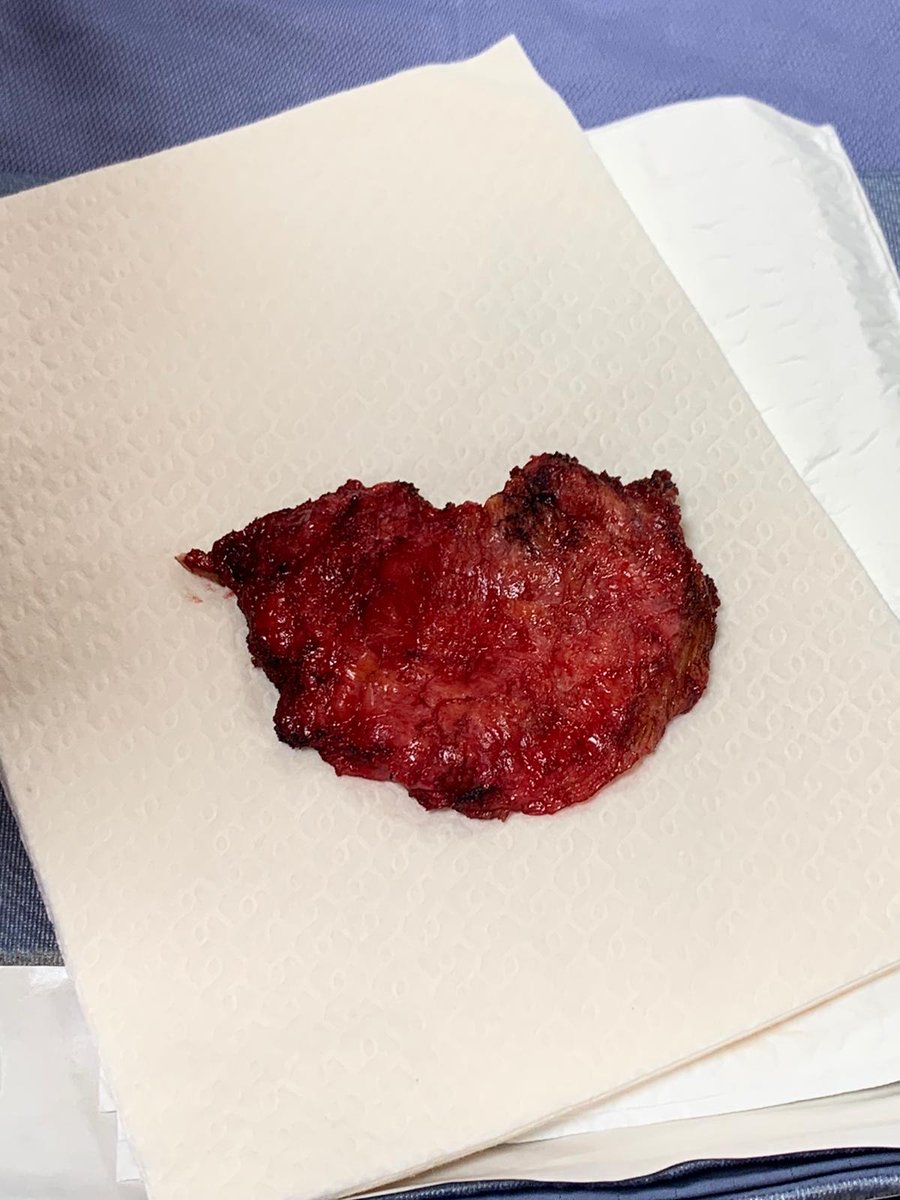
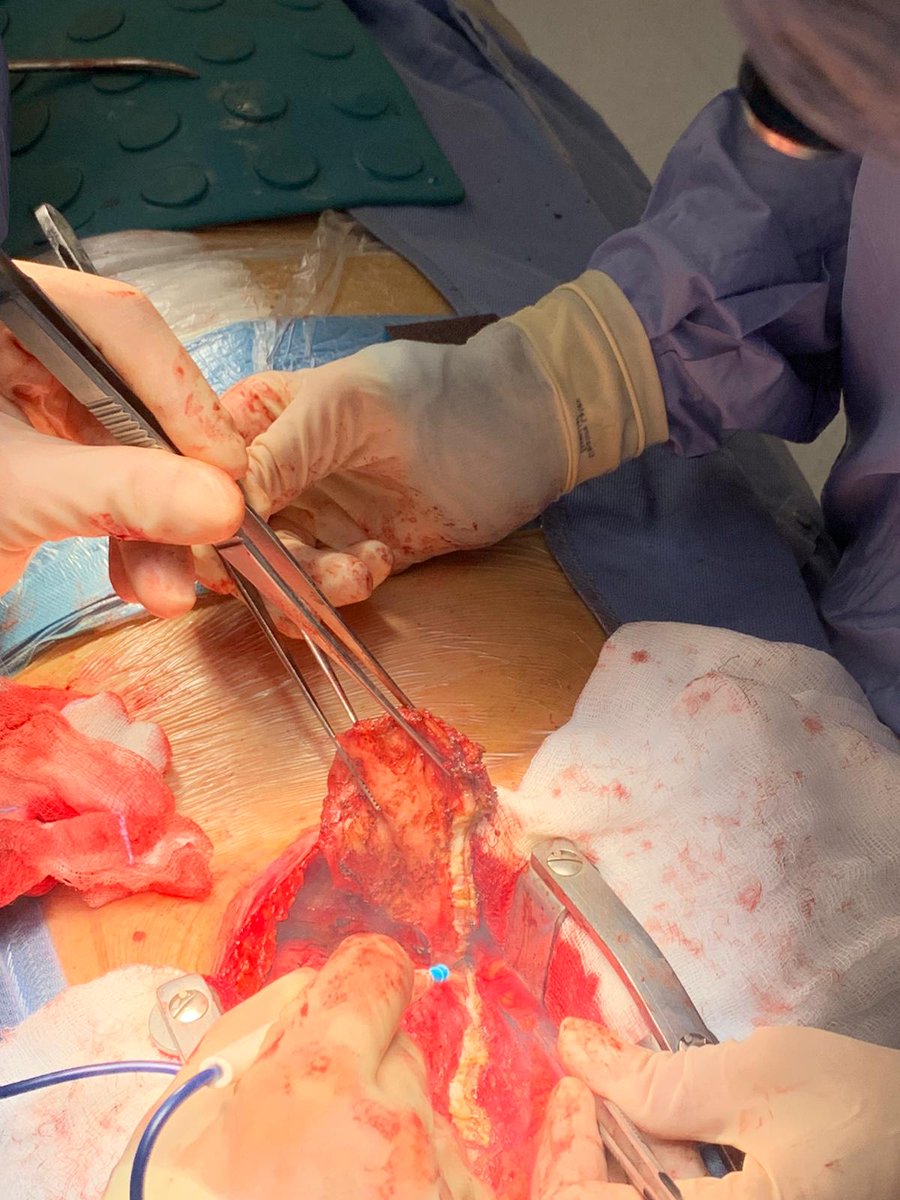
8⃣ PERICARDIECTOMY and surgical findings ⚡️
9⃣
Last video with pericardium in my hands.
Incredible stiffness! It seems that the heart was imprisoned in a cage
Last video with pericardium in my hands.
Incredible stiffness! It seems that the heart was imprisoned in a cage

Loading suggestions...