

#NeuroPostItPearls 24
1/
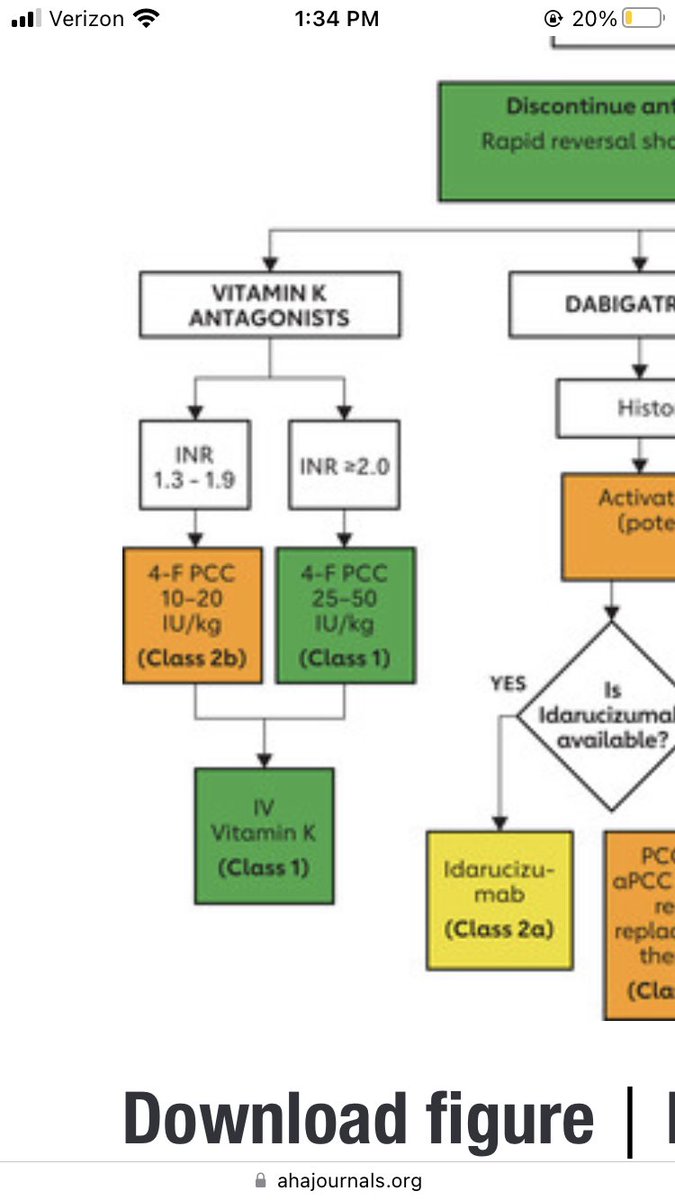
The @StrokeAHA_ASA guidelines for ICH recommend INR-based dosing for reversal of vitamin K.
This requires waiting to know the INR though.
Unless you really doubt the patient was taking the med, draw the INR, and give a standardized dose up front
1/
The @StrokeAHA_ASA guidelines for ICH recommend INR-based dosing for reversal of vitamin K.
This requires waiting to know the INR though.
Unless you really doubt the patient was taking the med, draw the INR, and give a standardized dose up front
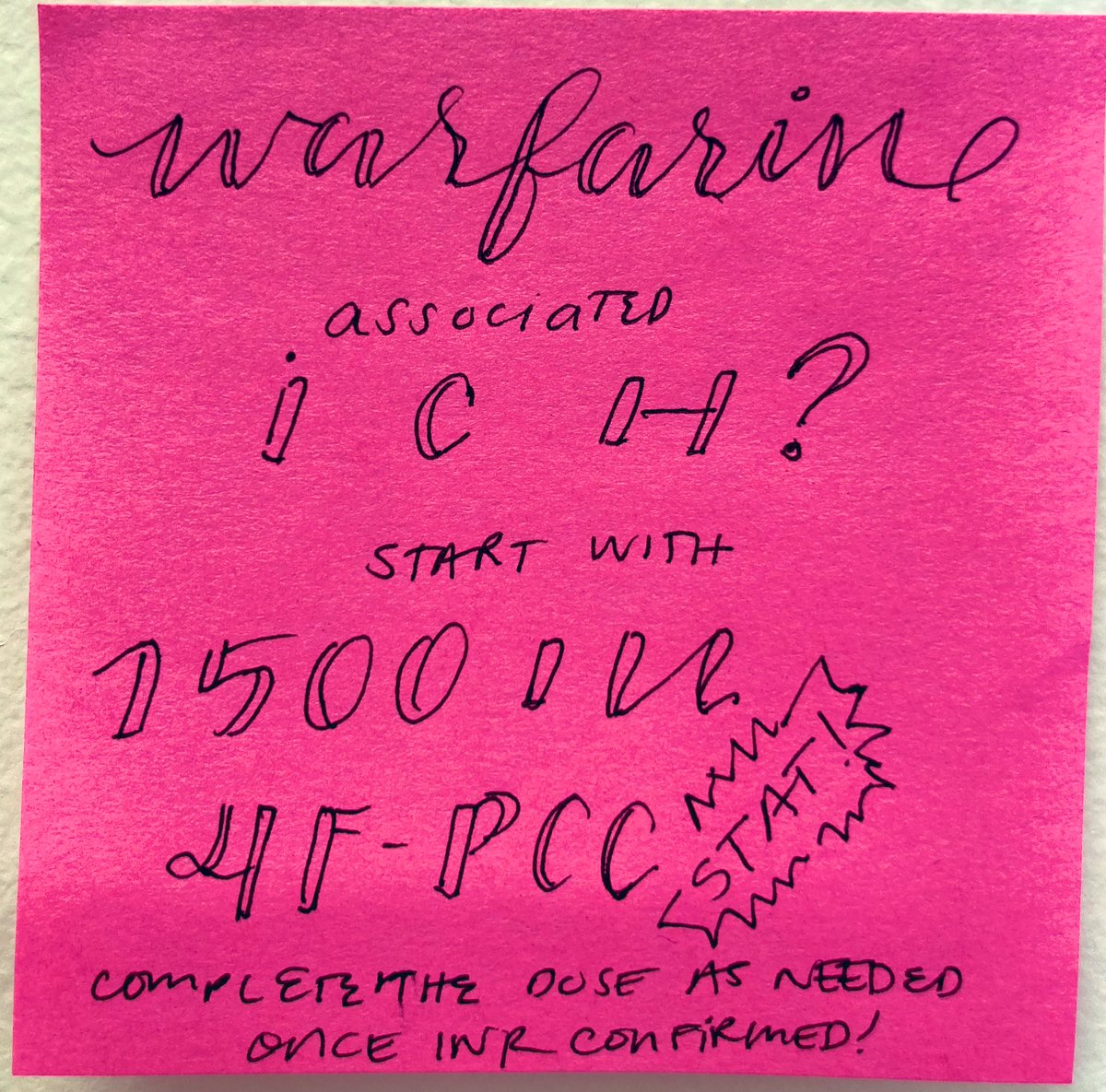
2/
#Timeisbrain and reversing quickly is so important.
Even if the INR comes back as 1.3, the 1500 IU load is within (class 2b) supported 10-20 IU/kg range for most normal weight patients.
#Timeisbrain and reversing quickly is so important.
Even if the INR comes back as 1.3, the 1500 IU load is within (class 2b) supported 10-20 IU/kg range for most normal weight patients.
3/
If the INR comes back as 3, then your total dose may end up being more like ~3000 IU
they’d need a second 1500 IU, but great that they’ve already gotten some of the reversal!
The only draw back is that you must remember to follow up the INR and finish the treatment!
If the INR comes back as 3, then your total dose may end up being more like ~3000 IU
they’d need a second 1500 IU, but great that they’ve already gotten some of the reversal!
The only draw back is that you must remember to follow up the INR and finish the treatment!
4/
There is some evidence that fixed dose strategies are faster (pubmed.ncbi.nlm.nih.gov)
And consistent quick action 👍!
But, giving a follow up dose adheres to the weight-based dosed per the guideline, best of both strategies!
There is some evidence that fixed dose strategies are faster (pubmed.ncbi.nlm.nih.gov)
And consistent quick action 👍!
But, giving a follow up dose adheres to the weight-based dosed per the guideline, best of both strategies!
Loading suggestions...