

1/12
A 58 y/o man presents with dyspnea.
We are struck by the appearance of his hands.
A 58 y/o man presents with dyspnea.
We are struck by the appearance of his hands.

2/12
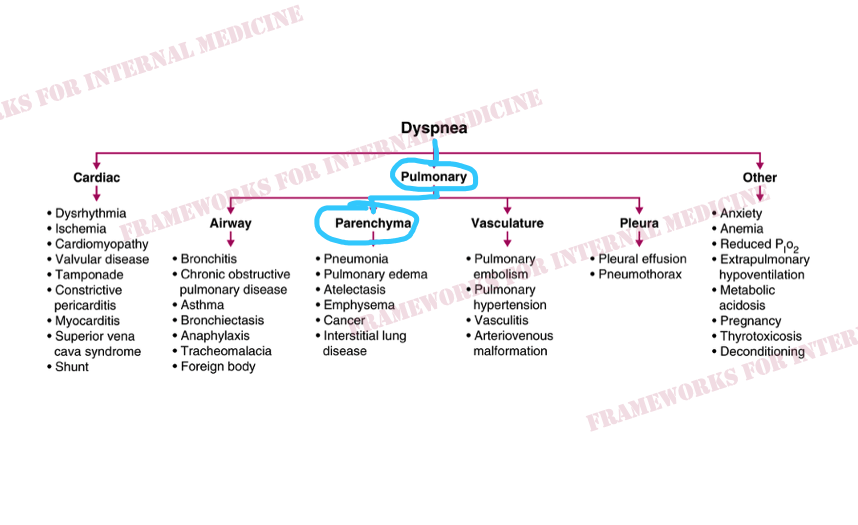
We ignore the hands for a moment and recall that most cases of dyspnea are primarily related to either the heart or the lungs (or both).
We ignore the hands for a moment and recall that most cases of dyspnea are primarily related to either the heart or the lungs (or both).

3/12
So what does our patient’s heart sound like?
So what does our patient’s heart sound like?

4/12
The heart sounds are abnormal. But the P2>A2 means the heart might be able to blame the lungs in this case.
Let’s listen to the lungs.
The heart sounds are abnormal. But the P2>A2 means the heart might be able to blame the lungs in this case.
Let’s listen to the lungs.

5/12
The presence of rales indicate a lung problem. The late, Velcro-like nature of the rales localizes the issue to the alveoli/parenchyma.
The presence of rales indicate a lung problem. The late, Velcro-like nature of the rales localizes the issue to the alveoli/parenchyma.
6/12
Listening higher up on the chest we hear this sound. What is it?
Listening higher up on the chest we hear this sound. What is it?

7/12
The inspiratory squawk is an unusual lung sound typically heard in the setting of interstitial lung disease.
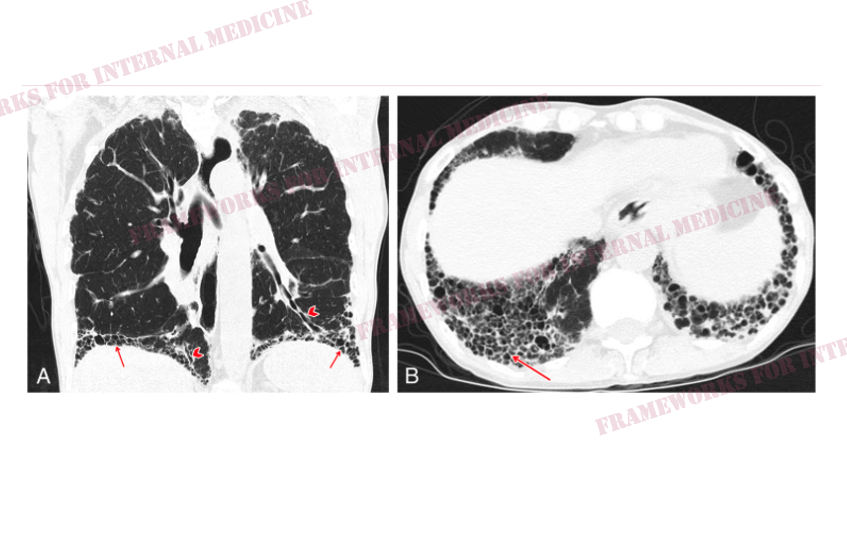
High res CT demonstrates lower lobe–predominant subpleural reticular opacities and honeycombing (arrows), traction bronchiectasis (arrowheads), and no ground glass
The inspiratory squawk is an unusual lung sound typically heard in the setting of interstitial lung disease.
High res CT demonstrates lower lobe–predominant subpleural reticular opacities and honeycombing (arrows), traction bronchiectasis (arrowheads), and no ground glass
8/12
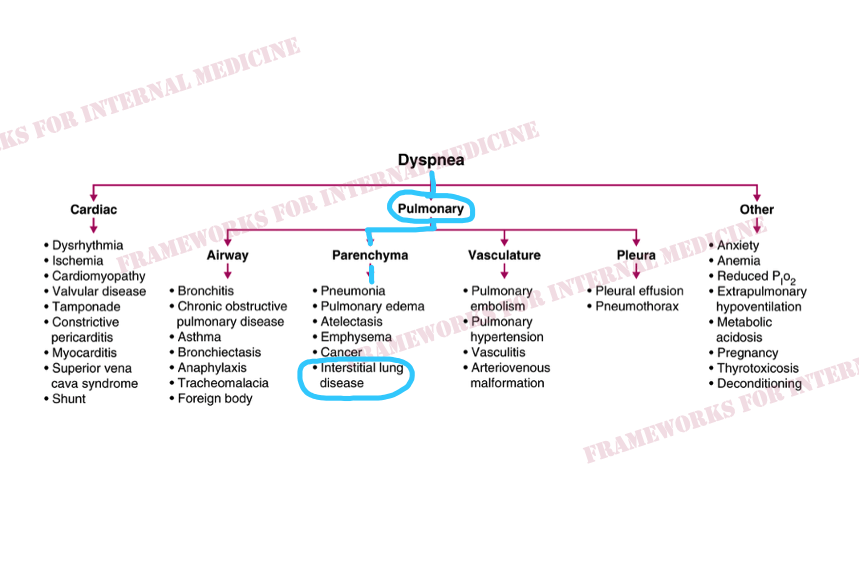
We have made a diagnosis of interstitial lung disease.
We have made a diagnosis of interstitial lung disease.
9/12
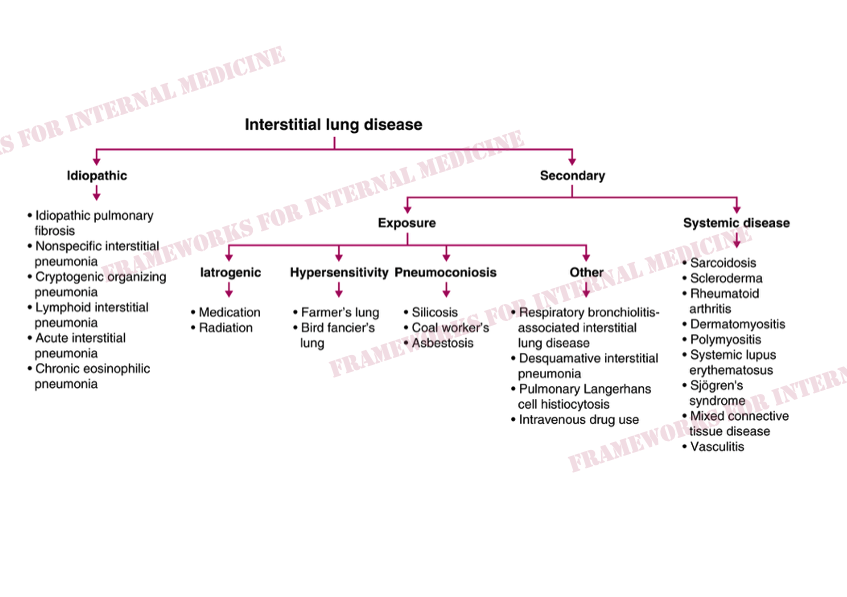
But like many diagnoses in medicine, we can’t just stop at “ILD”. What is the cause of ILD? For this we refer to another framework.
But like many diagnoses in medicine, we can’t just stop at “ILD”. What is the cause of ILD? For this we refer to another framework.
10/12
We return to the patient’s hands. We see sclerodactyly, characterized by skin thickening and hardening, giving the skin a shiny appearance and leading to curling of the fingers with loss of mobility. There is also digital skin pitting and poorly healing ulcerations.
We return to the patient’s hands. We see sclerodactyly, characterized by skin thickening and hardening, giving the skin a shiny appearance and leading to curling of the fingers with loss of mobility. There is also digital skin pitting and poorly healing ulcerations.
11/12
Our pt has scleroderma.
The pattern on HRCT imaging is UIP, a common presentation of ILD associated with scleroderma.
Overall, prognosis is poor. Pts with NSIP pattern tend to have better outcomes (median survival of 15 years) vs those with a UIP pattern (only 3 years).
Our pt has scleroderma.
The pattern on HRCT imaging is UIP, a common presentation of ILD associated with scleroderma.
Overall, prognosis is poor. Pts with NSIP pattern tend to have better outcomes (median survival of 15 years) vs those with a UIP pattern (only 3 years).

12/12
First we diagnosed interstitial lung disease, then we diagnosed underlying scleroderma. All with our eyes, ears, and a little help from hypothesis-driven testing.
For more frameworks: amazon.com
First we diagnosed interstitial lung disease, then we diagnosed underlying scleroderma. All with our eyes, ears, and a little help from hypothesis-driven testing.
For more frameworks: amazon.com

Loading suggestions...