

I think one of the hardest skills in med school, residency, and fellowship is presenting new patients to the attending. I create one notecard/patient and will walk you through my approach for Cardiology Consults.
*This is a made up patient*
#MedTwitter #Cardiotwitter
#MedEd
*This is a made up patient*
#MedTwitter #Cardiotwitter
#MedEd

1) Reason for the consult:
- In cardiology, common reasons include: atrial fibrillation, bradycardia, hypertensive urgency, heart failure exacerbation, etc. This allows the attending to focus his/her attention on what the clinical question is being asked as a consultant.
- In cardiology, common reasons include: atrial fibrillation, bradycardia, hypertensive urgency, heart failure exacerbation, etc. This allows the attending to focus his/her attention on what the clinical question is being asked as a consultant.
2) Relevant past medical history:
- Don't need to list every past medical problem, rather focus on those related to the diagnosis and clinical picture. This could include HTN, DM, HLD, COPD, CKD, AF, HFrEF.
- If not relevant, can avoid mentioning to condense presentation.
- Don't need to list every past medical problem, rather focus on those related to the diagnosis and clinical picture. This could include HTN, DM, HLD, COPD, CKD, AF, HFrEF.
- If not relevant, can avoid mentioning to condense presentation.
3) Chief Complaint:
- This is an art and requires telling the patient's story.
- For example, for chest pain: should include location, intensity, quality, duration, alleviating/precipitating factors, associated symptoms.
- Keep it brief, focused, and descriptive.
- This is an art and requires telling the patient's story.
- For example, for chest pain: should include location, intensity, quality, duration, alleviating/precipitating factors, associated symptoms.
- Keep it brief, focused, and descriptive.
4) ER Vitals and Labs:
- Present the vitals in the ER with ranges (for HR and BP), and O2 saturation (RA or NC).
- Labs (relevant): electrolytes, Creatinine (and baseline), troponin trends & BNP (compared to prior admissions), UDS, Hemoglobin & Platelets) (baseline), LDL, A1c
- Present the vitals in the ER with ranges (for HR and BP), and O2 saturation (RA or NC).
- Labs (relevant): electrolytes, Creatinine (and baseline), troponin trends & BNP (compared to prior admissions), UDS, Hemoglobin & Platelets) (baseline), LDL, A1c
5) ER Imaging:
- EKG (provide interpretation) and print-out if not by a computer (follow a methodical approach with rate, rhythm, axis, intervals, ischemic changes, etc). Can compare to prior if available
- CXR: signs of volume overload, effusions
- CTA: Evaluation for PE
- EKG (provide interpretation) and print-out if not by a computer (follow a methodical approach with rate, rhythm, axis, intervals, ischemic changes, etc). Can compare to prior if available
- CXR: signs of volume overload, effusions
- CTA: Evaluation for PE
6) ER Course:
- Mention the work-up in the ER, such as medications provided
- Common ones include ASA: 324 mg, Heparin gtt, IV Lasix, Sublingual Nitroglycerin
- Mention the work-up in the ER, such as medications provided
- Common ones include ASA: 324 mg, Heparin gtt, IV Lasix, Sublingual Nitroglycerin
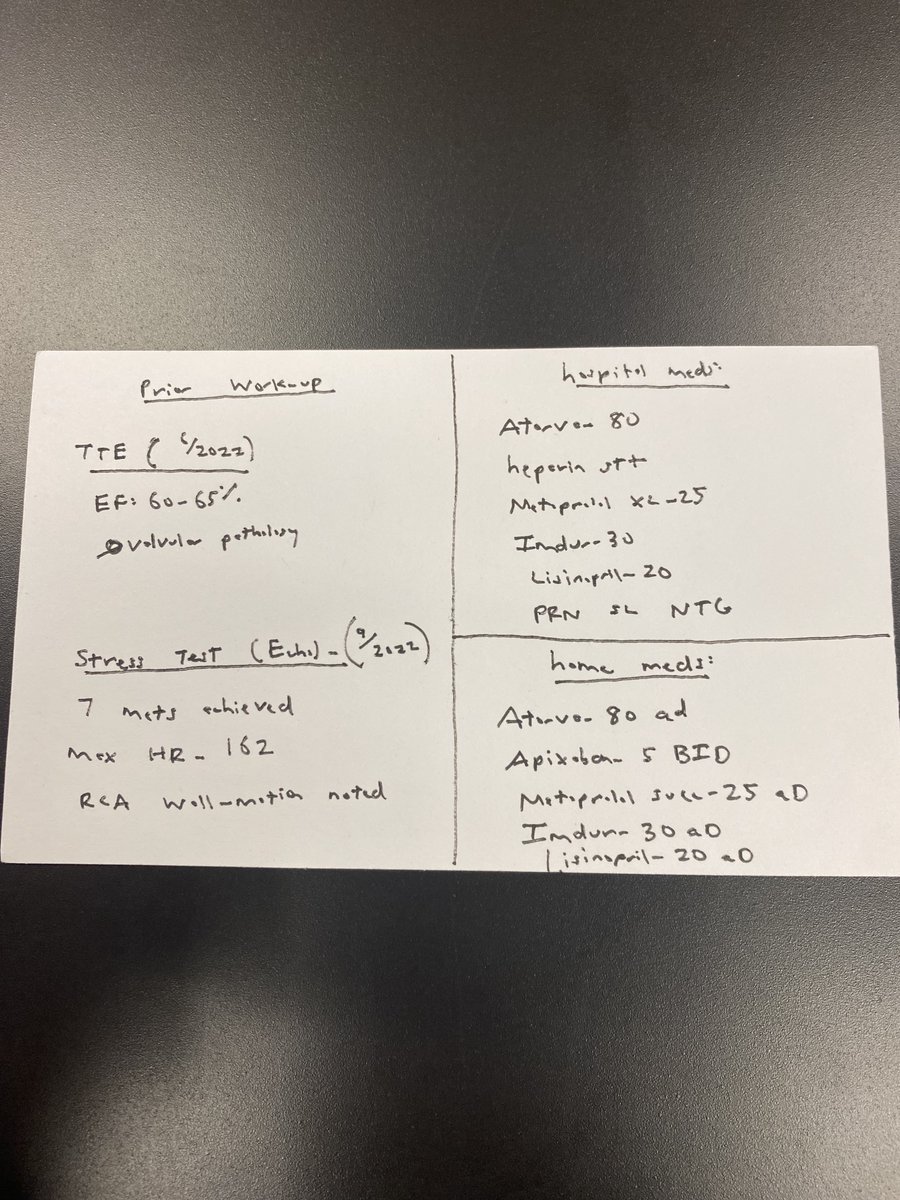
7) Prior Work-Up
- This can include prior TTE (with ejection fraction, diastolic dysfunction, valvular pathology), LHC (year and location of PCI), Stress Testing (Dobutamine, Lexiscan, Exercise Testing)
- This provides more information in context of current presentation
- This can include prior TTE (with ejection fraction, diastolic dysfunction, valvular pathology), LHC (year and location of PCI), Stress Testing (Dobutamine, Lexiscan, Exercise Testing)
- This provides more information in context of current presentation
8) Home Medications:
- As a cardiology fellow, I focus on the cardiac and diabetes medications.
- If possible, can verify with patients if they are taking medications
- Can discuss with pharmacy team (if available) for information about filling patterns
- As a cardiology fellow, I focus on the cardiac and diabetes medications.
- If possible, can verify with patients if they are taking medications
- Can discuss with pharmacy team (if available) for information about filling patterns
9) Hospital Medications:
- Compare the active medication list to the home medication list
- Question: Is there a reason some medications are being held (ACE for AKI, BB for cardiogenic shock, DOAC for bleeding)?
- Can make recommendations to start when clinically indicated
- Compare the active medication list to the home medication list
- Question: Is there a reason some medications are being held (ACE for AKI, BB for cardiogenic shock, DOAC for bleeding)?
- Can make recommendations to start when clinically indicated
10) Overnight Updates:
- Present vitals (ranges) from overnight
- Subjective and objective (physical exam findings)
- Mention lab trends compared from previous day
- I/O if being diuresed (net output, look for contraction alkalosis)
- Present vitals (ranges) from overnight
- Subjective and objective (physical exam findings)
- Mention lab trends compared from previous day
- I/O if being diuresed (net output, look for contraction alkalosis)
11) Assessment & Plan
- Offer clinical diagnosis based on supporting evidence and a plan of action
- It is okay to be wrong, but try to justify your thought process and clinical decision making
- Offer clinical diagnosis based on supporting evidence and a plan of action
- It is okay to be wrong, but try to justify your thought process and clinical decision making
Take-Aways:
- As a med student, I didn't have a standardized approach and felt over-whelmed.
- I learned that a notecard approach condenses all the information in one location
- Easy to make modifications to the hospital meds portion with hospital course.
- As a med student, I didn't have a standardized approach and felt over-whelmed.
- I learned that a notecard approach condenses all the information in one location
- Easy to make modifications to the hospital meds portion with hospital course.
Take-Aways:
- It takes time (years) to master presentations skills
- Often times, attending physicians are starting fresh and your presentation will guide clinical decision-making
- Can modify for other specialties (especially internal medicine)
- Ask for seniors for feedback!
- It takes time (years) to master presentations skills
- Often times, attending physicians are starting fresh and your presentation will guide clinical decision-making
- Can modify for other specialties (especially internal medicine)
- Ask for seniors for feedback!
Loading suggestions...