

1/ #CHEST2022 was fantastic! Here are some of my big take away points from this week’s sessions. @accpchest @VCU_PCCM @crit_caring_MD @lkbrath @DanckersMD @aggie07girl @DrMeganConroy @subanichandra

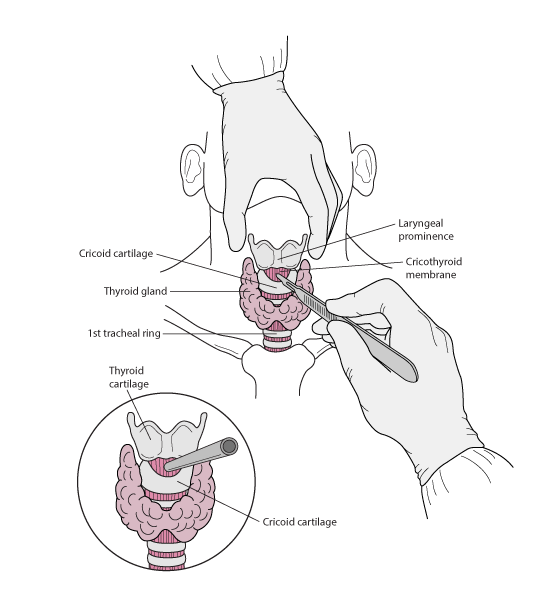
2/ From the CHEST Fellow’s Course, if you have a difficult airway and are asking for a supraglottic airway you should also be calling for help in case you need a surgical airway.

3/Also from the CHEST Fellow’s Course: In the setting of ARDS, be sure to have completed the standards of care in ARDS including proning and neuromuscular blockade before pursuing VV ECMO.

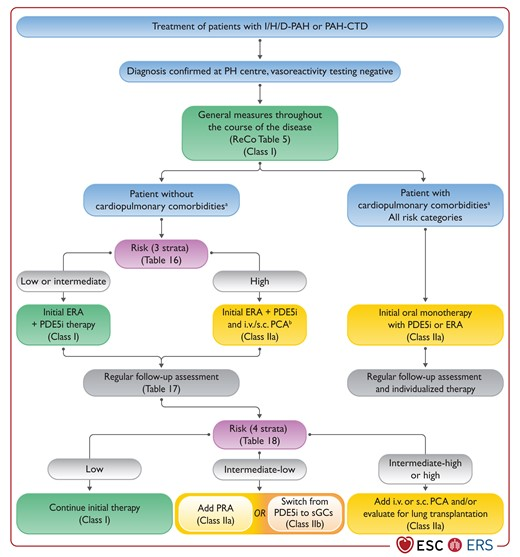
4/ In severe PAH, initial triple therapy can be a reasonable approach given PAH treatments are more efficacious early. Additionally, there have been retrospective studies showing afterload reduction and survival benefits with triple therapy.
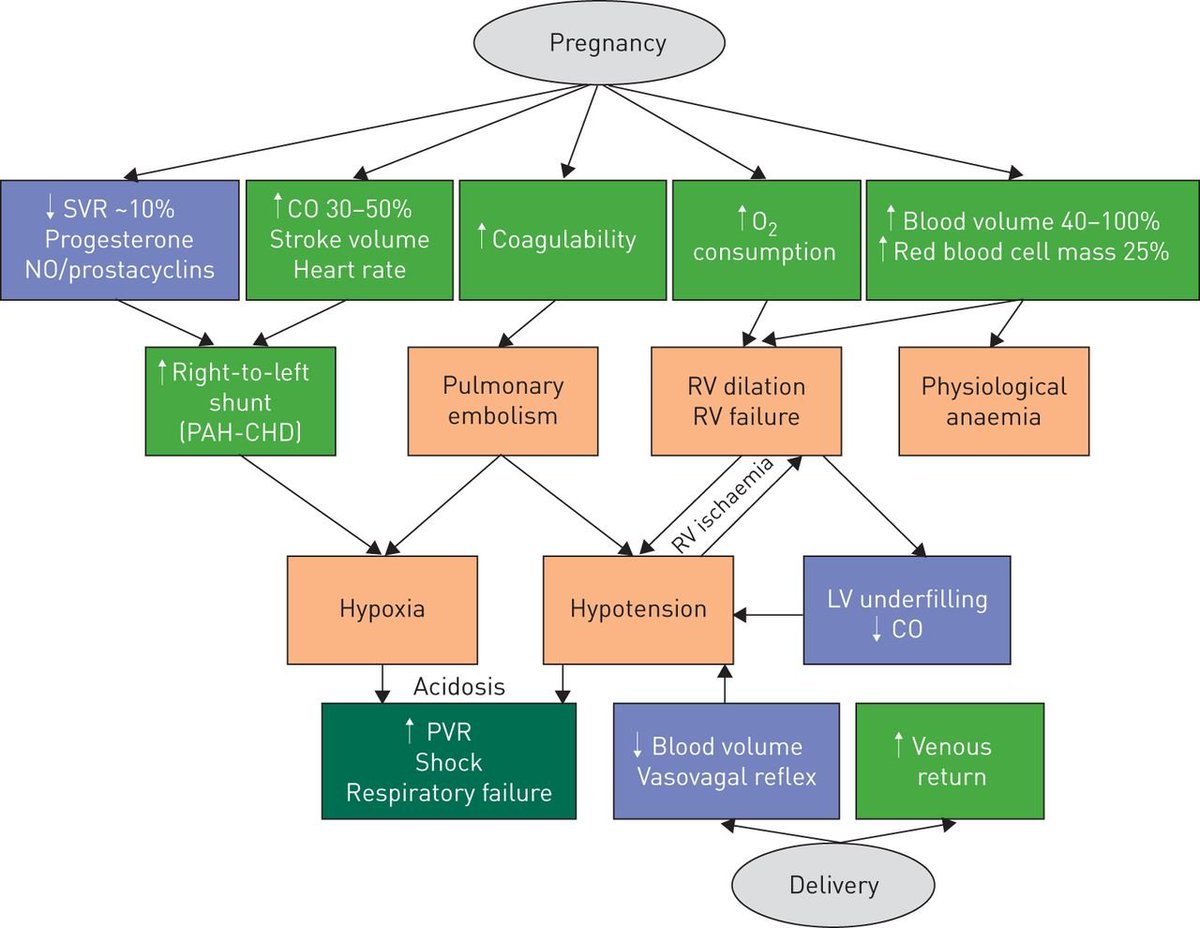
5/ Pregnancy in PAH patients should be avoided. Pregnancy in PH requires a multidisciplinary approach. Studies suggest optimal timing for delivery is ~34 weeks gestation via C-section. The first 72 hours following delivery can be the most tenuous from a hemodynamic standpoint.
6/ There remains a lot of controversy regarding the management of intermediate risk pulmonary embolus patients. Should we be doing TPA or thrombectomy in these patients?
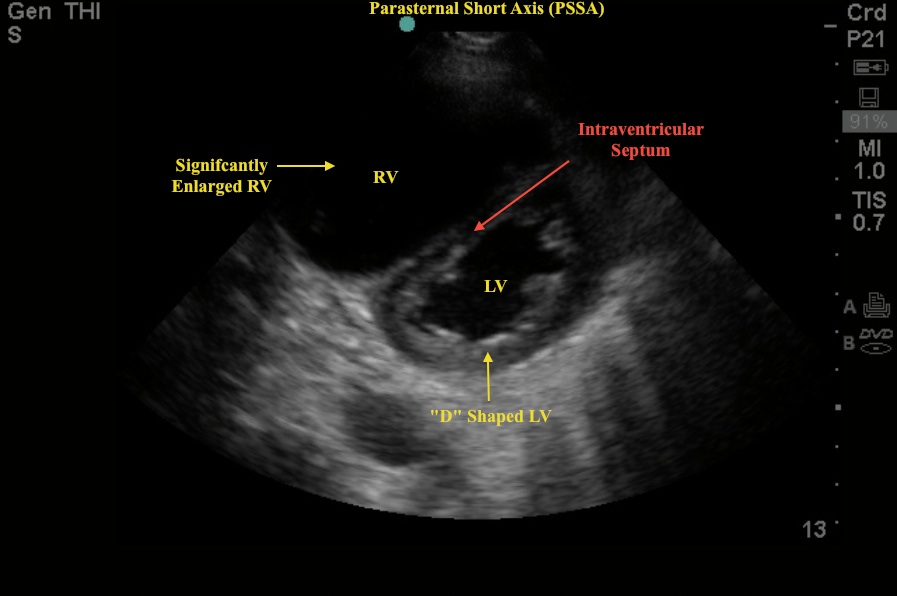
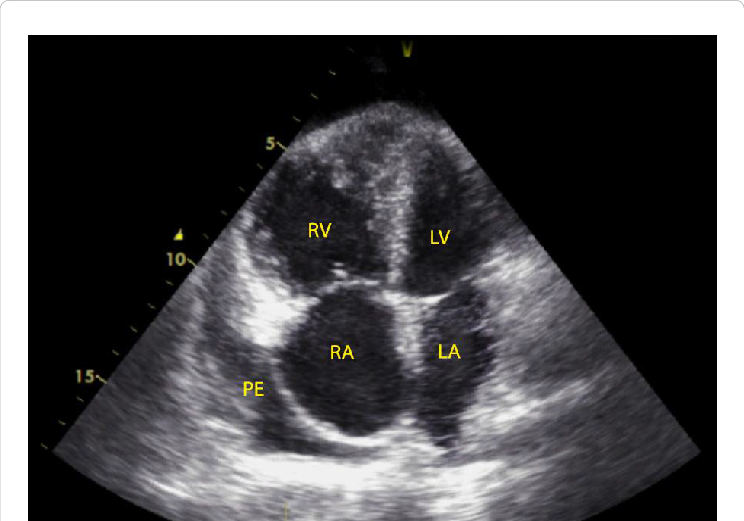
7/ TTE provides non-invasive assessment of right heart structure and function in PAH. Findings of the 3 Ss can guide differential diagnosis and assessment of PH severity.
1⃣Size – RV dilation/ RV shape
2⃣Squeeze – RV contraction
3⃣Smush – Interventricular septal flattening
1⃣Size – RV dilation/ RV shape
2⃣Squeeze – RV contraction
3⃣Smush – Interventricular septal flattening
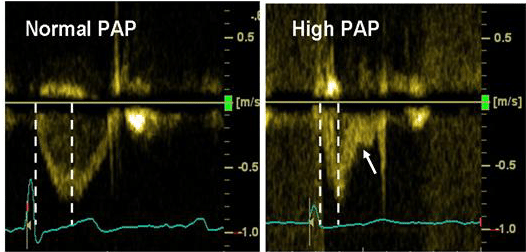
8/ Evidence suggests that in nearly 50% of cases PASP by doppler differs by >10 mmHg from RHC findings. Doppler in the RV outflow tract can help differentiate between PAH and group 2 PH as a mid-systolic notch on doppler indicates high PVR and poor PA compliance.
9/ In PAH, it is the not pressure overload that causes septal flattening but instead it is the combination of high PVR and low compliance of the pulmonary vasculature.
10/ The PHAR is attempting to address some of the healthcare disparities seen in prior pulmonary hypertension registries. Additionally, we need to do a better job as a healthcare community in ensuring that all patient populations are represented in clinical trials.
11/ There is an overestimation of arterial oxygenation saturation levels by pulse oximetry in patients of racial and ethnic minorities. It is important for healthcare providers to recognize this issue and to advocate for a solution. jamanetwork.com
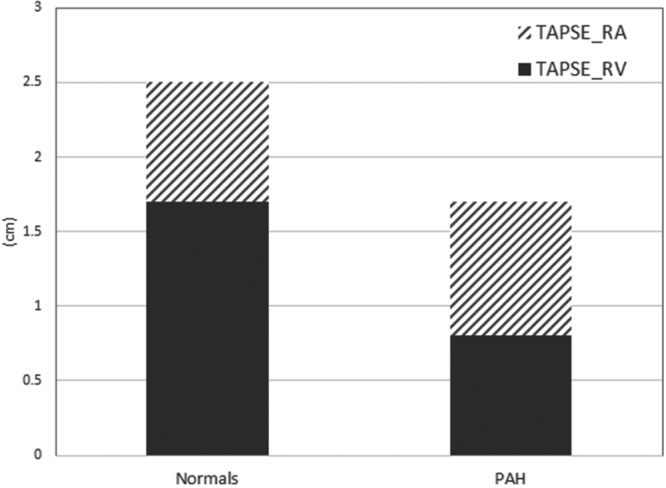
12/ The atrial kick in a normal RV contributes to 20% of RV function; however, in PH the atrial kick contributes up to approximately 50% of RV function. This demonstrates the importance of rhythm control in the setting of an SVT. Avoid beta blockers and CCB in PH patients.

13/ Principles in the management of RV failure include the following:
1⃣Optimize Preload – DIURESE!
2⃣Reduce Afterload
3⃣Optimize Contractility
1⃣Optimize Preload – DIURESE!
2⃣Reduce Afterload
3⃣Optimize Contractility
14/ Other good practice measures in management of RV failure:
1⃣Target SaO2 > 95% to avoid hypoxic pulmonary vasoconstriction
2⃣Avoid acidosis
3⃣Avoid dynamic hyperinflation in MV
4⃣Try to keep PEEP <10
5⃣May benefit from higher hemoglobin goal >10 g/dL
1⃣Target SaO2 > 95% to avoid hypoxic pulmonary vasoconstriction
2⃣Avoid acidosis
3⃣Avoid dynamic hyperinflation in MV
4⃣Try to keep PEEP <10
5⃣May benefit from higher hemoglobin goal >10 g/dL
15/ That's it I promise.

Loading suggestions...