

😵💫 Approach to Dizziness! 😵💫
4 big buckets:
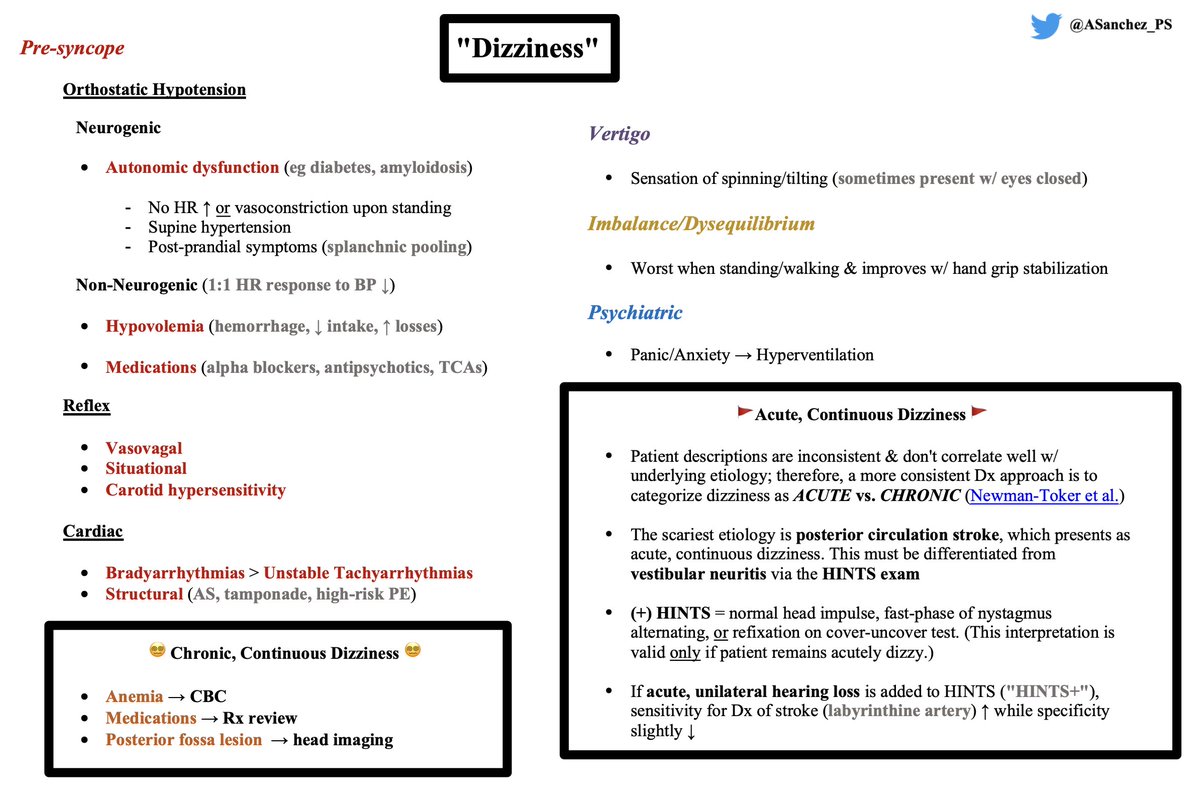
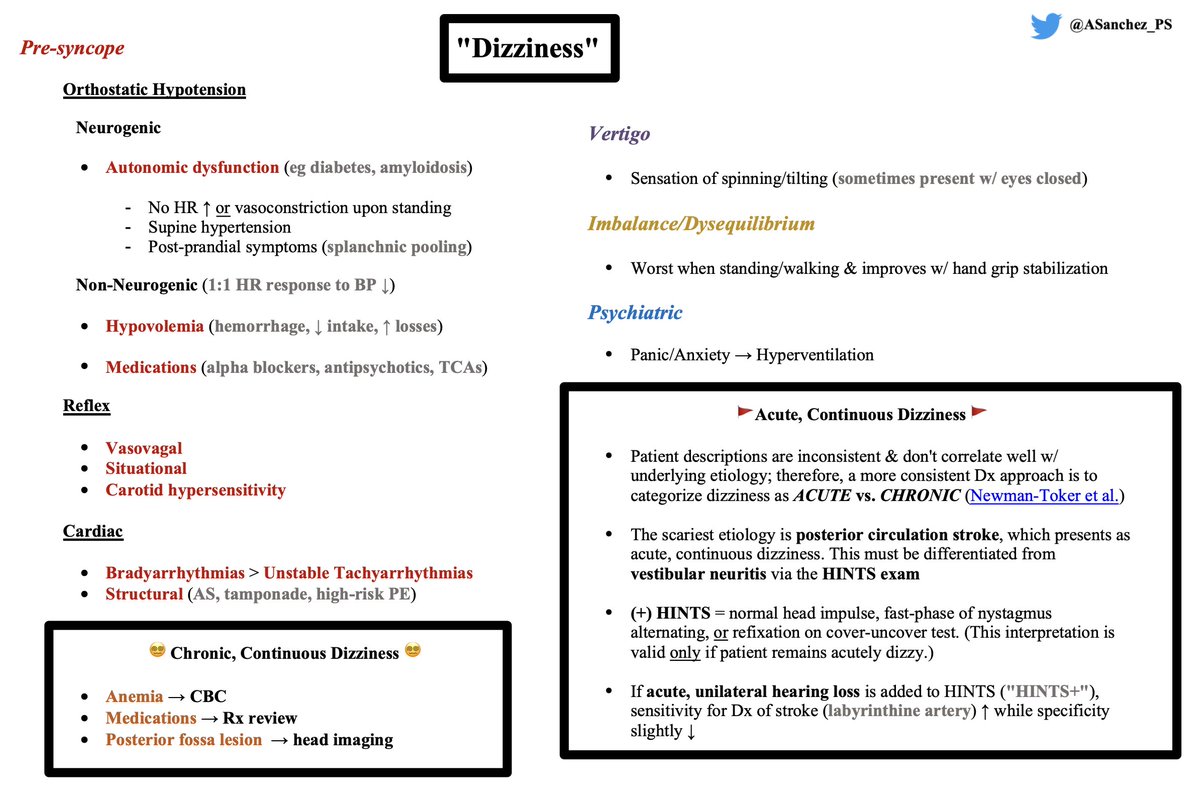
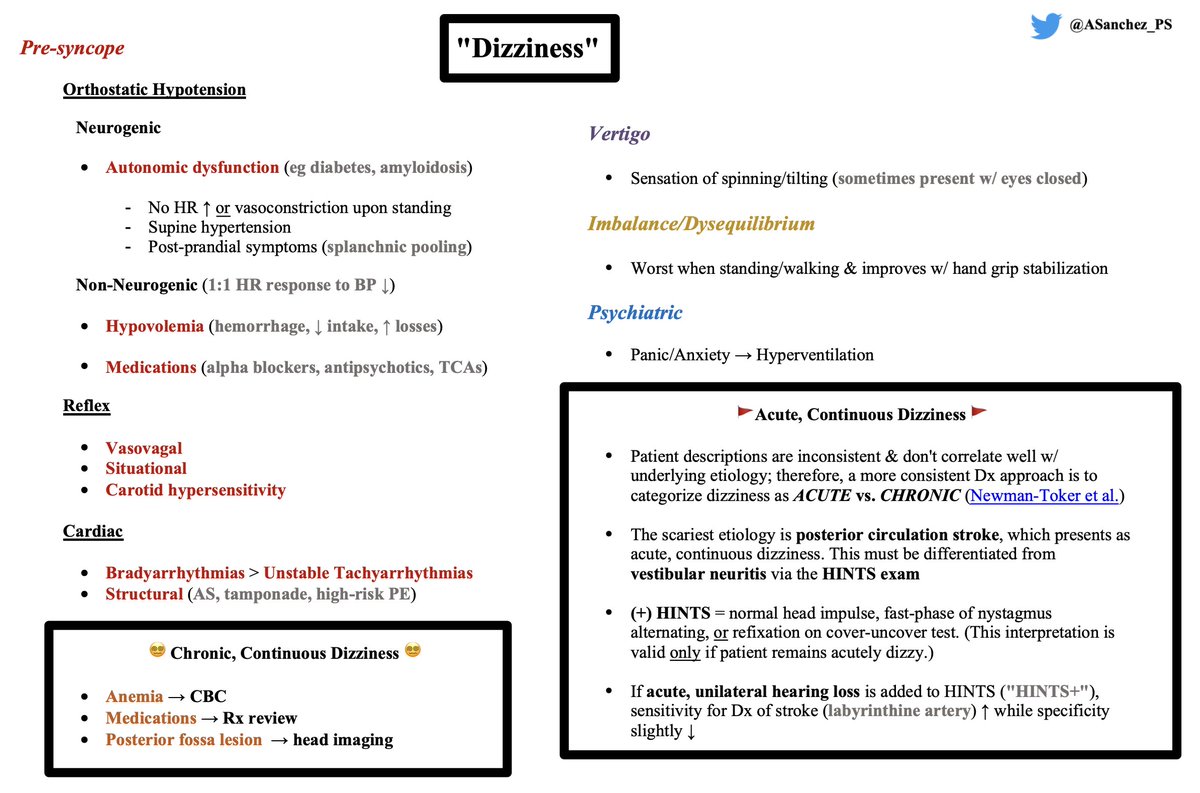
- Pre-syncope
- Vertigo
- Imbalance/Dysequilibrium
- Psychiatric
This approach is very much a bird's eye view approach that should assist in history/data acquisition. I'll also cover a tricky don't-miss Dx.
4 big buckets:
- Pre-syncope
- Vertigo
- Imbalance/Dysequilibrium
- Psychiatric
This approach is very much a bird's eye view approach that should assist in history/data acquisition. I'll also cover a tricky don't-miss Dx.
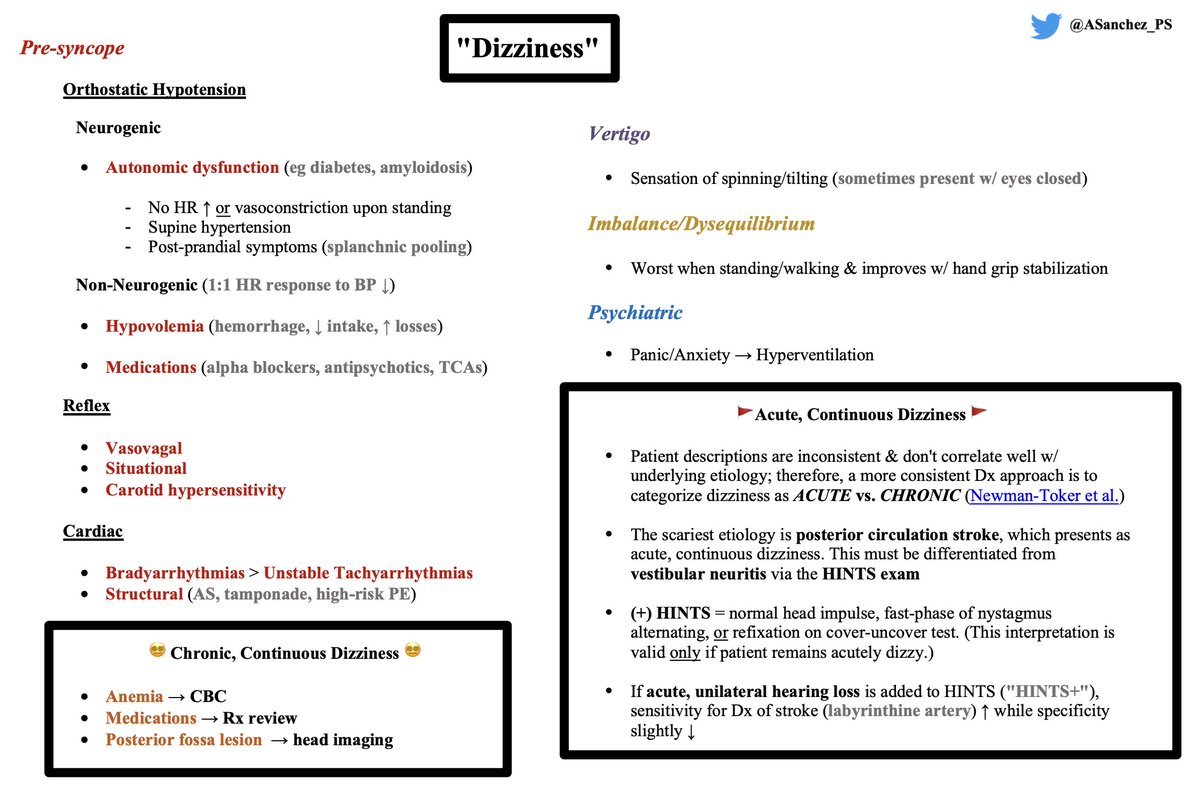
Dizziness 2/2 Pre-syncope:
🔴 History: "lightheadedness"
🔴 Pre-syncope DDx is stratified by the classic approach to syncope (orthostatic hypotension, reflex, cardiac)
Let's touch more on orthostatic hypotension, as this is not an endpoint Dx.
🔴 History: "lightheadedness"
🔴 Pre-syncope DDx is stratified by the classic approach to syncope (orthostatic hypotension, reflex, cardiac)
Let's touch more on orthostatic hypotension, as this is not an endpoint Dx.

Orthostatic hypotension = ↓ in systolic BP ≥ 20 mmHg / ≥ 10 mmHg in diastolic BP
Neurogenic etiologies 2/2 autonomic dysfunction are marked by:
🔴 No HR ↑ / vasoconstriction upon standing
🔴 Supine hypertension
🔴 Post-prandial symptoms (splanchnic pooling)
Neurogenic etiologies 2/2 autonomic dysfunction are marked by:
🔴 No HR ↑ / vasoconstriction upon standing
🔴 Supine hypertension
🔴 Post-prandial symptoms (splanchnic pooling)
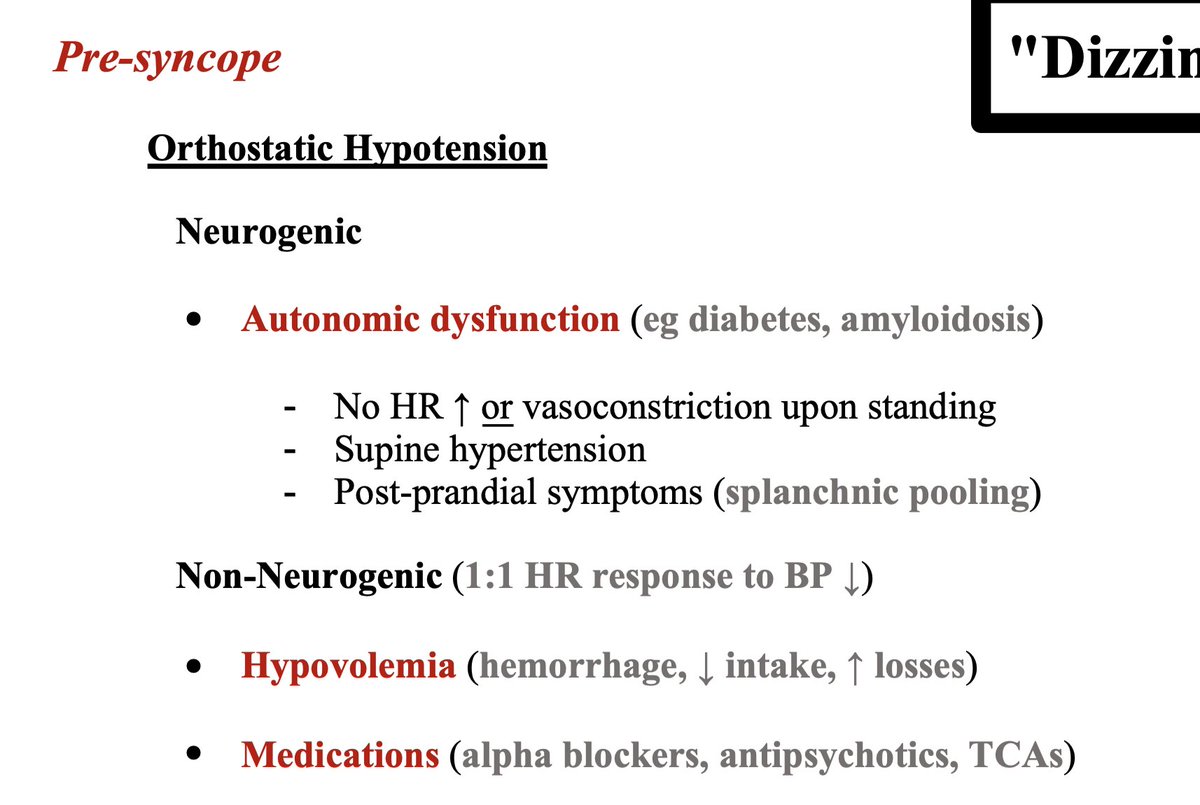
Non-neurogenic etiologies show a 1:1 HR response to ↓in BP (mmHg).
Consider:
🔴 Hypovolemia (hemorrhage, ↓ intake, ↑ losses)
🔴 Medications (alpha blockers, psychiatric meds)
Consider:
🔴 Hypovolemia (hemorrhage, ↓ intake, ↑ losses)
🔴 Medications (alpha blockers, psychiatric meds)
The remaining buckets encompass numerous disorders:
🟣 Vertigo (spinning/tilting sensation, often present w/ eyes closed)
🟡 Imbalance/Proprioception (worse when standing/walking & improves w/ hand grip stabilization)
🔵 Psychiatric (panic/anxiety → hyperventilation)
🟣 Vertigo (spinning/tilting sensation, often present w/ eyes closed)
🟡 Imbalance/Proprioception (worse when standing/walking & improves w/ hand grip stabilization)
🔵 Psychiatric (panic/anxiety → hyperventilation)
Patient history consistent with a specific etiology should prompt targeted testing.
BUT!
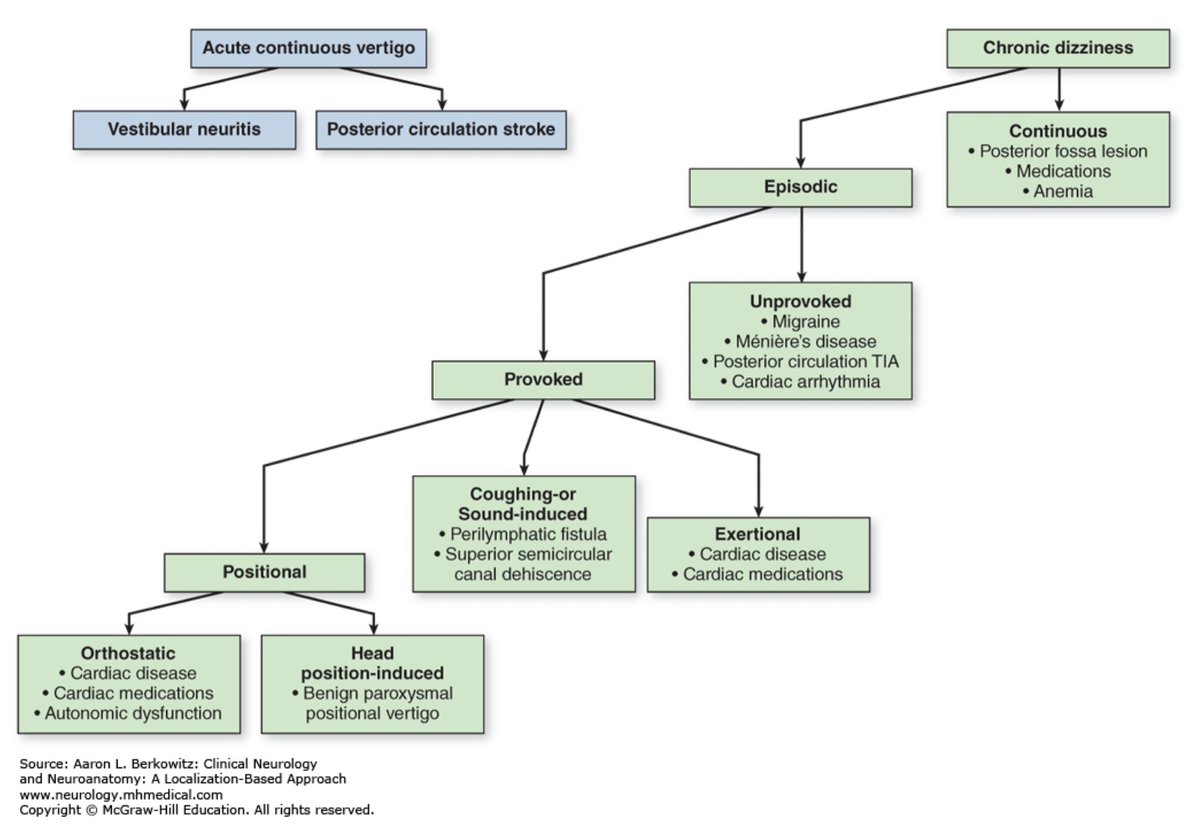
Patient descriptions are inconsistent & don't correlate well w/ underlying etiology; therefore, a more consistent Dx approach is to categorize dizziness as Acute vs. Chronic.
BUT!
Patient descriptions are inconsistent & don't correlate well w/ underlying etiology; therefore, a more consistent Dx approach is to categorize dizziness as Acute vs. Chronic.
I said I'd cover a tricky don't miss Dx: let's step into the world of acute, continuous dizziness.
DDx = posterior circulation stroke (!) vs. vestibular neuritis (benign)
If patient remains acutely dizzy, perform HINTS exam: youtube.com
DDx = posterior circulation stroke (!) vs. vestibular neuritis (benign)
If patient remains acutely dizzy, perform HINTS exam: youtube.com

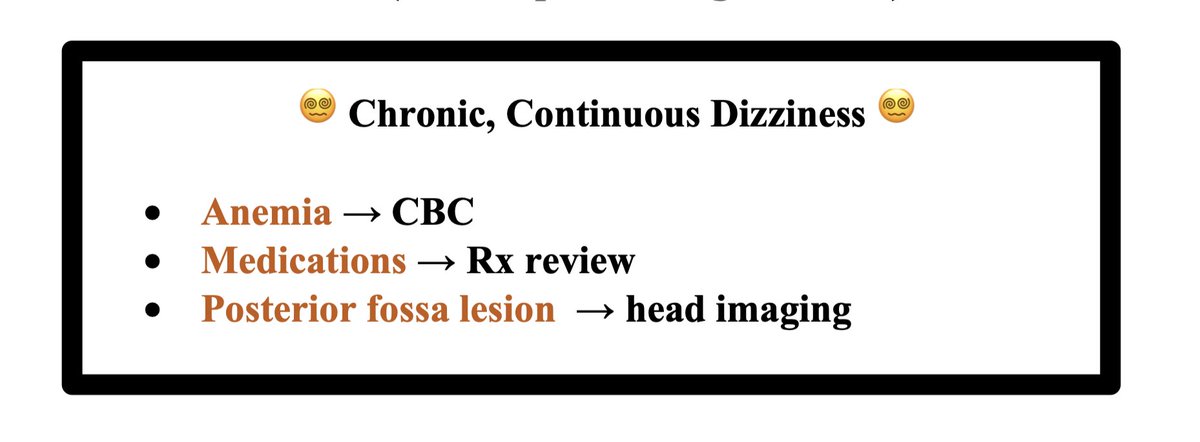
If dizziness is continuous & chronic, consider the following work-up:
😵💫 Anemia → CBC
😵💫 Medications → Rx review
😵💫 Posterior fossa lesion → Head imaging
😵💫 Anemia → CBC
😵💫 Medications → Rx review
😵💫 Posterior fossa lesion → Head imaging
Summary:
🏁 Dizziness DDx = pre-syncope, vertigo, imbalance/dysequilibrium, psychiatric
🏁 Orthostatic hypotension is not an endpoint Dx
🏁 Patient descriptions are inconsistent. If acute & continuous dizziness (vertigo), perform HINTS to assess for posterior circ. stroke
🏁 Dizziness DDx = pre-syncope, vertigo, imbalance/dysequilibrium, psychiatric
🏁 Orthostatic hypotension is not an endpoint Dx
🏁 Patient descriptions are inconsistent. If acute & continuous dizziness (vertigo), perform HINTS to assess for posterior circ. stroke
More thorough Dx approach to dizziness by @AaronLBerkowitz here. Buy his fantastic book!
References:
1) Dr. John Chang (all-star clinician educator @YaleIM_Chiefs)
2) n.neurology.org
3) accessmedicine.mhmedical.com by @AaronLBerkowitz
4) youtube.com
1) Dr. John Chang (all-star clinician educator @YaleIM_Chiefs)
2) n.neurology.org
3) accessmedicine.mhmedical.com by @AaronLBerkowitz
4) youtube.com
Loading suggestions...