
Health
Healthcare
Medical Research
Medical Technology
Gastroenterology
Medical Devices
Surgery
Surgical procedures

Hemostatic Forceps Tweetorial 🧵:
A useful thermal alternative for when you can’t “push” (bipolar probe) and precision work. It’s not just for ESD (Coagrasper). Hot biopsy forceps have been around for decades; not a novel tool! This is how surgeons do hemostasis.
#GITwitter
A useful thermal alternative for when you can’t “push” (bipolar probe) and precision work. It’s not just for ESD (Coagrasper). Hot biopsy forceps have been around for decades; not a novel tool! This is how surgeons do hemostasis.
#GITwitter

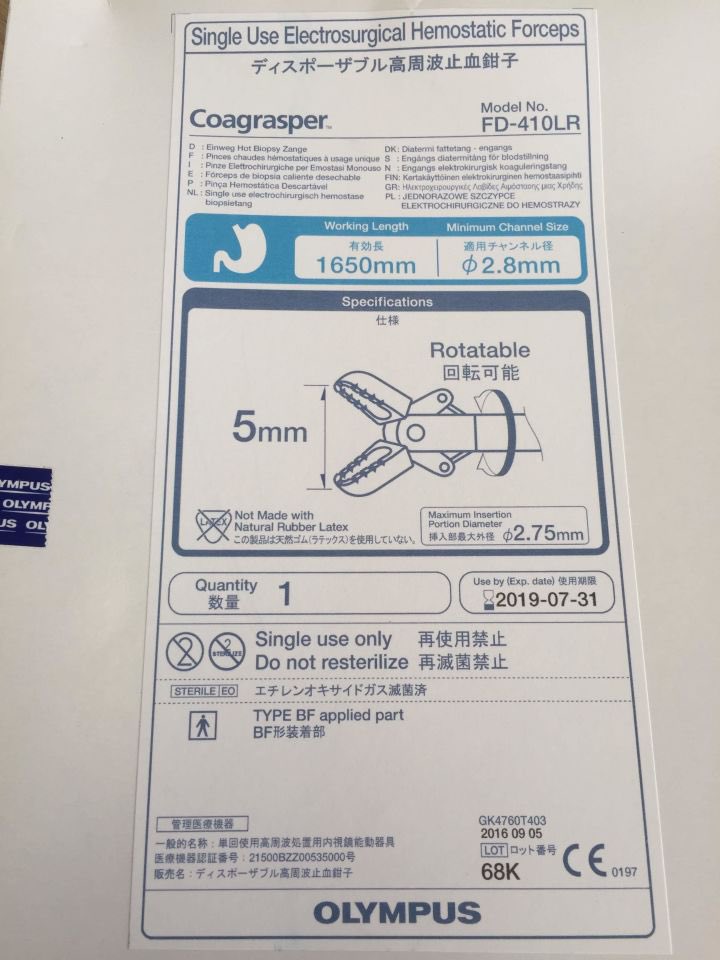
Olympus Coagrasper is smaller, newer (4-5mm opening width) and for precision work ($250).
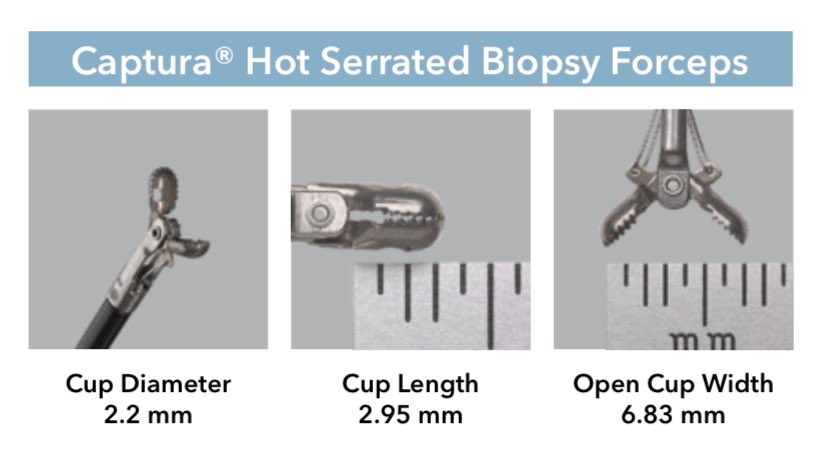
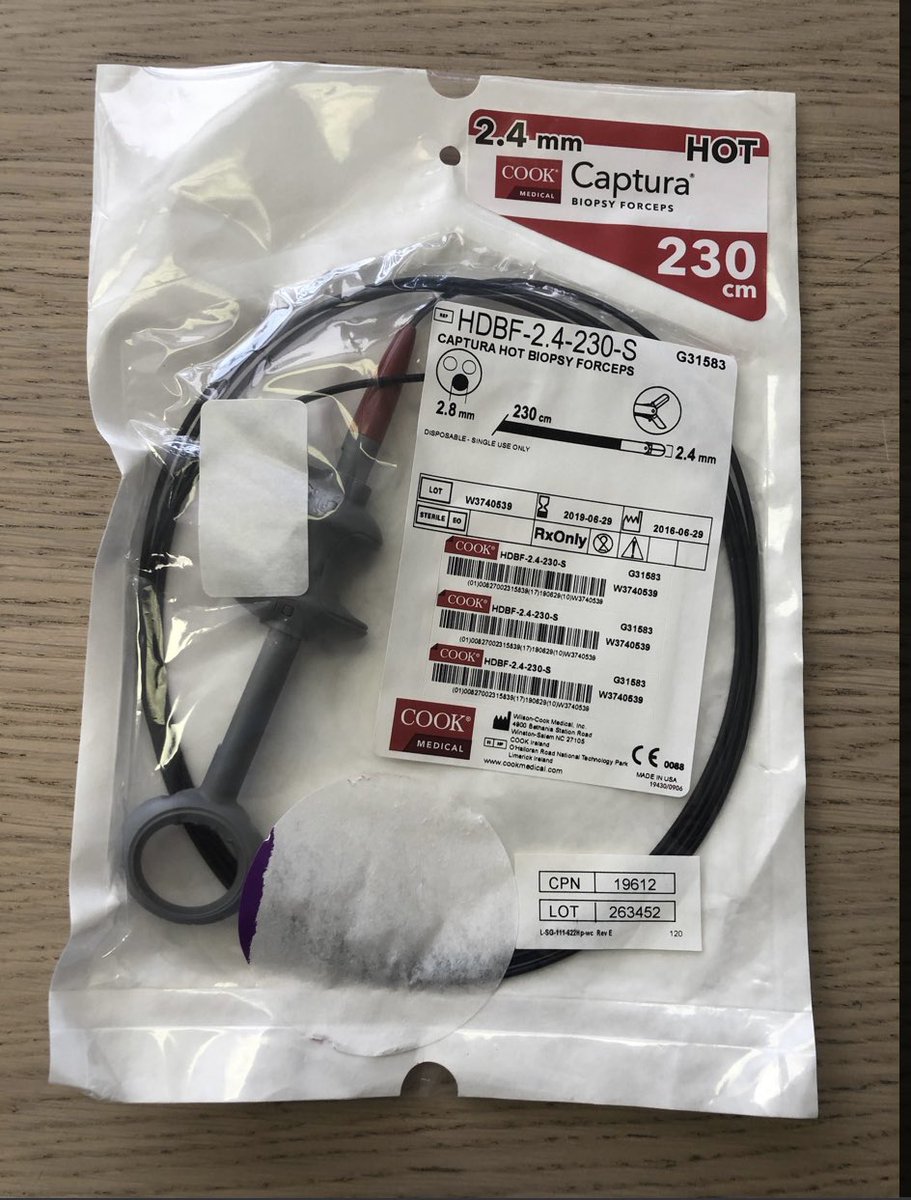
Hot biopsy forceps are larger with a cup and grab more tissue, less touchpoint work ($25)
Hot biopsy forceps are larger with a cup and grab more tissue, less touchpoint work ($25)

Dieulafoy vessel: Hemostatic forceps allow stable, quick mechanical and thermal hemostasis. This is not the only way to treat this. Bipolar or clips will be great. Epi injection I skip (no feedback if true hemostasis).
(2/)
(2/)

Anastamotic Ulcer vessel: A small vessel on a ridge with a soft base like this is favorable for hemostatic forceps. A bipolar probe can work but may feel more precarious when pushing forward. A clip is obviously excellent and I placed one for dual modality tx.
(3/)
(3/)

Post polypectomy bleeding: If you wish to have dual therapy, hemostatic forceps work well to grasp the cauterize the end of the stalk. A clip is always best to finish or solo. Dual therapy is probably overkill.
(4/)
(4/)

Post op anastomotic vessel: also quite amenable to hemostatic forceps as the vessels are on a ridge. Removing a clot also feels safer when concurrently cauterizing during the plucking maneuver.
(5/)
(5/)

Peptic Ulcer: An example of a larger vessel on the edge of a ridge where pushing with bipolar probe may result in unstable slippage. Consider hot biopsy forceps if you wanted thermal hemostasis or a clip (if not too fibrotic). Remember to not push with monopolar energy!
(6/)
(6/)

Anastomotic vessel: Bipolar probe on a ridge is possible but can be trickier to coaptive cauterize as seen here. Hemostatic forceps would have been a bit more efficient here. Yes, a clip was placed as dual therapy ( likely overkill )
(7/)
(7/)

Post sphincterotomy bleeding: small Coagrasper for precision work is where it shines. Bending the forceps tip slightly can get it to turn up if needed.
A bipolar probe would be less stable as you wouldn’t want to slip and burn the into CBD or PD orifice when pushing.
(8/)
A bipolar probe would be less stable as you wouldn’t want to slip and burn the into CBD or PD orifice when pushing.
(8/)

Post polypectomy bleeding: removing an adherent clot can be safely done with hot biopsy forceps during the plucking maneuver, as the junction between then vessel and the clot is often unclear. Once again a clip was placed as the final modality.
(9/)
(9/)

Acute polypectomy bleed: torrential bleed in EMR bed is quickly grasped and cauterized without pushing (bipolar) lest perforation. Pt positional change altered the vector of gravity to reveal the vessel.
Note this is a hot biopsy forceps.
Credit: @RobertBechara
(10/)
Note this is a hot biopsy forceps.
Credit: @RobertBechara
(10/)

Dieulafoy (suprapapillary): Coagrasper forceps via duodenoscope allows for precision cautery and avoiding pushing (bipolar probe) and avoiding the papillary orifice itself. Recall the technique is to lightly tug away before cauterizing. Stop when tissue whitens.
(11/)
(11/)

EMR : Exposed small arterioles in EMR beds is where the small Coagrasper shines. The small forceps can provide precision “touch point” hemostasis without grabbing muscle layer.
(12/)
(12/)

In summary, hemostatic forceps are a cost effective combination of mechanical and thermal hemostasis. You may not have a Coagrasper, but you likely have a dusty hot biopsy forceps ($25) lying about.
This is how surgeons cauterize. Only GI “push and pray” (bipolar probe).
(13/)
This is how surgeons cauterize. Only GI “push and pray” (bipolar probe).
(13/)
Consider them for AVMs, small vessel work (EMR), when you can’t push (papilla, rapid polypectomy bleed), or a vessel on a ridge (unstable probe). I always try for dual therapy (thermal +mechanical) to minimize rebleeding. The cheap hot bx forceps keeps it cost effective.
(14/)
(14/)
Loading suggestions...