

It is very common that new trainees ask us why we write Orthotopic Heart Transplant in the problem list, which sounds redundant to them. I was one of them, too.
Well, the reason we do so is because there are 2 ways to do a heart transplant...
Well, the reason we do so is because there are 2 ways to do a heart transplant...

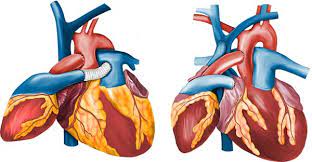
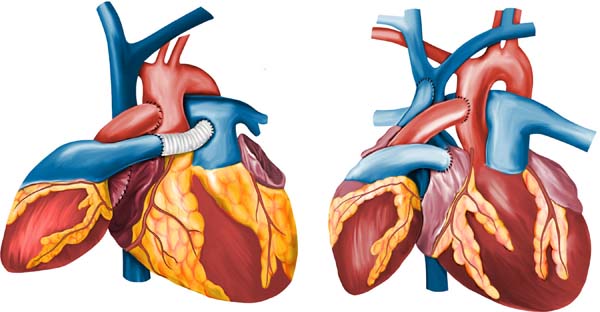
The classic one (orthotopic) in which you replace the diseased native heart for a healthy one from a donor
and
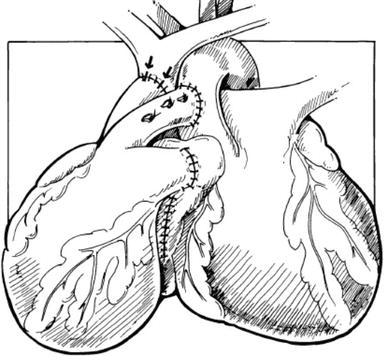
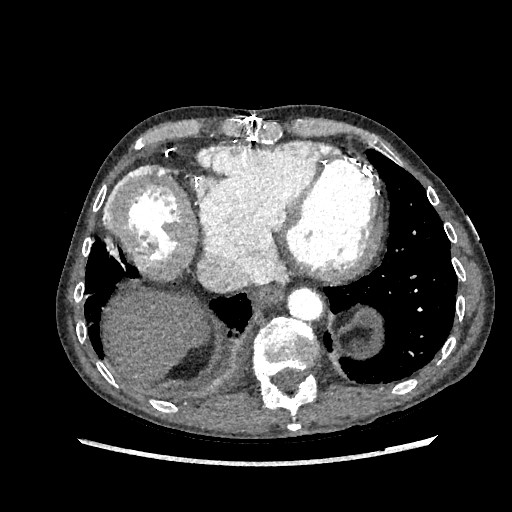
This one! The heterotopic or piggyback
and
This one! The heterotopic or piggyback
This option was used in the past for patients with severe and/or fixed pulmonary hypertension and severe pulmonary vascular resistance in the absence of native right ventricular failure. Basically a primitive (and organic) VAD
Harefield has a handful of HHTx patients, many of them have survived 20+ years post-tx. They have their own particularities as you could imagine. Also, in our cohort, the anastomosis is donor PA to native RA to avoid the need to use prosthetic material
The 2 most commons problems we face in the late stage are:
- RV dysfunction as the donor RV pumps the blood to a dilated and often dysfunctional chamber (native RV) losing efficiency
- And:
- RV dysfunction as the donor RV pumps the blood to a dilated and often dysfunctional chamber (native RV) losing efficiency
- And:
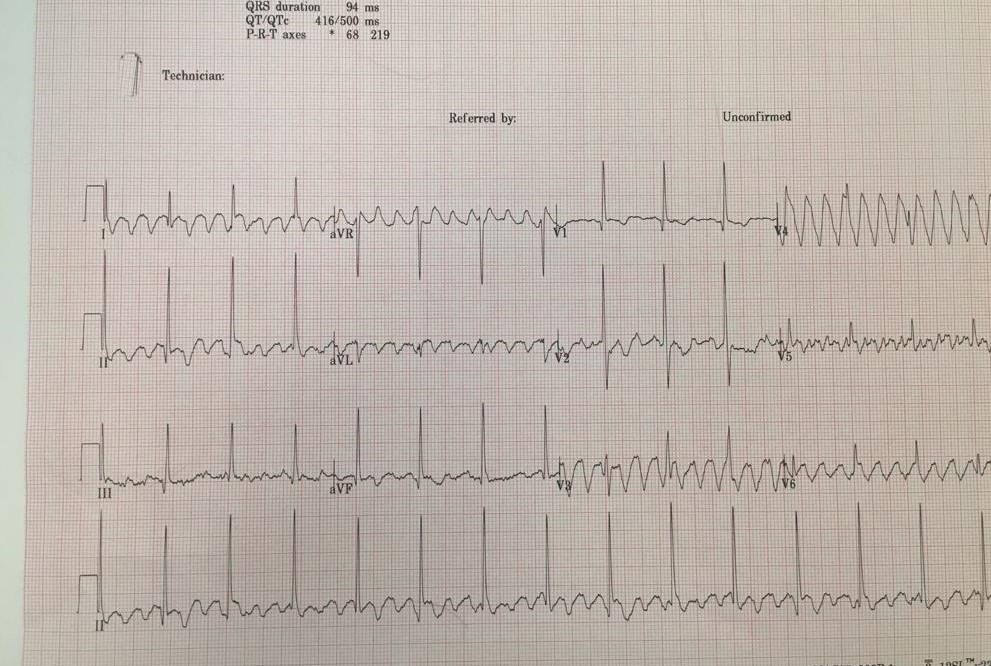
As in LVAD patients, HHTx ones tend to tolerate native heart VT quite well and this heart is not the main contributor to the cardiac output. Very often, they walk to the hospital complaining of palpitations and lethargy but HD stable

The initial management is very typical:
- Anti-arrhythmics is HD ok
- DCCV if not or failure to pharmacological options
Interestingly, you need to synchronize the shock to donor's heart rhythm.
- Anti-arrhythmics is HD ok
- DCCV if not or failure to pharmacological options
Interestingly, you need to synchronize the shock to donor's heart rhythm.
We also try to identify the potential cause:
- Electrolyte dysbalance
- New ischaemic injury
- Progressive HF
- Progressive valvular disease (typically AR)
- Chronic scar
- Electrolyte dysbalance
- New ischaemic injury
- Progressive HF
- Progressive valvular disease (typically AR)
- Chronic scar
You shouldn't forget the donor's heart can have VT too, like in the traditional way of transplantation: CAV, rejection, scar, etc, so make sure you got right what ventricle it is!
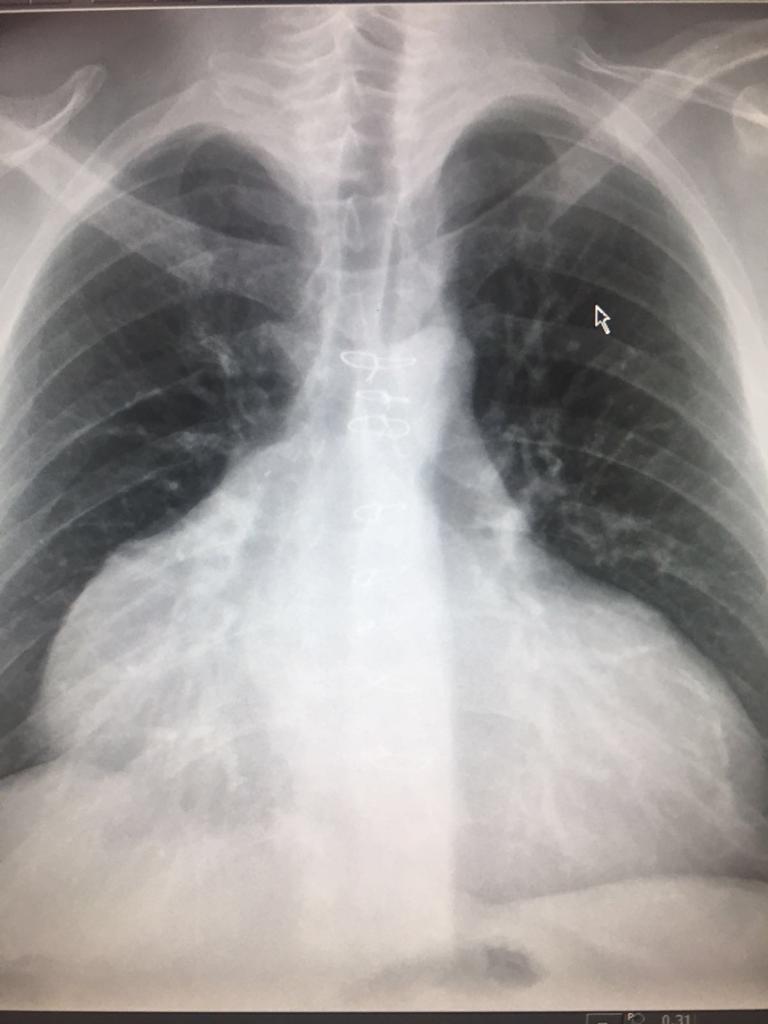
Now is when our patient comes to play: 70M patient with a HHTx in the early 90s for IHD. Native heart function is poor. Donor heart function is preserved. He has no DSA and no evidence of CAV.
He has had several VT episodes managed with either amiodarone infusion of DCCV.
He has had several VT episodes managed with either amiodarone infusion of DCCV.
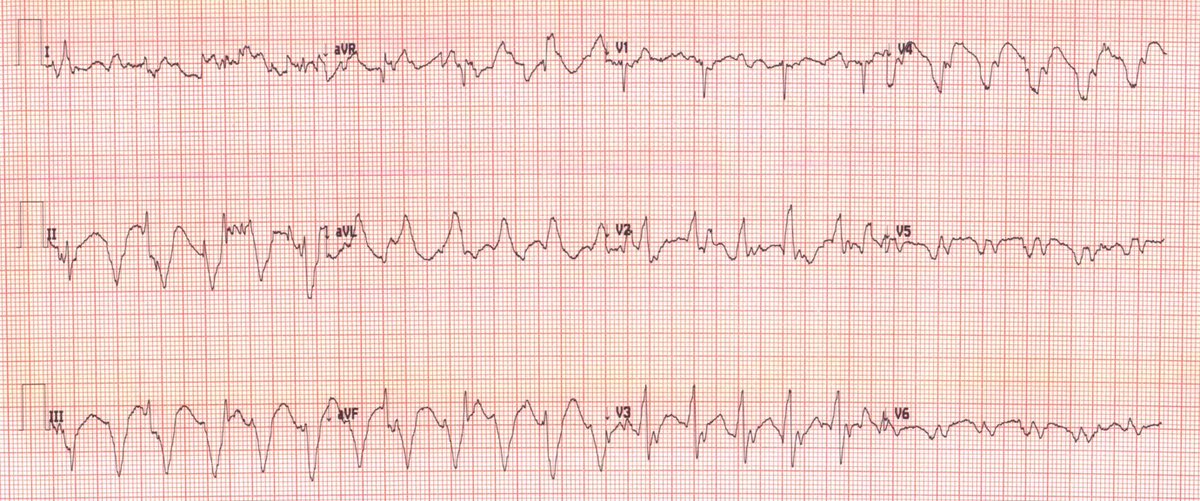
However one of these episodes became refractory to cardioversion so he underwent VT ablation which terminated the arrhythmia BUT lead to asystole 😱not responding to atropine nor isoprenaline
What would you do then:
3rd option would be cool but is a bit unrealistic, especially taking into account the age and clinical situation.
We have done option number 4 in one occasion, for a patient who had extremely advanced RV dysfunction but we would not consider it for a rhythm issue (and is risky)
We have done option number 4 in one occasion, for a patient who had extremely advanced RV dysfunction but we would not consider it for a rhythm issue (and is risky)
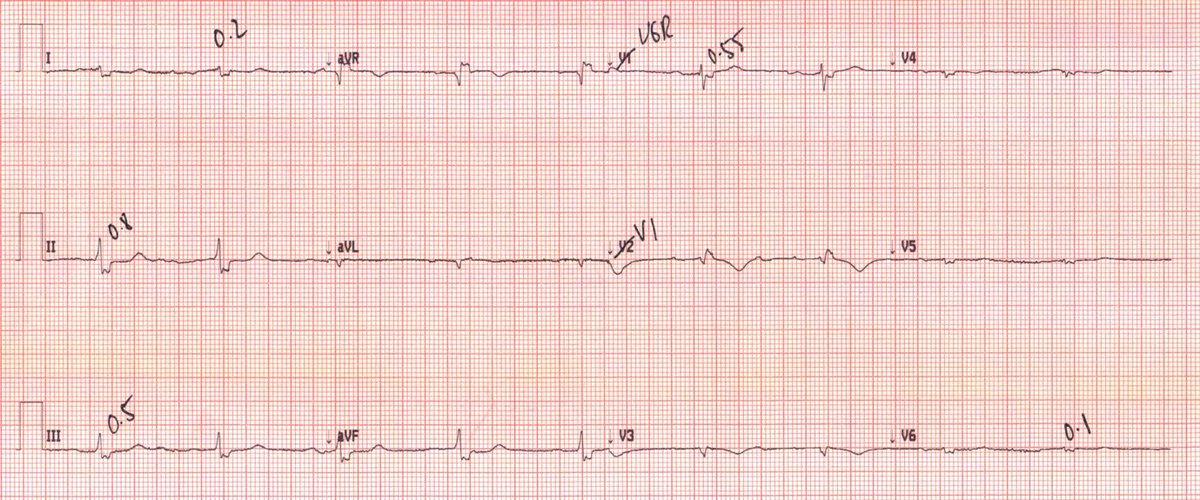
Between the first 2 options, leaving the heart in asystole seemed unsatisfactory since the patient had good QoL and we needed the native's RV contribution to maintain adequate CO.
So we went for option 2
So we went for option 2
We decided to implant a single chamber PPM into his native RV. After several attempts, we found a suitable position for capture and the heart started beating again!
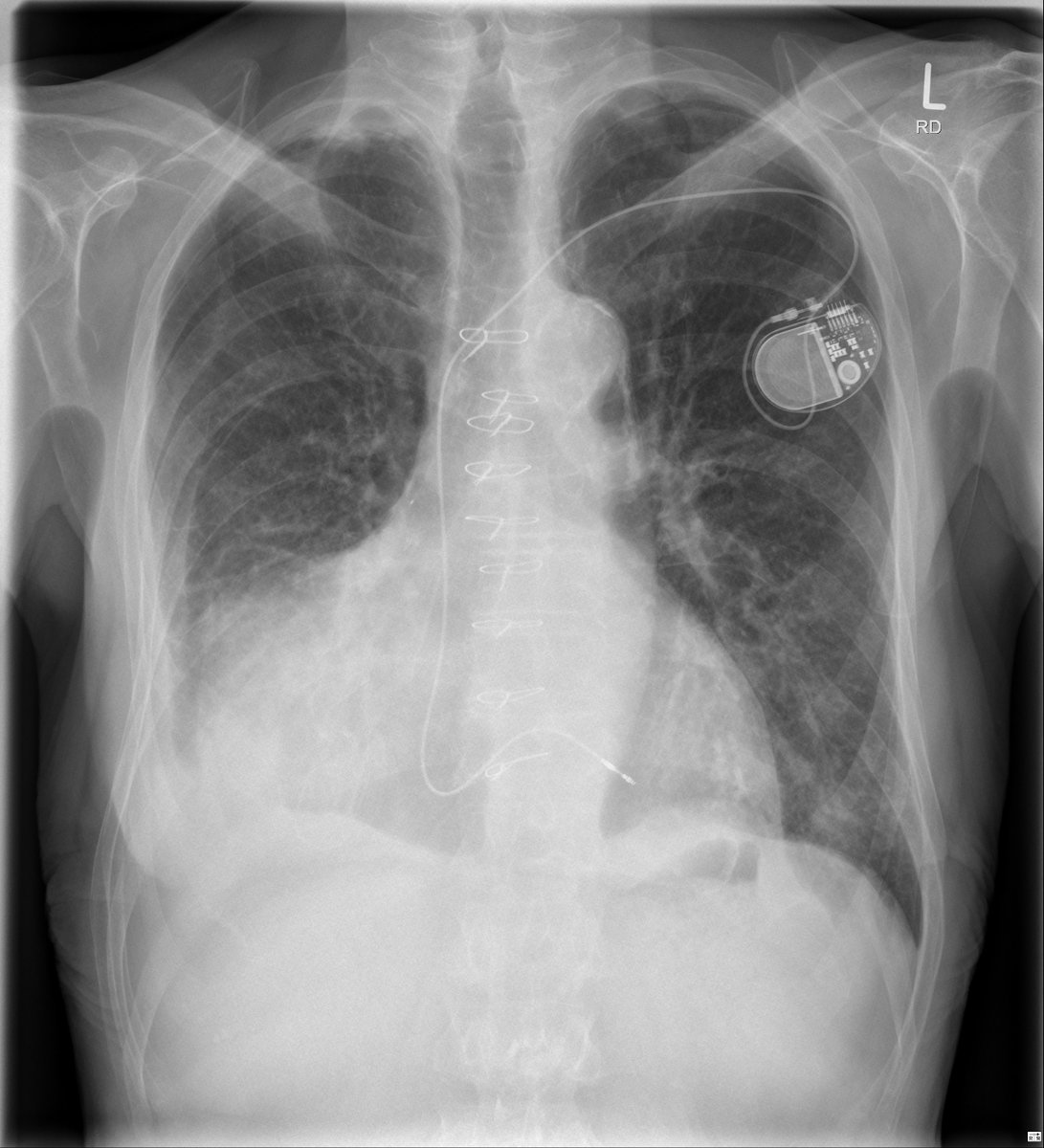
The patient survived the admission and PPM insertion and was discharged home 1 month after he came in. His cardiac function remained optimal in his last clinic appointment 6 months after. His resilience was impressive and inspiring, what a true character!

Can't even start with what lessons we learnt, it was a whole compendium of cardiology and physiology!
But happy to hear your comments and questions!
But happy to hear your comments and questions!
I hoped you liked this case and enjoyed this week as much as I did. It’s time to disconnect, too much cardiology!
But before I leave and handover the account to one of my pals, take the time to enjoy this song from my favorite band in the world.
open.spotify.com
But before I leave and handover the account to one of my pals, take the time to enjoy this song from my favorite band in the world.
open.spotify.com
Loading suggestions...