

THREAD OF STEP BY STEP EXPLANATION OF HOW A CAESARIAN SECTION IS DONE
content warning 🚨: sensitive content in thread
#MedTwitter
1. Preoperative steps: this patient was undergoing an emergency CS. In this instance it is now our practice to prep the vagina with iodine solution
content warning 🚨: sensitive content in thread
#MedTwitter
1. Preoperative steps: this patient was undergoing an emergency CS. In this instance it is now our practice to prep the vagina with iodine solution

An IDC was already in situ as the patient had an epidural in labour. TED stockings have been placed on the patient for VTE prophylaxis.
2. IV antibiotics: currently the Therapeutic Guidelines recommend 2 g IV Cephazolin as routine prophylaxis 15–60 minutes prior to skin incision
2. IV antibiotics: currently the Therapeutic Guidelines recommend 2 g IV Cephazolin as routine prophylaxis 15–60 minutes prior to skin incision

3. Skin preparation for caesarean section with chlorhexidine-alcohol prep, which should be allowed to dry prior to draping. It is important that solution does dry and doesn’t pool underneath the drapes, as this is a fire risk and patient burns have occurred previously.

4. Skin incision: the Joel Cohen technique involves making a straight incision 3 cm below the level of the anterior superior iliac spines.

5. Entry technique: sharp entry through the skin, middle 3 cm of the subcutaneous fat and rectus sheath is demonstrated here.

6. Blunt extension of the subcutaneous tissue and rectus sheath.

THREAD PAUSED.🛑
@gyn_doctor follow me to learn more. Check out on my content. You won't regret.🥰♥️🔥🧑⚕️
Men's health, Reproductive, obstetrics and gynecology!
@gyn_doctor follow me to learn more. Check out on my content. You won't regret.🥰♥️🔥🧑⚕️
Men's health, Reproductive, obstetrics and gynecology!

7. Blunt entry into the peritoneal cavity is used as a part of the Joel Cohen caesarean section technique. This should be done high in order to avoid entering into the bladder, which may be high following prior CS or in the advanced stages of labour.

8. 8a (Left) & 8b (right). Creation of a bladder flap. The loose utero-vesical peritoneum is identified. It should be opened approximately 2 cm below the level of its fixed attachment to the uterus in the midline and extended laterally each side.
The peritoneum can then be
The peritoneum can then be
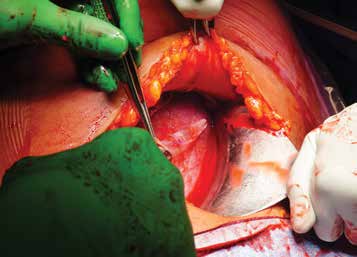

picked up with forceps and the bladder gently separated from the lower segment bluntly with the forefinger, or in the presence of adhesions sharply reflected down.
9. Uterine entry: this demonstrates cephalad-caudad blunt extension of the uterine incision performed after making a small 2–3 cm horizontal sharp incision on the lower uterine segment.

10. 10a (right) & 10b (left). Delivery of the fetal head is usually achieved with flexion and elevation of the fetal head toward the uterine incision, and then completed with the addition of the assistant giving fundal pressure (10b). In photo 10a, forceps delivery of the fetal


head is demonstrated, which may be necessary in the elective setting where the fetal head can still be high.
11. Spontaneous delivery of the placenta: fundal massage and controlled cord traction are being used here to achieve spontaneous delivery of the placenta.
11. Spontaneous delivery of the placenta: fundal massage and controlled cord traction are being used here to achieve spontaneous delivery of the placenta.

12. An oxytocic is usually given following the delivery of the baby to reduce the risk of PPH, and here is shown an oxytocin infusion, as is current evidence-based practice.
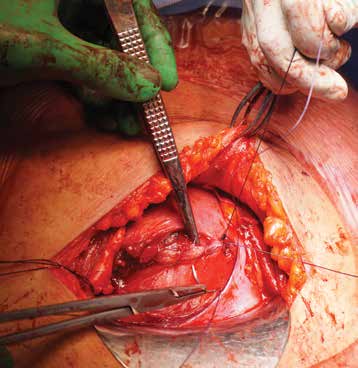
13. Identifying the uterine incision and uterine angles: it is useful to place Green-Armytage forceps on the upper and lower edges of the uterine incision to ensure they are identified correctly (particularly the lower edge, which can at times recede inferiorly and be

difficult to identify because of bleeding, which has led some to mistake the posterior wall of the lower segment for the lower edge of the uterine incision). This practice also allows clear identification of the uterine angles that are often secured first.
14. Closure of the uterus: here the uterus is closed with a double-layer, non-locking continuous monofilament (1 monocryl) suture. The first layer should include the cut edge of the myometrium and achieves haemostasis. The second layer pulls uncut myometrium together in order to
cover the first layer.
15. Checking the tubes and ovaries should be done routinely at caesarean section, so as not to miss any adnexal pathology.
15. Checking the tubes and ovaries should be done routinely at caesarean section, so as not to miss any adnexal pathology.

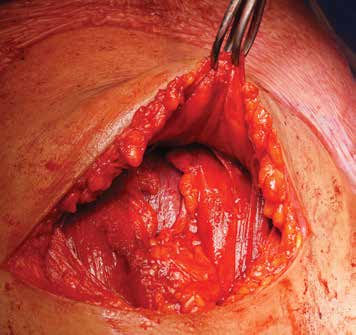
16. Non-closure of the peritoneum. Haemostasis between the rectus sheath and muscle should be checked at this point because of the risk of injury to perforating vessels during entry.
17. Rectus sheath closure is demonstrated here with a 1 PDS suture, using a continuous non-locking technique.

18. The subcutaneous fat in this instance has not been closed as it is less than 2 cm. A continuous subcutaneous suture is used for skin closure.

Special thanks to Dr. Francis Hills where I adopted the article.
Retweet, like and comment.
Follow me @gyn_doctor to learn more about reproductive, obstetrics and gynecology plus men's health content.
Retweet, like and comment.
Follow me @gyn_doctor to learn more about reproductive, obstetrics and gynecology plus men's health content.
For more reasons why a doctor might consider a caesarian section delivery as the best for mothers, check out in this thread 👇👇
Loading suggestions...