

#JustAnOtherDayOnICU
You are asked to do POCUS on a 72 y/o lady with increasing norepinephrine requirements (0.4 mcg/kg/min) and lactate second day post total pancreatectomy and splenectomy for ca.
Clips, questions and 'what happened' in the long thread below.
#POCUS #EchoFirst
You are asked to do POCUS on a 72 y/o lady with increasing norepinephrine requirements (0.4 mcg/kg/min) and lactate second day post total pancreatectomy and splenectomy for ca.
Clips, questions and 'what happened' in the long thread below.
#POCUS #EchoFirst
1/
First quiz time:
What do these numbered traces represent on this LV CW doppler trace?
First quiz time:
What do these numbered traces represent on this LV CW doppler trace?
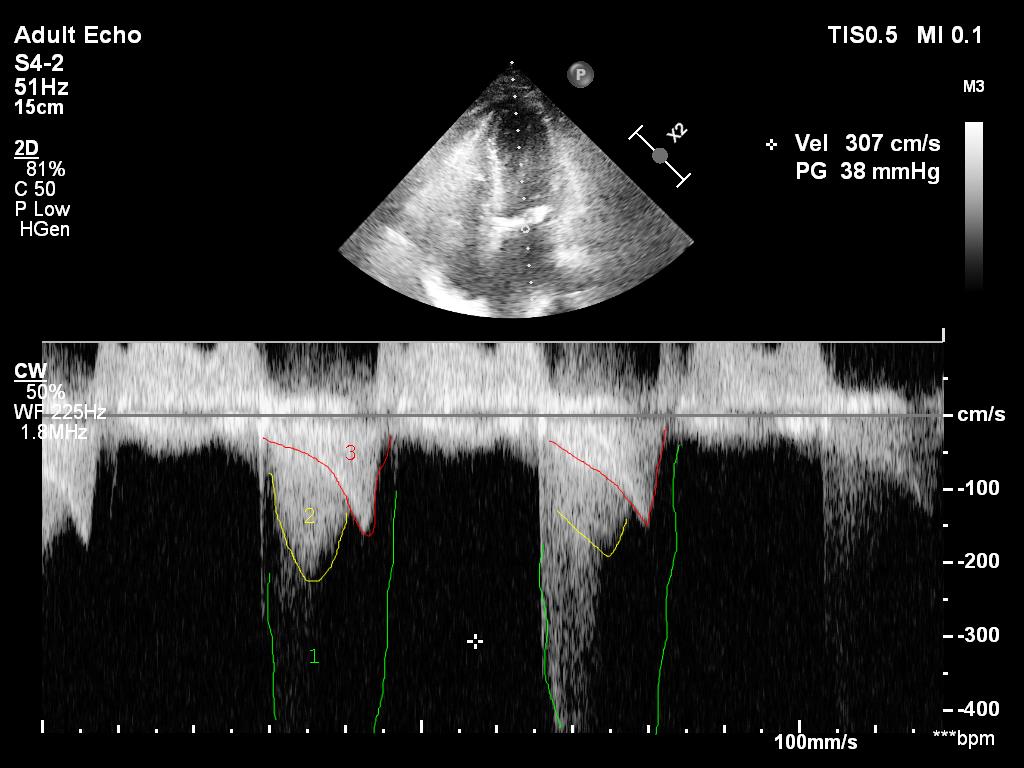
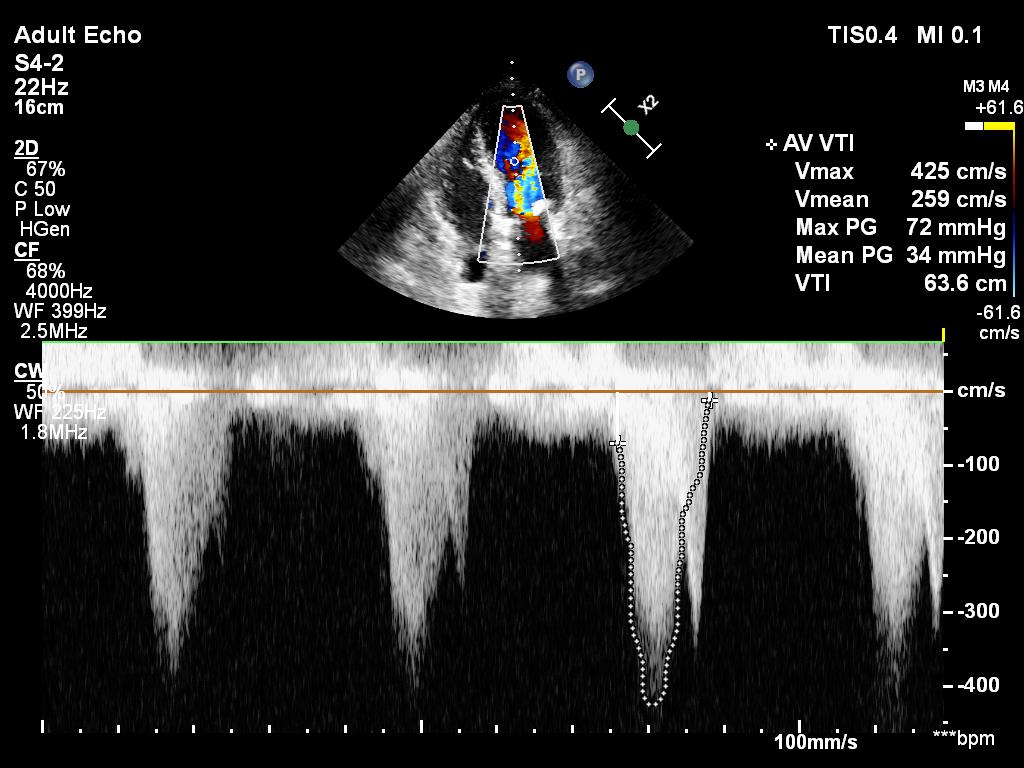
2/ I cheated. This is actually a pic after an intervention. This was the original.
3/ And more POCUS clips for you.
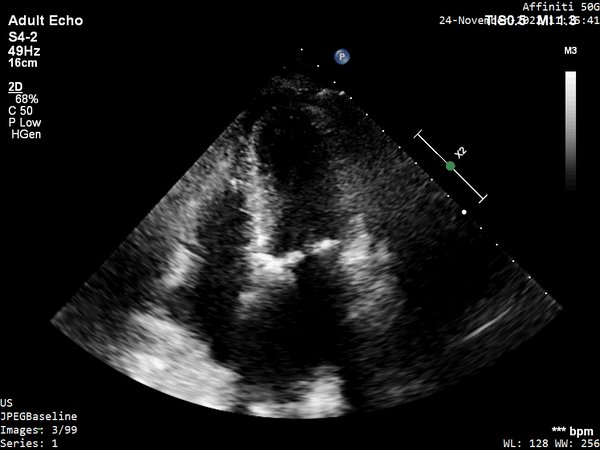
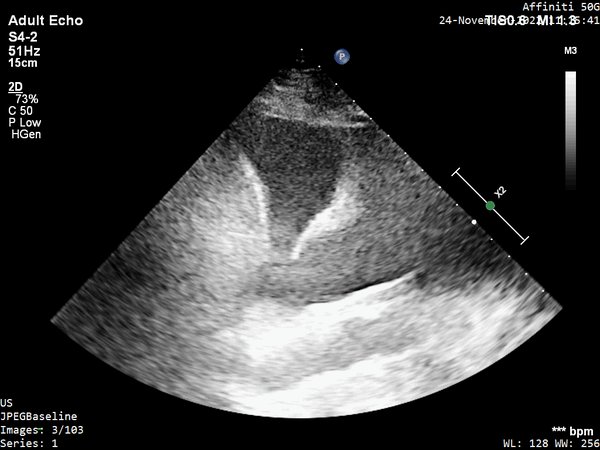
A4C
A4C
4/ A4C w/ colour

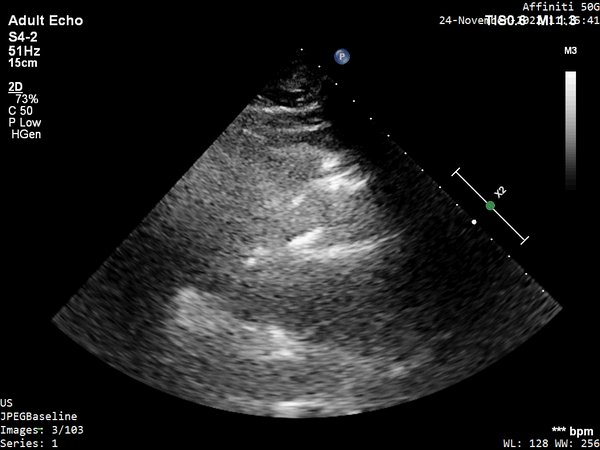
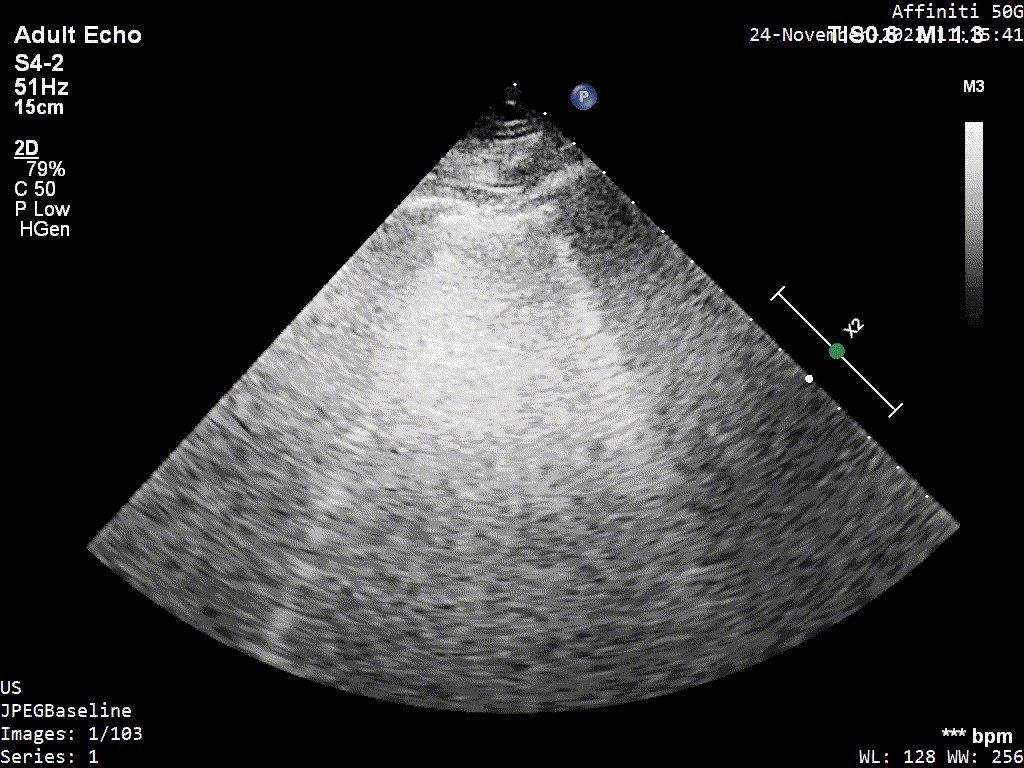
5/ PLAX
6/ Left lung
7/ Right lung
8/ and VEXUS...although not easy and quality not ideal
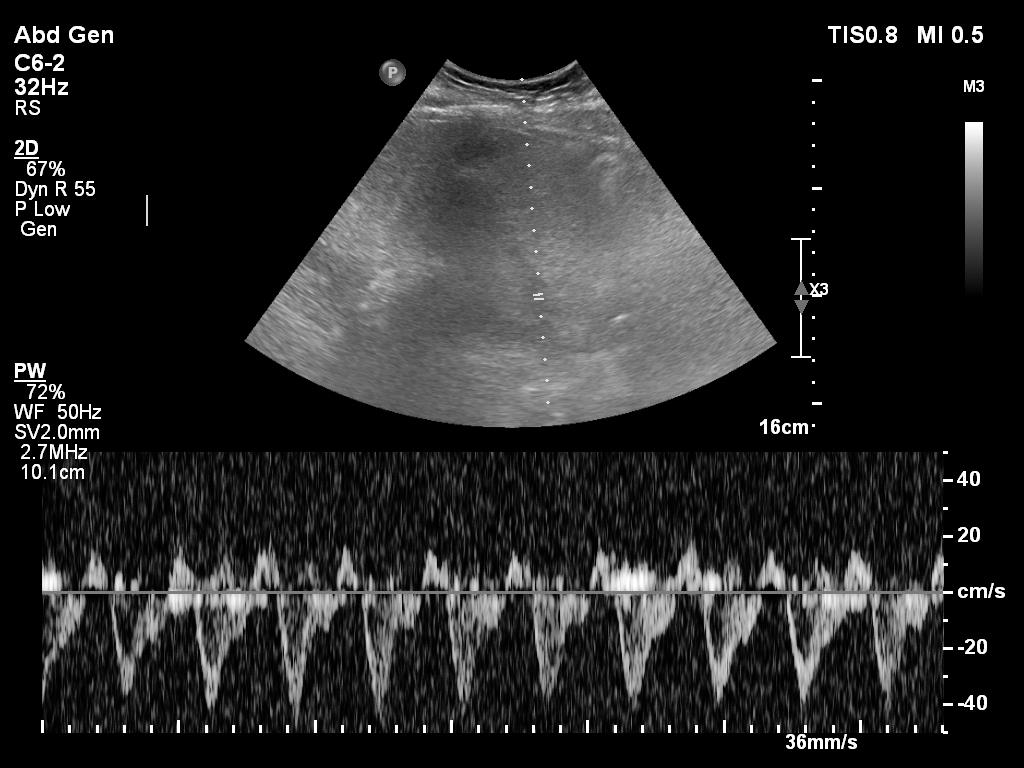
hepatic vein
hepatic vein
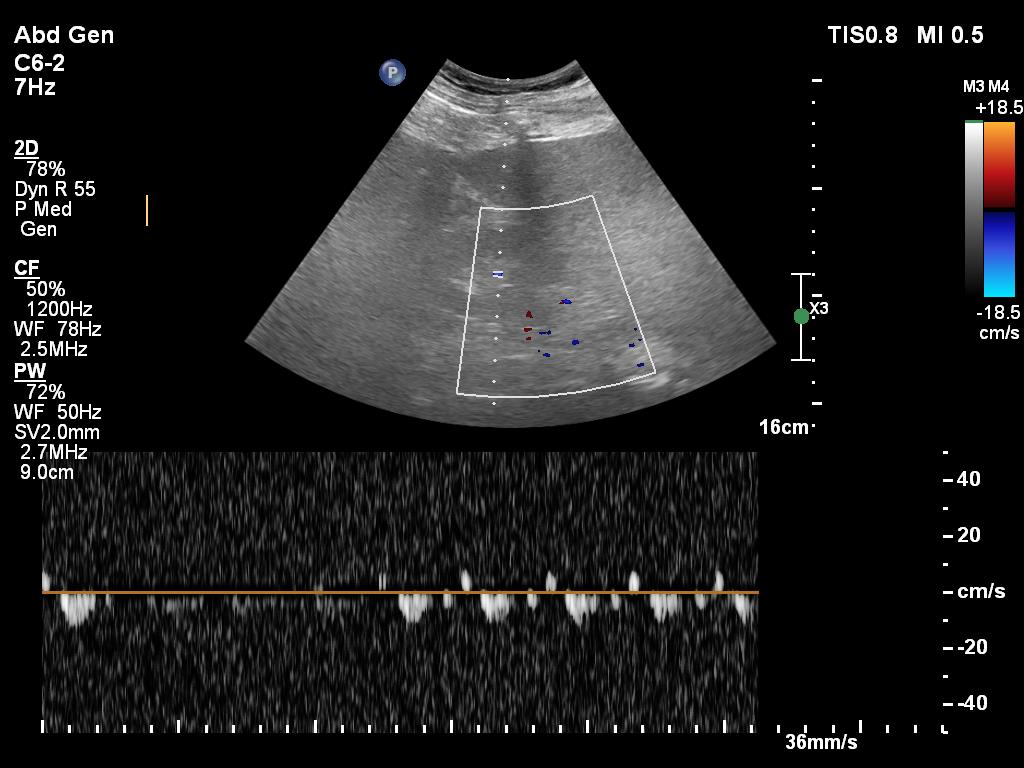
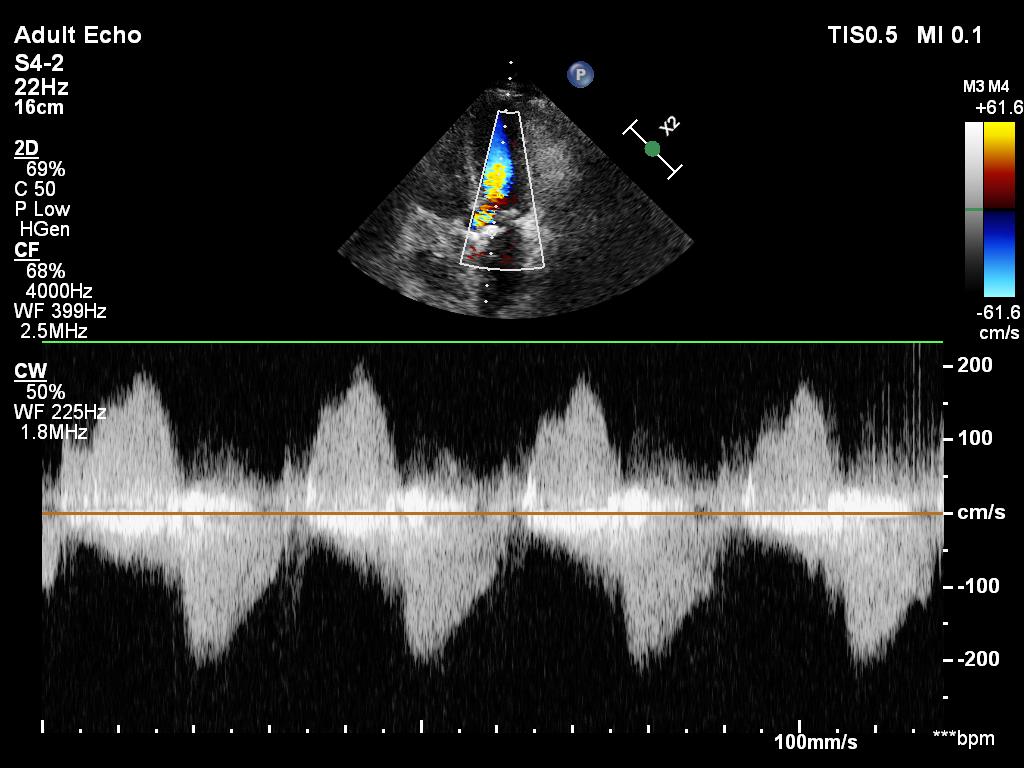
9/ portal vein

10/ renal vein (or not :)
11/ So what's the probelm and haemodynamic intervention you suggest?
1) Fluid challenge
2) Beta blockers
3) Vasopressin
4) Something else
1) Fluid challenge
2) Beta blockers
3) Vasopressin
4) Something else
12/ Back to the clips:
The first quiz pic shows
1) mitral regurgitation - probably only mild
2) flow across the aorta - aortic stenosis?
3) intraventricular obstruction
Let's look at the last two detail
The first quiz pic shows
1) mitral regurgitation - probably only mild
2) flow across the aorta - aortic stenosis?
3) intraventricular obstruction
Let's look at the last two detail
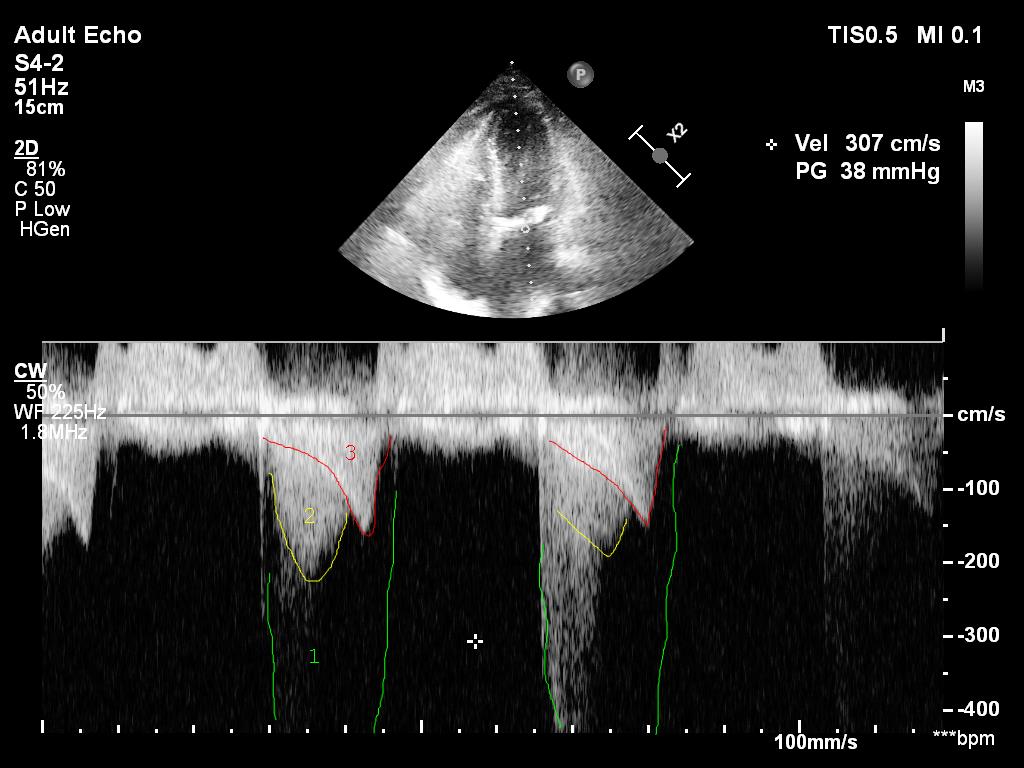
13/ On this earlier pic the intraventricular peak gradient (red late peaking, saber like) is 43hgmm. It is considered 'obstruction' if PG is above 30hgmm and hemodynamically significant if above 50hgmm. This one here is clearly an issue.
Is there aortic stenosis too though?
Is there aortic stenosis too though?
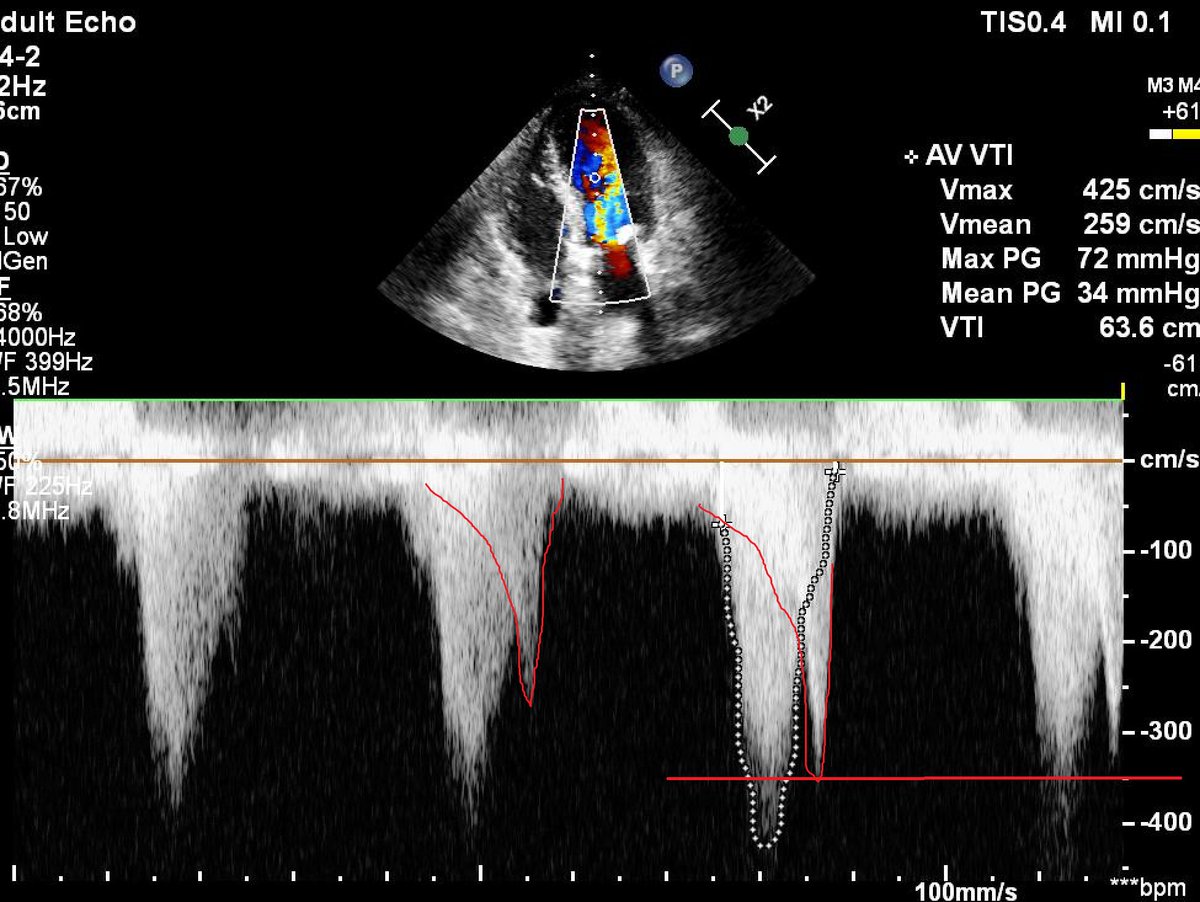
14/ If I just look at the mean gradient on the previous clip (34hgmm), there is. However, it is impossible to calculate the true gradient if there is an intraventricular obstruction.
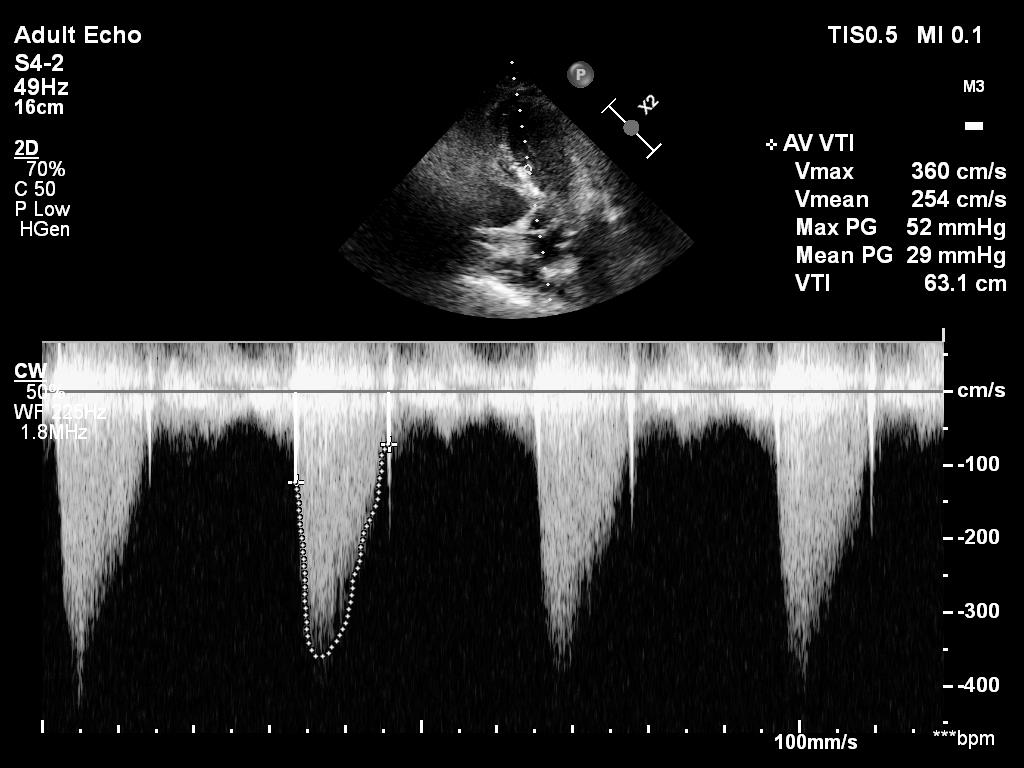
15/ I tried my best to 'isolate' the aorta in A5C, but still it is impossible to tell how much the intraventricular acceleration contributes.
16/ Intraventricular obstruction can be caused by:
1) reduced LV filling du to hypovolemia or vasodilatation
2) reduced afterload due to vasodilatation
3) LV hypertrophy secondary to a sclerotic aortic valve/hypertension (this case)
1) reduced LV filling du to hypovolemia or vasodilatation
2) reduced afterload due to vasodilatation
3) LV hypertrophy secondary to a sclerotic aortic valve/hypertension (this case)
17/ 4) hypercontractile LV due to endogenous or exogenous cathecolamines
5) HCM or other structural abnormalities not present in this case
5) HCM or other structural abnormalities not present in this case
18/ Treatment is logical:
1) fluids
2) avoid cathecolamines especially dobutamine, but vasopressin is best
3) beta-blockers
More on this @PulmCrit emcrit.org though this is not a classic LVOTO with SAM, the obstruction is intra/midventricular.
1) fluids
2) avoid cathecolamines especially dobutamine, but vasopressin is best
3) beta-blockers
More on this @PulmCrit emcrit.org though this is not a classic LVOTO with SAM, the obstruction is intra/midventricular.

19/ In this case I advised starting vasopressin but holding fluids and Also beta blockers for now.
My rationale behind fluids was that the patient was already net positive 3000ml in 24 hrs, urine output was low.
POCUS showed 'fluids' in the lungs (B profile, pleural effusion).
My rationale behind fluids was that the patient was already net positive 3000ml in 24 hrs, urine output was low.
POCUS showed 'fluids' in the lungs (B profile, pleural effusion).
20/ My interpretation of VEXUS is Grade I: normal hepatic vein, mild portal vein pulsatility and biphasic renal vein flow. But pancreatitis is a 'leaky' state, so VEXUS is often not very abnormal as fluid readily leaks to the tissues.
21/ What happened?
After starting vasopressin with 2U/h noradrenaline could be reduced and intraventricular obstruction improved from 43hgmm to 9 hgmm. Urine output picked up. Pt was discharged 2 days later.
After starting vasopressin with 2U/h noradrenaline could be reduced and intraventricular obstruction improved from 43hgmm to 9 hgmm. Urine output picked up. Pt was discharged 2 days later.
22/ I went back to see her a week later because I was really curious to see her in a 'lower flow state'. I wanted to check the aortic valve (is there stenosis?) and also the mitral (some hidden nuggets there).
Intraventricular obstruction almost disappeared...
Intraventricular obstruction almost disappeared...
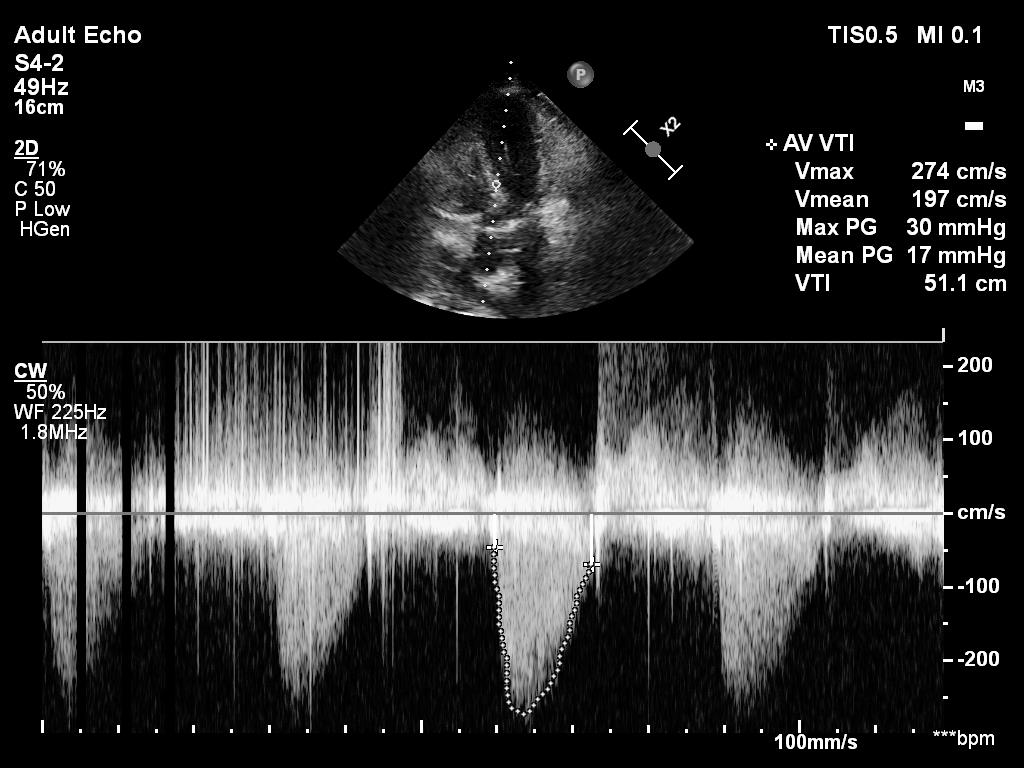
23/ Mean aortic gradient was only 17hgmm (reduction from 34). This corresponds to NO aortic stenosis (cutoff 20hgmm, Vmax 2.5m/s) and I reported it as aortic sclerosis.
24/
Lastly a theoretical haemodynamic question:
Can reduction of afterload lead to intraventricular obstruction if there is a sclerotic aortic valve? Does it not provide a 'fixed obstruction' that overrides reduction of afterload due to vasodilatation?
Lastly a theoretical haemodynamic question:
Can reduction of afterload lead to intraventricular obstruction if there is a sclerotic aortic valve? Does it not provide a 'fixed obstruction' that overrides reduction of afterload due to vasodilatation?
Was intraventricular gradient mediated more via venodilatation and preload reduction?
What do you think @msiuba @NephroP @ArgaizR @ThinkingCC @drmarcogarrone @khaycock2 ?
What do you think @msiuba @NephroP @ArgaizR @ThinkingCC @drmarcogarrone @khaycock2 ?
Loading suggestions...