

You are a young #medicine resident!
You are working in a heavy emergency when:
23,♂️,p/w acute breathlessness
You check his SpO2, it's👇🏻
You are worried and start him on supplemental 02, but he remains hypoxic😭
Read on for the diagnosis and a brief review!
1/20
#MedTwitter
You are working in a heavy emergency when:
23,♂️,p/w acute breathlessness
You check his SpO2, it's👇🏻
You are worried and start him on supplemental 02, but he remains hypoxic😭
Read on for the diagnosis and a brief review!
1/20
#MedTwitter

Let's start with the causes of hypoxic that don't respond to supplemental oxygen !
🔸R➡️L cardiac shunts
🔸Methemoglobinemia
🔸Sulfmethemoglobinemia
The ABG that you sent is back!!
It shows a normal Pa02 but your pulse oximeter is still reading 85% 🤷♂️
2/20
#MedTwitter
🔸R➡️L cardiac shunts
🔸Methemoglobinemia
🔸Sulfmethemoglobinemia
The ABG that you sent is back!!
It shows a normal Pa02 but your pulse oximeter is still reading 85% 🤷♂️
2/20
#MedTwitter
Your registrar is smart and he asks you to send another sample, this time asking the lab for a methemoglobin value.
Voila !!
The lab says: 45% methemoglobin 😮
3/20
#MedTwitter
Voila !!
The lab says: 45% methemoglobin 😮
3/20
#MedTwitter
Diagnosis established, registrar is a hero 🫡
This is acute methemoglobinemia, most likely acquired, secondary to some drug/toxin 😮
4/20
#MedTwitter
This is acute methemoglobinemia, most likely acquired, secondary to some drug/toxin 😮
4/20
#MedTwitter
Let's list out a few drugs/toxins you need to ask about:
1. Primaquine
2. Dapsone
3. Aniline dyes
4. Nitrites
5. Napthalene
6. Rasburicase
7. Topical anesthetic
The list is endless, any oxidant drug can l/t this !
5/20
#MedTwitter
1. Primaquine
2. Dapsone
3. Aniline dyes
4. Nitrites
5. Napthalene
6. Rasburicase
7. Topical anesthetic
The list is endless, any oxidant drug can l/t this !
5/20
#MedTwitter

Our guy was given some medication for fever by his GP, most likely an antimalarial. Maybe that's the trigger !!
It's important to know because it's to be avoided, FOREVER !!
6/20
#MedTwitter
It's important to know because it's to be avoided, FOREVER !!
6/20
#MedTwitter

You start treating him immediately ✅
1. Continue oxygen
2. Get an IV in place
3. STOP THAT DRUG
4. Send his G6PD levels !!
Wait, G6PD !! WHY❓
7/20
#MedTwitter
1. Continue oxygen
2. Get an IV in place
3. STOP THAT DRUG
4. Send his G6PD levels !!
Wait, G6PD !! WHY❓
7/20
#MedTwitter
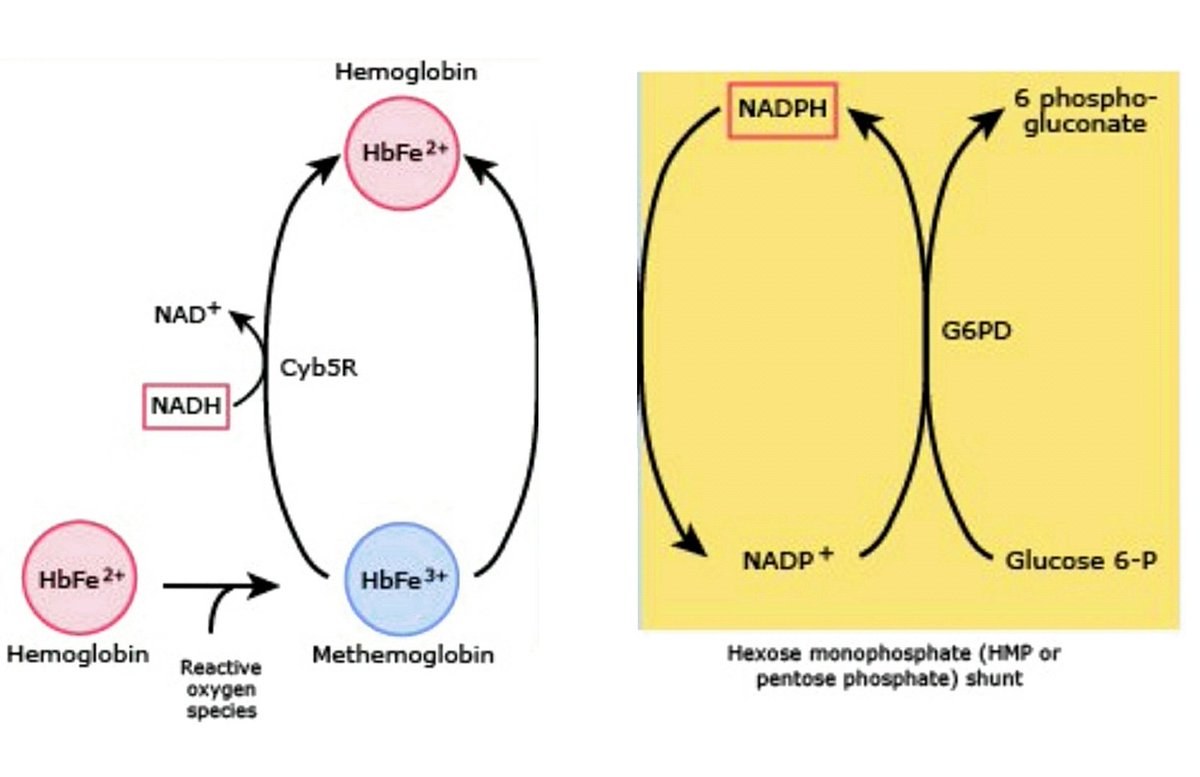
G6PD is important here. To understand this, we need to understand the pathophysiology of metHb'emia
MetHb = Fe++➡️Fe+++
i.e. oxidation=loss of electron
This Fe+++ can't deliver 02 to tissues so hypoxia develops, it's like functional anemia
Treatment Aim: reduce it back to Fe++
MetHb = Fe++➡️Fe+++
i.e. oxidation=loss of electron
This Fe+++ can't deliver 02 to tissues so hypoxia develops, it's like functional anemia
Treatment Aim: reduce it back to Fe++
How does one convert Fe+++➡️Fe++
You add an electron, i.e search for an electron donor !!
In the body, an enzyme called Cytochrome B5 reductase does that.
So if this is ⤵️ then one can develop congenital metHb'emia or be predisposed to it at lesser dose of trigger drug!
9/20
You add an electron, i.e search for an electron donor !!
In the body, an enzyme called Cytochrome B5 reductase does that.
So if this is ⤵️ then one can develop congenital metHb'emia or be predisposed to it at lesser dose of trigger drug!
9/20

Another way of Fe+++➡️Fe++ is to use NADPH from the HMP shunt (uses G6PD)
Normally this is not active in the RBC because RBC has no electron acceptor. This works only if extrinsic electron acceptor like methylene blue is present !!
Phew 😴😴
10/20
Normally this is not active in the RBC because RBC has no electron acceptor. This works only if extrinsic electron acceptor like methylene blue is present !!
Phew 😴😴
10/20
Ok, I'll summarise !!
🔸MetHb is commonly drug induced
🔸Hypoxia despite 02
🔸Normal Pa02 but ⤵️Sp02
🔸Cyanosis ++
🔸Treat:
Stop drug
Give an electron donor to reduce Fe+++
Don't worry, we are 👇🏻
11/20
#MedTwitter
🔸MetHb is commonly drug induced
🔸Hypoxia despite 02
🔸Normal Pa02 but ⤵️Sp02
🔸Cyanosis ++
🔸Treat:
Stop drug
Give an electron donor to reduce Fe+++
Don't worry, we are 👇🏻
11/20
#MedTwitter
Coming back to the patient !
You recieve his G6PD levels and they are within normal limits 🙏🏻
You decide to administer methylene blue 🔵🔵🔵
Dose: 1mg/kg IV
Repeat dose after 1 hr if symptoms persist.
12/20
#MedTwitter
You recieve his G6PD levels and they are within normal limits 🙏🏻
You decide to administer methylene blue 🔵🔵🔵
Dose: 1mg/kg IV
Repeat dose after 1 hr if symptoms persist.
12/20
#MedTwitter
You can't use the ABG now to monitor his methemoglobin levels !!
The methylene blue will cause a false + reading. Can't get into details here, DM for more if interested !
So next dose only if clinically indicated, i.e. dyspnoea still present or worse.
13/20
#MedTwitter
The methylene blue will cause a false + reading. Can't get into details here, DM for more if interested !
So next dose only if clinically indicated, i.e. dyspnoea still present or worse.
13/20
#MedTwitter
What if his G6PD was ⤵️ ?
1. The methylene blue wouldn't work
2. The methylene blue could possibly harm him too!
Methylene blue is an oxidant itself and in G6PD deficiency it can paradoxically cause methemoglobinemia🤷♂️
We use high dose Vit C here, upto 10gm
14/20
#MedTwitter
1. The methylene blue wouldn't work
2. The methylene blue could possibly harm him too!
Methylene blue is an oxidant itself and in G6PD deficiency it can paradoxically cause methemoglobinemia🤷♂️
We use high dose Vit C here, upto 10gm
14/20
#MedTwitter
Also don't use methylene blue if a patient is on an SSRI.
There's a risk of serotonin syndrome !!
15/20
#MedTwitter
There's a risk of serotonin syndrome !!
15/20
#MedTwitter

This patient recieved Methylene blue x 1 dose and recovered well 👍🏻
But did he have some predisposition to develop it in the first place ??
Maybe some enzyme deficiency, like cytochrome B5 reductase as we spoke about earlier !
16/20
#MedTwitter
But did he have some predisposition to develop it in the first place ??
Maybe some enzyme deficiency, like cytochrome B5 reductase as we spoke about earlier !
16/20
#MedTwitter
Maybe !!
Heterozygous state for cytochrome b5 reductase can predispose to developing metHb with minimal exposure d/t borderline enzyme activity.
Any little exposure might push them over the edge 👇🏻
17/20
#MedTwitter
Heterozygous state for cytochrome b5 reductase can predispose to developing metHb with minimal exposure d/t borderline enzyme activity.
Any little exposure might push them over the edge 👇🏻
17/20
#MedTwitter

Homozygous state presents in childhood itself w/
1. Chronic cyanosis
2. Minimal hypoxia due to a compensatory ⤴️RBC (erythrocytosis)
The acute management won't change so it's not so important to determine this at present. Can order an enzyme activity/NGS after recovery !
18/20
1. Chronic cyanosis
2. Minimal hypoxia due to a compensatory ⤴️RBC (erythrocytosis)
The acute management won't change so it's not so important to determine this at present. Can order an enzyme activity/NGS after recovery !
18/20
Summary slide, yeah finally 🤣
🔸When to suspect:
•Hypoxia despite 02
•Unexplained cyanosis
🔸Easy to dx on an ABG
🔸Inherited or acquired
🔸Detailed drug history
🔸Treat if metHb ≥10%
🔸Send G6PD
🔸Start Vitamin C
🔸Give methylene blue if normal G6PD
19/20
🔸When to suspect:
•Hypoxia despite 02
•Unexplained cyanosis
🔸Easy to dx on an ABG
🔸Inherited or acquired
🔸Detailed drug history
🔸Treat if metHb ≥10%
🔸Send G6PD
🔸Start Vitamin C
🔸Give methylene blue if normal G6PD
19/20
If you've read this far, you are awesome 💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼💪🏼
Thank you 🙏🏻
#MedTwitter if you like it, share it ✅
20/20
#MedEd
Thank you 🙏🏻
#MedTwitter if you like it, share it ✅
20/20
#MedEd

Loading suggestions...