

1) Welcome to our #IM_tweetorial, follow us for unlimited educational series in the field of internal medicine by @sscpInMedpsn, @SSCP_KSA
2) In this #IM_tweetorial series, we will be highlighting key updates summary on the recently published "Standards of Care in Diabetes-2023" by American Diabetes Association (#ADA)
It's updated and published annually, or more often online if there was new evidence or any changes
It's updated and published annually, or more often online if there was new evidence or any changes

3) Sections to key updates summary:
🔍Diagnosis
Point-of-care #A1C testing for screening and diagnosis should be restricted to U.S FDA– approved devices at laboratories proficient in performing testing of moderate complexity or higher by trained personnel.
🔍Diagnosis
Point-of-care #A1C testing for screening and diagnosis should be restricted to U.S FDA– approved devices at laboratories proficient in performing testing of moderate complexity or higher by trained personnel.
- More intensive preventive should be considered for whom are at high risk of progression to #DM:
• BMI ≥ 35 kg/m2
• Higher glucose levels (e.g., FBG 110–125 mg/dL, 2-h post-challenge glucose 173– 199 mg/dL, A1C ≥ 6.0%)
• History of gestational diabetes mellitus
• BMI ≥ 35 kg/m2
• Higher glucose levels (e.g., FBG 110–125 mg/dL, 2-h post-challenge glucose 173– 199 mg/dL, A1C ≥ 6.0%)
• History of gestational diabetes mellitus
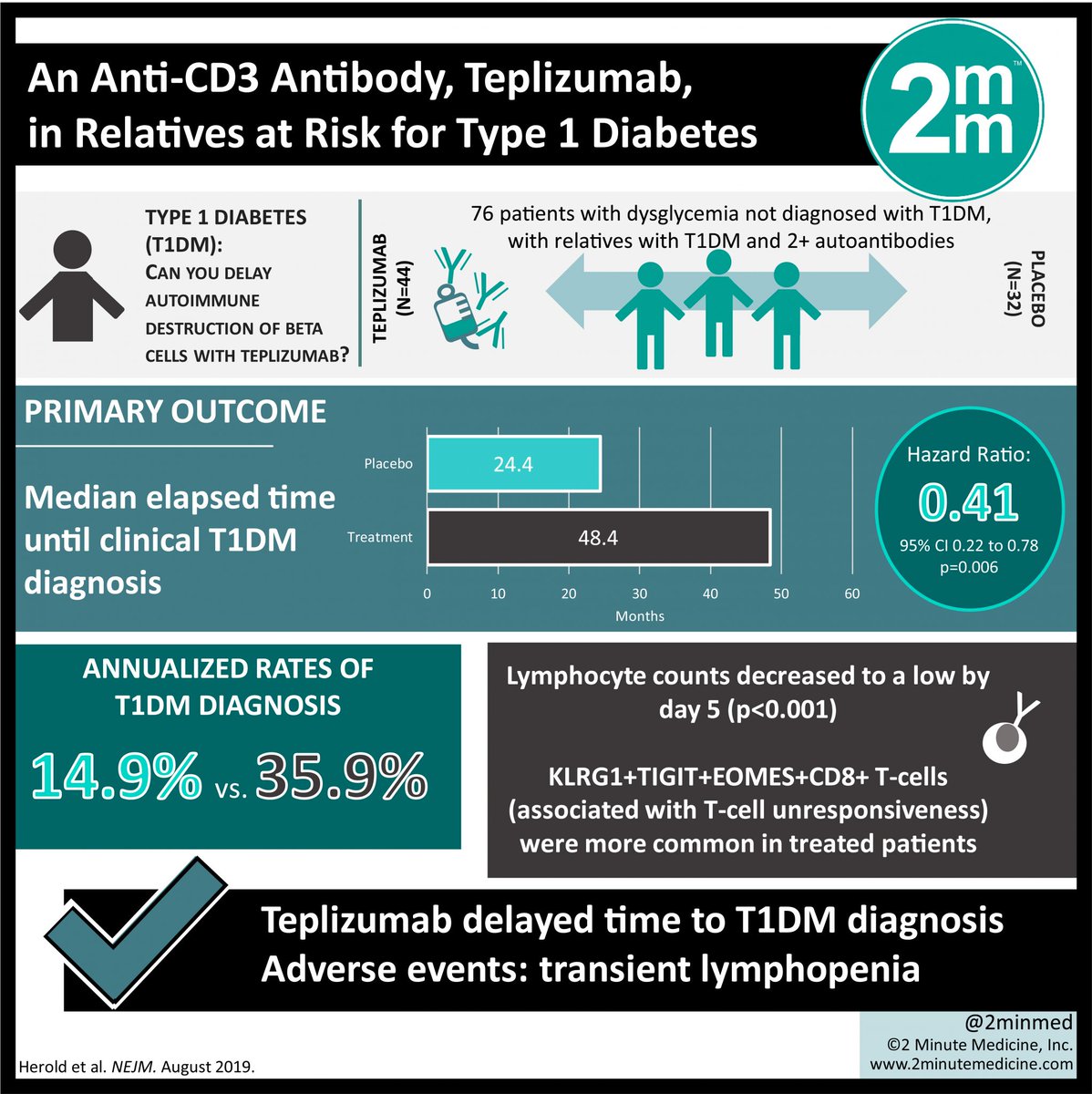
- The guide has also addressed the new medication #Teplizumab, a newly anti-CD3 FDA approved for stage 2 #T1D to delay progression to stage 3 #T1D. It's not currently available for clinical use.
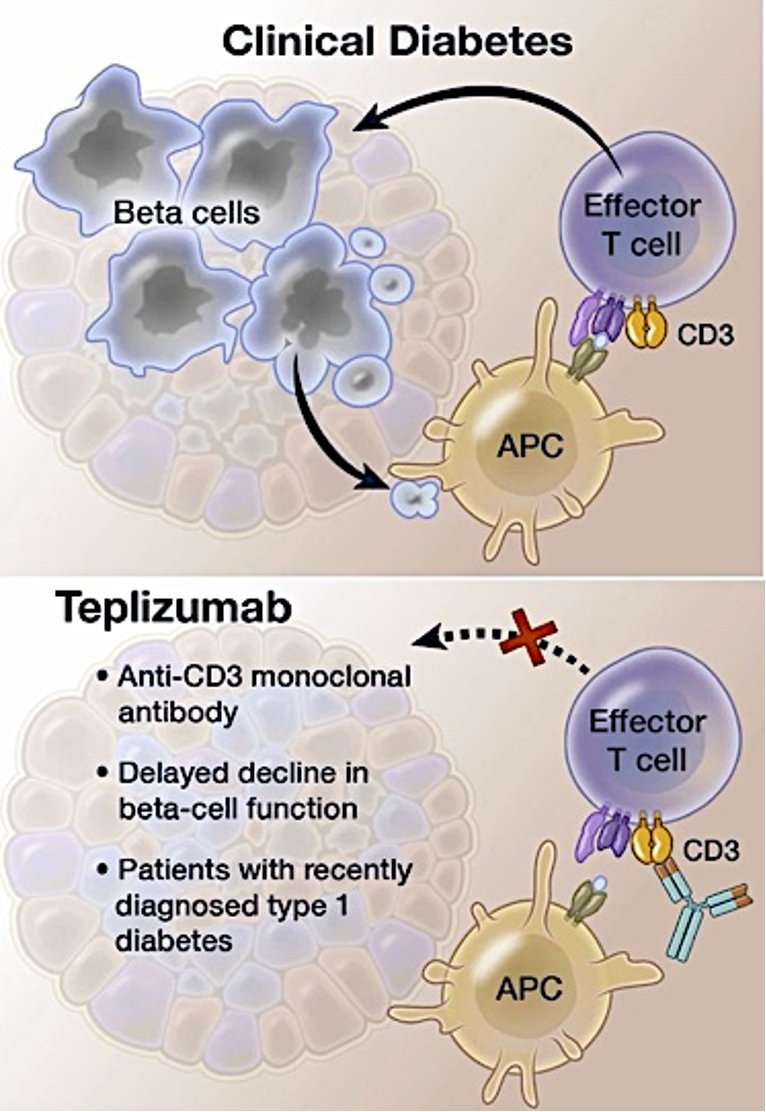
- "An anti-CD3 Antibody, Teplizumab, in relatives at risk for Type 1 Diabetes"- a phase 2, randomized, placebo-controlled, double-blind trial which included 76 participants with relatives with #T1D and were assigned to a single 14-day IV course of teplizumab or placebo.
5) 🧩 Comorbidities:
- A complete medical evaluation should be performed at the initial visit.
- A complete medical evaluation should be performed at the initial visit.

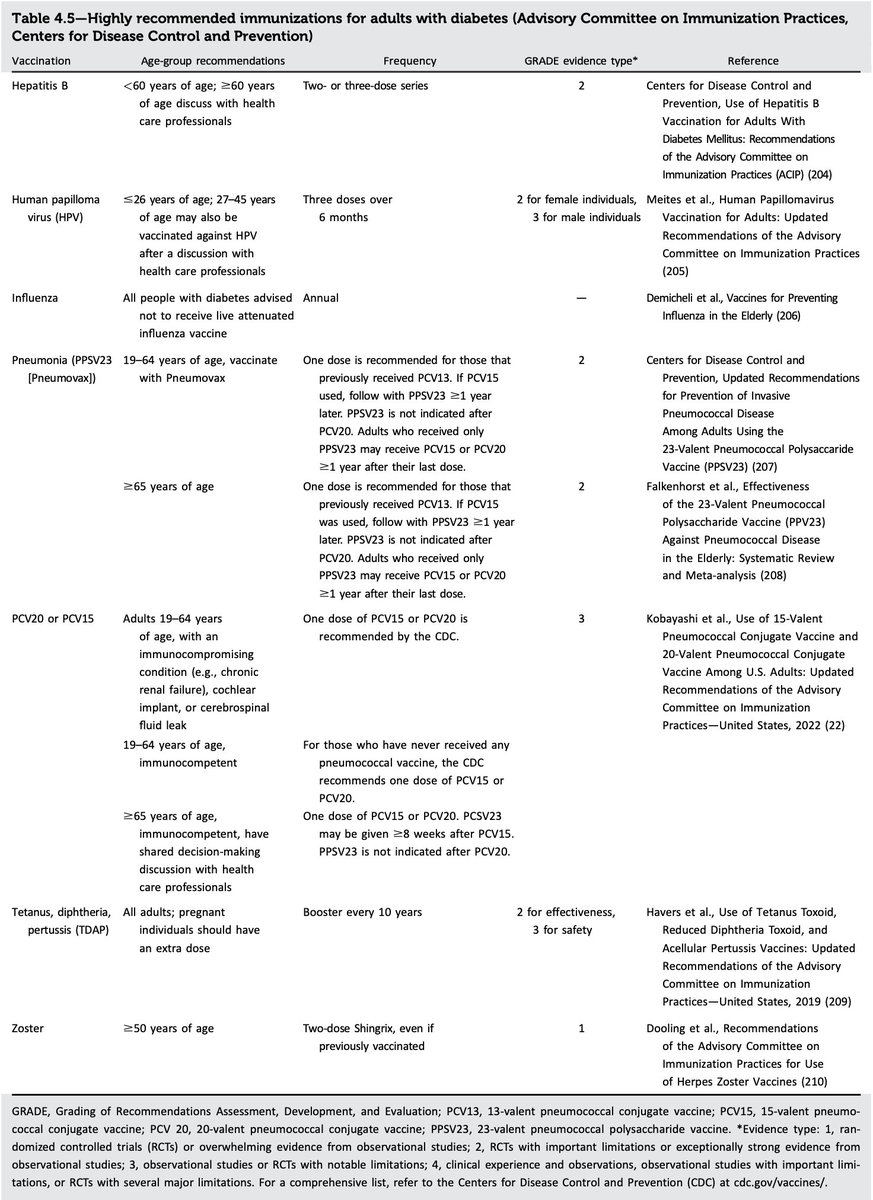
- Considerable changes were made in the #immunizations subsection to reflect new indications and guidance, particularly for #COVID-19 and pneumococcal pneumonia vaccinations.
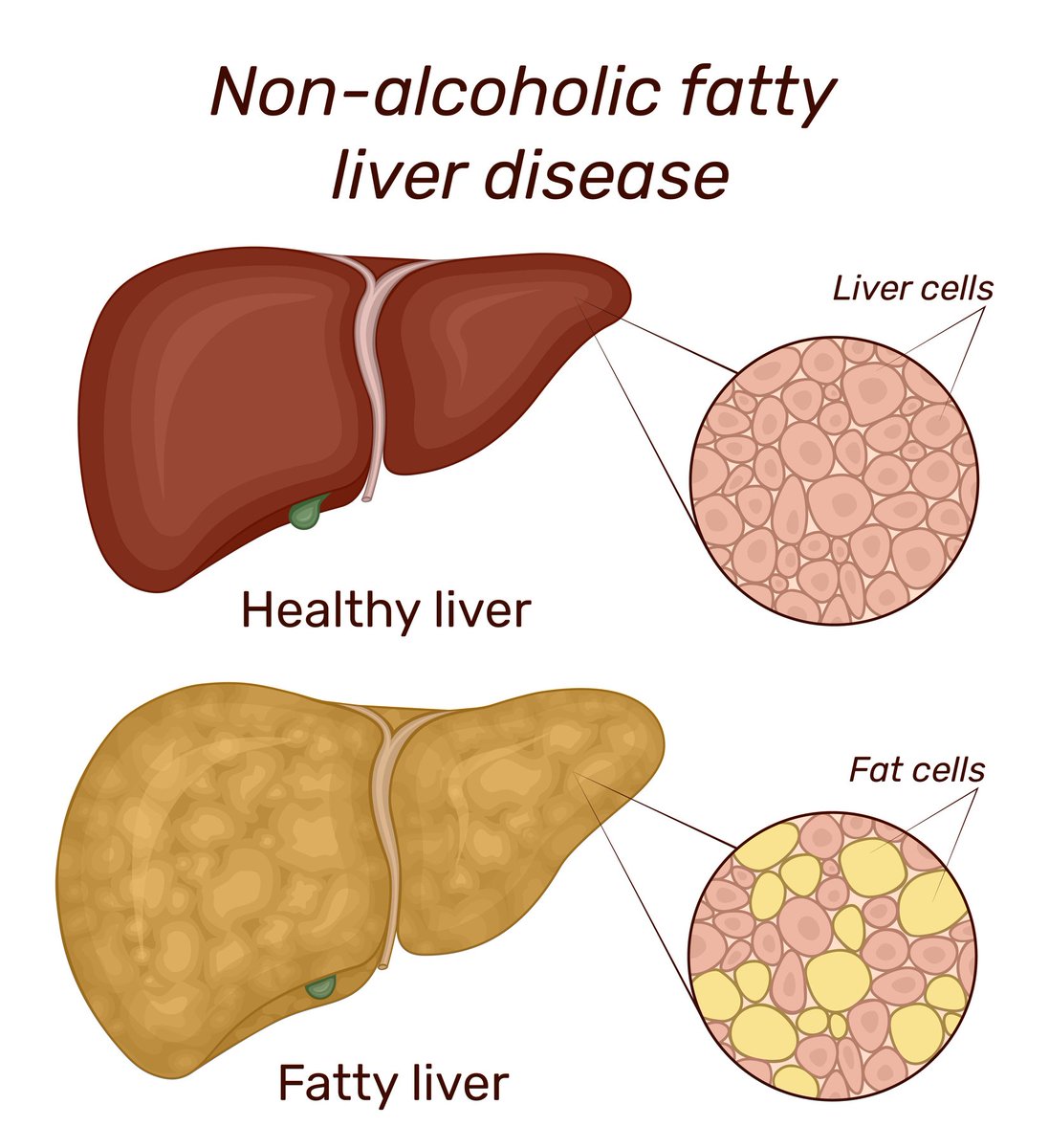
- In #T2D or #prediabetes with cardio-metabolic risk factor, who have either elevated ALT or fatty liver on imaging, should be evaluated for nonalcoholic steatohepatitis and liver fibrosis.
- A minimum weight loss goal of 5%, preferably ≥10% is needed to improve liver histology
- A minimum weight loss goal of 5%, preferably ≥10% is needed to improve liver histology
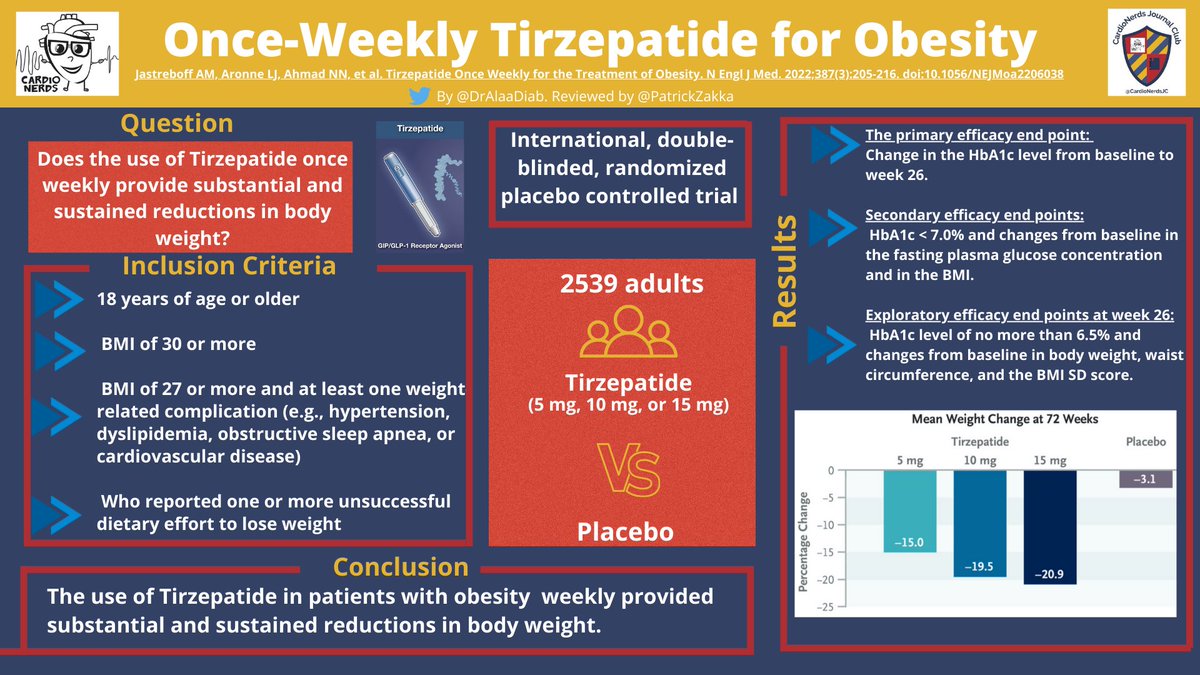
- More emphasis on large weight loss goals (up to 15%) with the new efficacious drugs
- Dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) receptor agonist (#Tirzepatide) was added as a glucose-lowering option with the potential for weight loss nejm.org
- Dual GLP-1/glucose-dependent insulinotropic polypeptide (GIP) receptor agonist (#Tirzepatide) was added as a glucose-lowering option with the potential for weight loss nejm.org
❓Which of these BMIs where a pharmacological therapy is indicated?
✅ D, that’s correct. 👏🏻 Pharmacological therapy is indicated as an adjunct to nutrition, physical activity, and behavioral counseling for selected people with type 2 diabetes and BMI ≥27 kg/m
8) 🫀CV
- Updated #HTN definition as SBP ≥130 mmHg or DBP ≥80 mmHg based on an average of >2 measurements obtained on >2 occasions.
- If BP ≥180/110 mmHg + CV disease could be diagnosed with HTN at a single visit.
- Target BP goal is <130/80 mmHg if can safely be attained.
- Updated #HTN definition as SBP ≥130 mmHg or DBP ≥80 mmHg based on an average of >2 measurements obtained on >2 occasions.
- If BP ≥180/110 mmHg + CV disease could be diagnosed with HTN at a single visit.
- Target BP goal is <130/80 mmHg if can safely be attained.
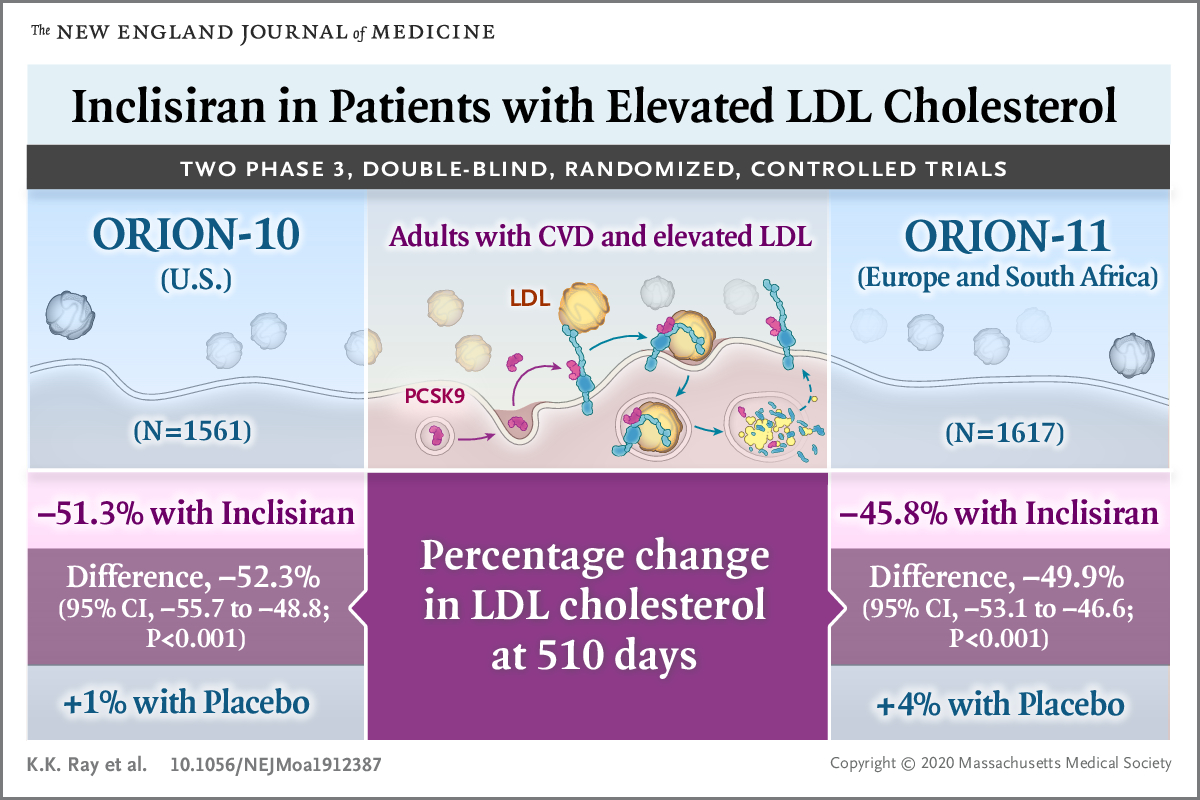
- A paragraph was added to include #Inclisiran, an siRNA directed against #PCSK9, a new FDA- approved cholesterol-lowering therapy.
nejm.org
- A CV outcome trial using Inclisiran in people with established #CV disease is currently ongoing.
nejm.org
- A CV outcome trial using Inclisiran in people with established #CV disease is currently ongoing.
9)🫘CKD
- New levels for starting #SGLT2i at GFR ≥20 & urinary albumin ≥200 mg/g creatinine
- #SGLT2i might be effective in urinary albumin normal to 200 mg/g creatinine
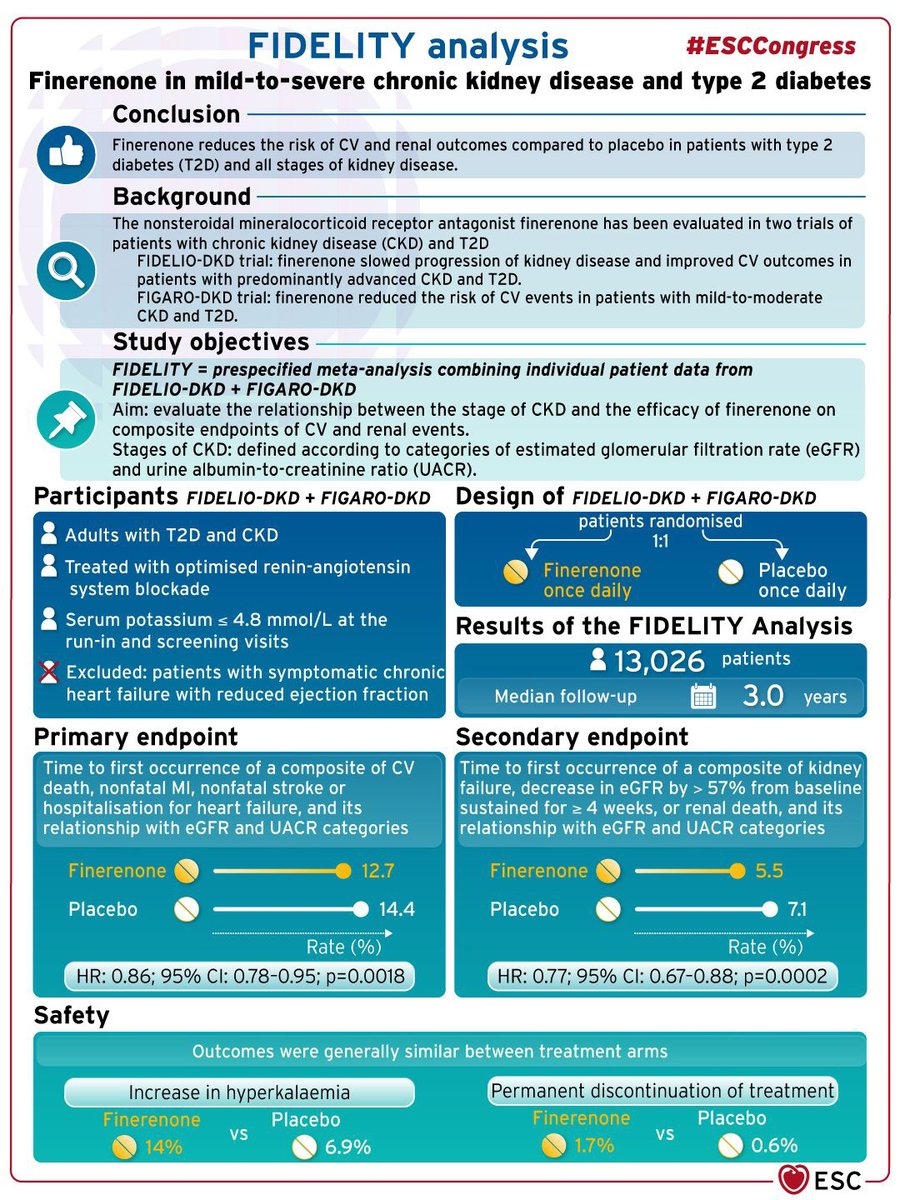
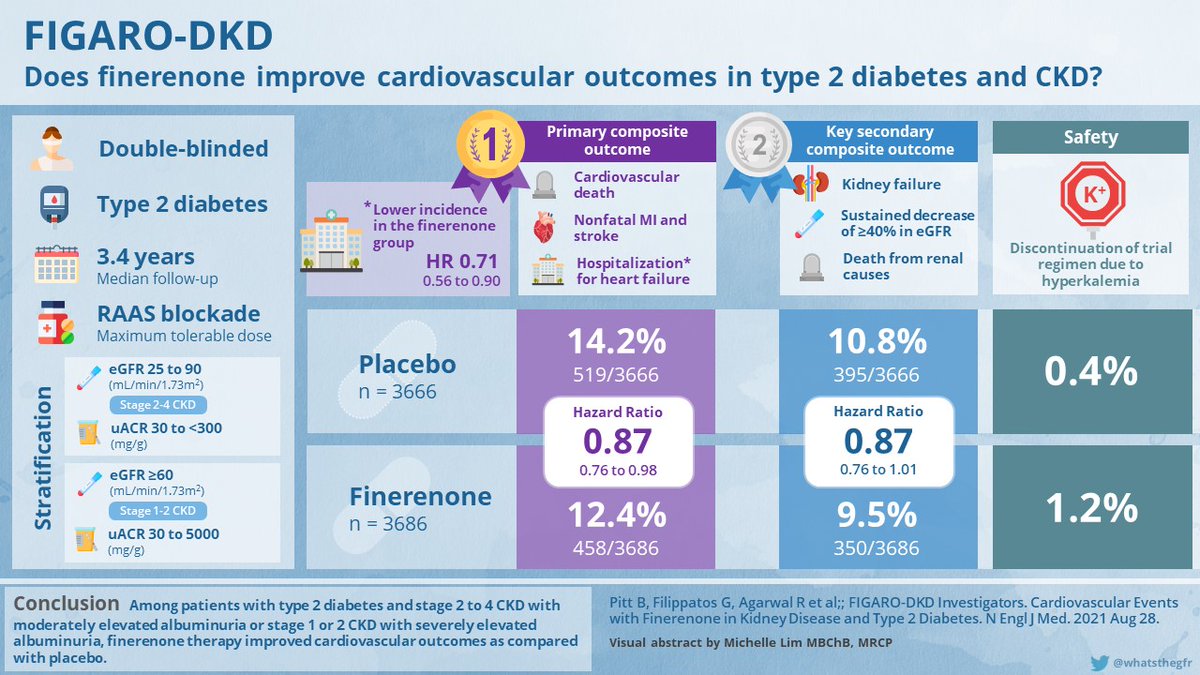
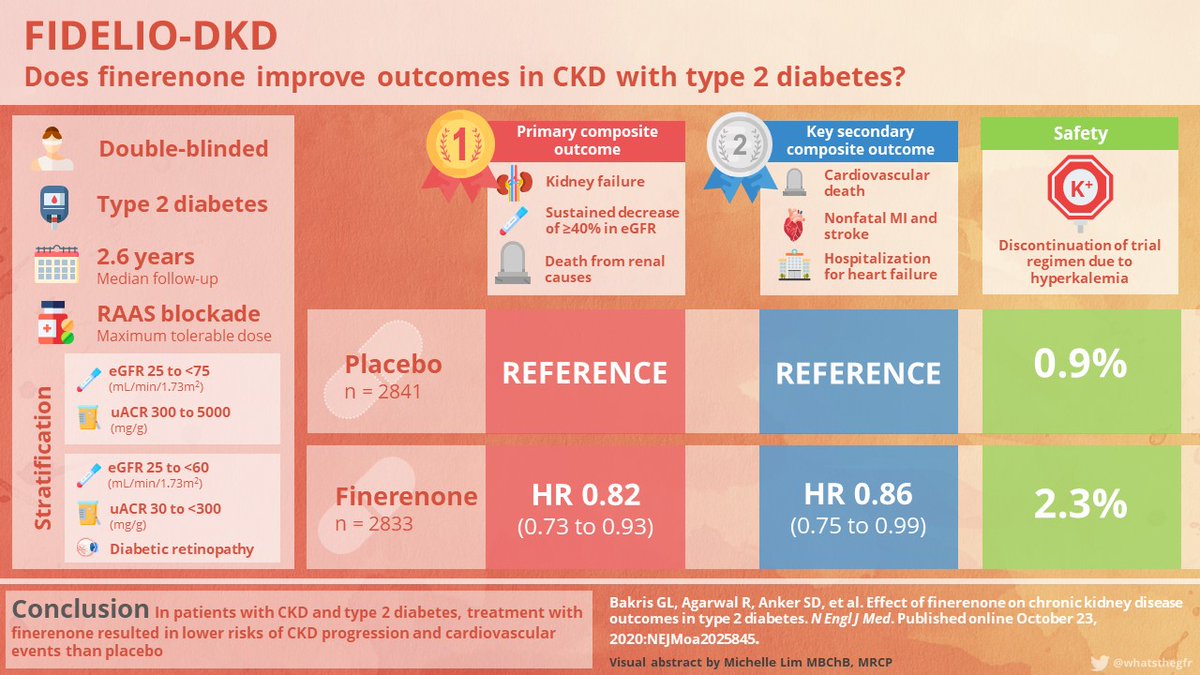
- #T2D+#CKD+#albuminuria on max. tolerated ACE/ARB,adding #Finerenone is recommended for CV & CKD protection
- New levels for starting #SGLT2i at GFR ≥20 & urinary albumin ≥200 mg/g creatinine
- #SGLT2i might be effective in urinary albumin normal to 200 mg/g creatinine
- #T2D+#CKD+#albuminuria on max. tolerated ACE/ARB,adding #Finerenone is recommended for CV & CKD protection
❓In a patient with T2D + diabetic kidney disease, agents with CV risk reduction are?
✅ D, that’s correct👏🏻, SGLT2i in GFR ≥20 mL/min/1.73 m2, GLP1, or Finerenone in GFR ≥25 mL/min/1.73 m2 are indicated to reduce CV risk in T2D with diabetic kidney disease.
10)🦶🏻Neuropathy
- Screen diabetic peripheral #neuropathy at diagnosis of #T2D & 5y after diagnosis of #T1D & annually thereafter.
- Screening includes checking: orthostatic dizziness, syncope, dry cracked skin in the extremities.
- Screen diabetic peripheral #neuropathy at diagnosis of #T2D & 5y after diagnosis of #T1D & annually thereafter.
- Screening includes checking: orthostatic dizziness, syncope, dry cracked skin in the extremities.
- Signs of autonomic neuropathy include orthostatic hypotension, resting tachycardia, or evidence of peripheral dryness or cracking of the skin.
- Gabapentinoids, SNRIs, TCAs, and sodium channel blockers are recommended as initial therapy for neuropathic pain in diabetes.
- Gabapentinoids, SNRIs, TCAs, and sodium channel blockers are recommended as initial therapy for neuropathic pain in diabetes.
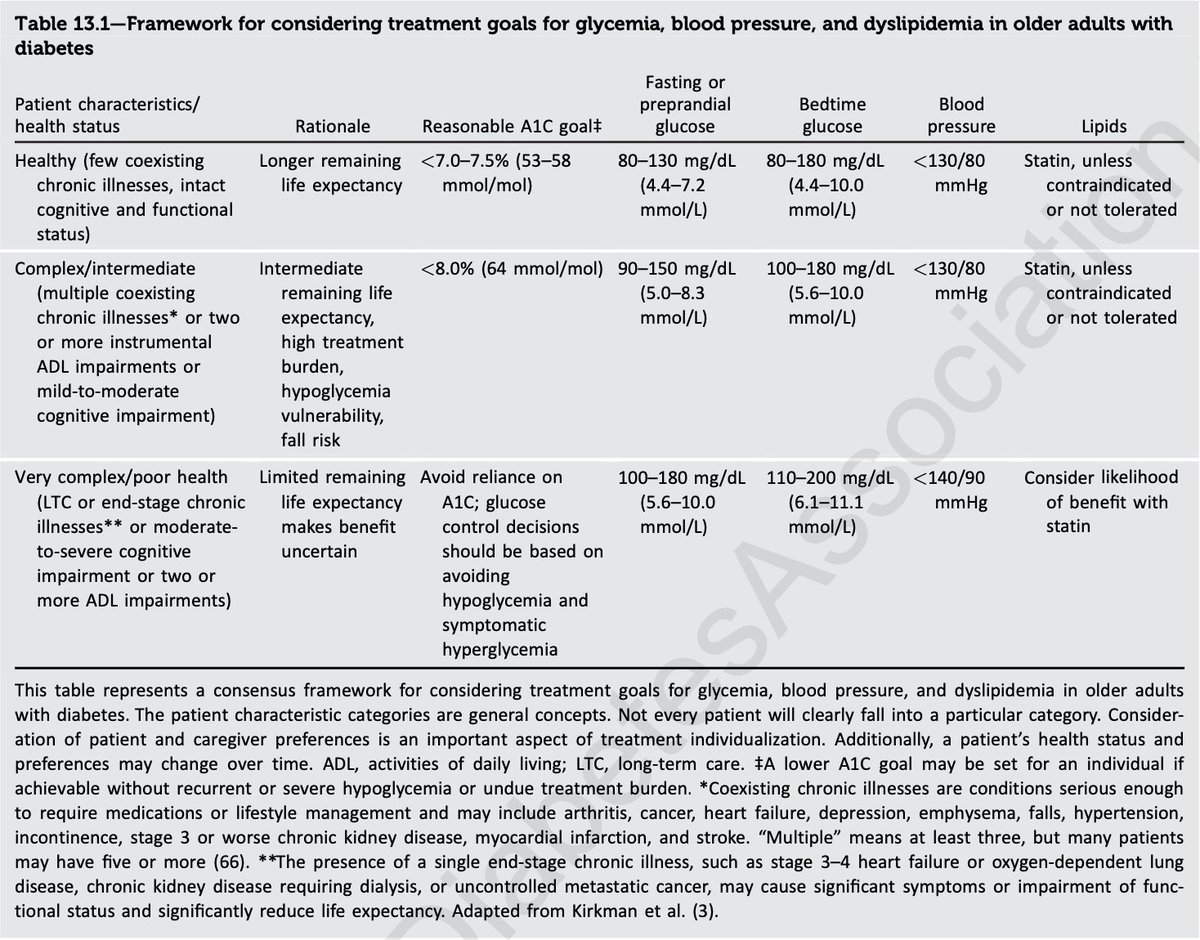
- Blood pressure targets were lowered to align with evidence from multiple recent trials.
- Recommendation on De-intensification of treatment goals to reduce the risk of hypoglycemia & Simplification of complex treatment plans to reduce the risk of hypoglycemia and poly-pharmacy.
- Recommendation on De-intensification of treatment goals to reduce the risk of hypoglycemia & Simplification of complex treatment plans to reduce the risk of hypoglycemia and poly-pharmacy.
12) 🏥Diabetes Care in the Hospital
- Need for target individualization with inpatients of hyperglycemia in noncritical care
- Expert consensus recommend a target 100–180 mg/dL (5.6–10.0 mmol/L) for noncritically with “new” hyperglycemia as well with known DM prior to admission
- Need for target individualization with inpatients of hyperglycemia in noncritical care
- Expert consensus recommend a target 100–180 mg/dL (5.6–10.0 mmol/L) for noncritically with “new” hyperglycemia as well with known DM prior to admission
- An insulin regimen with basal, prandial, and correction components is the preferred treatment for most noncritically ill hospitalized patients with adequate nutritional intake.
13) 🤩Finally, for more details you can check
Full ADA guideline version available at diabetesjournals.org
Free app with interactive tools at:
📱Apple: apps.apple.com
📱Google Play: play.google.com
Full ADA guideline version available at diabetesjournals.org
Free app with interactive tools at:
📱Apple: apps.apple.com
📱Google Play: play.google.com
Loading suggestions...