

Tweetorial coming up.. 🧵 #AskRenal #NSMC #MedTwitter #NephTwitter
Why does hypophosphatemia (serum phosphorus ˂2.5 mg/dL) happen in patients with cancer?
Why does hypophosphatemia (serum phosphorus ˂2.5 mg/dL) happen in patients with cancer?
The answer is all of the above. There are multiple reasons as to why serum phosphate levels drop in patients with cancer.
But before we dive into them, let’s talk about some basic physiology.
But before we dive into them, let’s talk about some basic physiology.

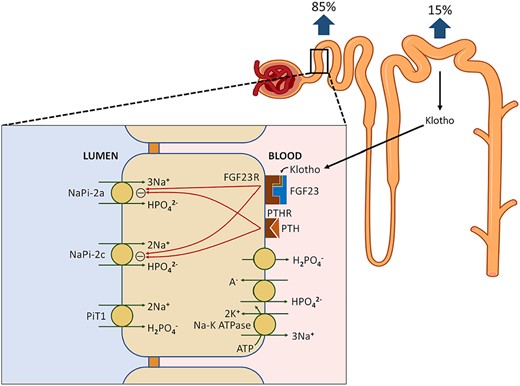
Around 85% of phosphate is reabsorbed in the proximal tubule through secondary active transport.
5–20% of filtered phosphate (13 mg/kg/day) is eventually excreted in the urine.
⁉️What transporters reabsorb phosphate?
5–20% of filtered phosphate (13 mg/kg/day) is eventually excreted in the urine.
⁉️What transporters reabsorb phosphate?
Reabsorption of phosphate happens at the level of the NaPis.
High serum phosphorus levels cause internalization of the transporters and an increase in phosphate excretion.
PTH and phosphatonins (FGF-23 and klotho) cause downregulation of NaPis leading to phosphate excretion.
High serum phosphorus levels cause internalization of the transporters and an increase in phosphate excretion.
PTH and phosphatonins (FGF-23 and klotho) cause downregulation of NaPis leading to phosphate excretion.
Pseudohypophosphatemia is when we have low serum phosphorus that does not reflect the actual systemic levels- kind of an illusion.
It should be considered in patients with multiple myeloma (MM), paraproteinemias & leukemia due to interference with the phosphate assay.
It should be considered in patients with multiple myeloma (MM), paraproteinemias & leukemia due to interference with the phosphate assay.
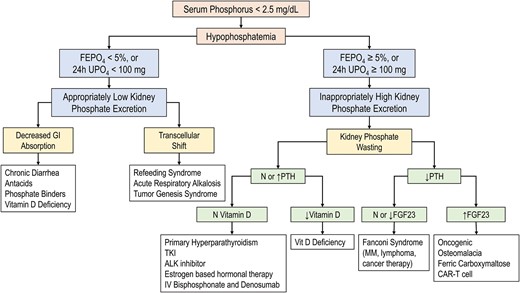
When pseudohypophosphatemia is excluded, we think about hypophosphatemia in 3 etiologies:
🔹Decreased PO intake
🔹Losses (renal and GI)
🔹Decreased intestinal absorption.
🔹Decreased PO intake
🔹Losses (renal and GI)
🔹Decreased intestinal absorption.
We can follow the below algorithm from @CKJsocial that simplifies etiologies of hypophosphatemia.
🔹Decreased intake:
Patients with cancer frequently suffer from significant malnutrition marked by nausea, weight loss, and loss of muscle mass
Patients with cancer frequently suffer from significant malnutrition marked by nausea, weight loss, and loss of muscle mass
🔹Decreased intestinal absorption:
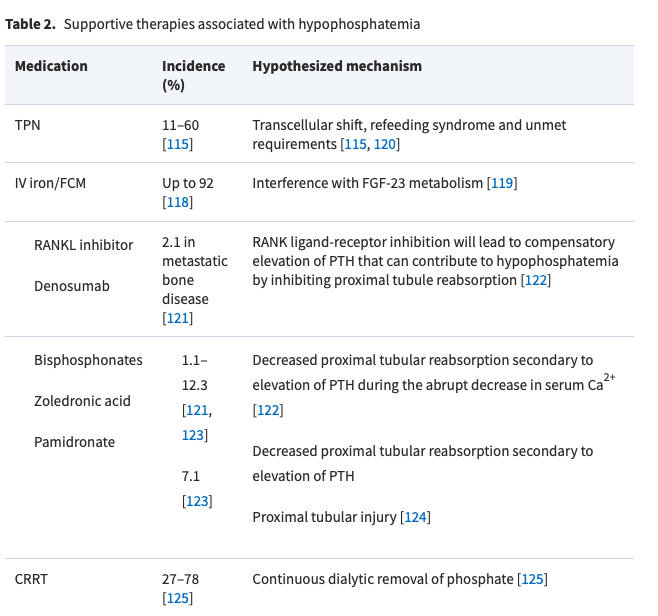
Cancer therapy and supportive therapies may contribute to poor intestinal absorption and increased GI losses (diarrhea).
Some etiologies of supportive therapies and hypophosphatemia are listed below:
Cancer therapy and supportive therapies may contribute to poor intestinal absorption and increased GI losses (diarrhea).
Some etiologies of supportive therapies and hypophosphatemia are listed below:
🔹Transcellular shifts:
Refeeding syndrome is a potentially fatal metabolic disturbance due to reinstitution of nutrition in patients with poor nutrition
Tumor genesis syndrome is hypophosphatemia caused by a shift of extracellular phosphorus into the rapidly replicating cells
Refeeding syndrome is a potentially fatal metabolic disturbance due to reinstitution of nutrition in patients with poor nutrition
Tumor genesis syndrome is hypophosphatemia caused by a shift of extracellular phosphorus into the rapidly replicating cells

Renal losses:
certain hematological malignancies (lymphoma and monoclonal gammopathy) and cancer therapies have been associated with acquired PCT dysfunction => Fanconi sd => generalized impairment in reabsorption of solutes including phosphate
certain hematological malignancies (lymphoma and monoclonal gammopathy) and cancer therapies have been associated with acquired PCT dysfunction => Fanconi sd => generalized impairment in reabsorption of solutes including phosphate

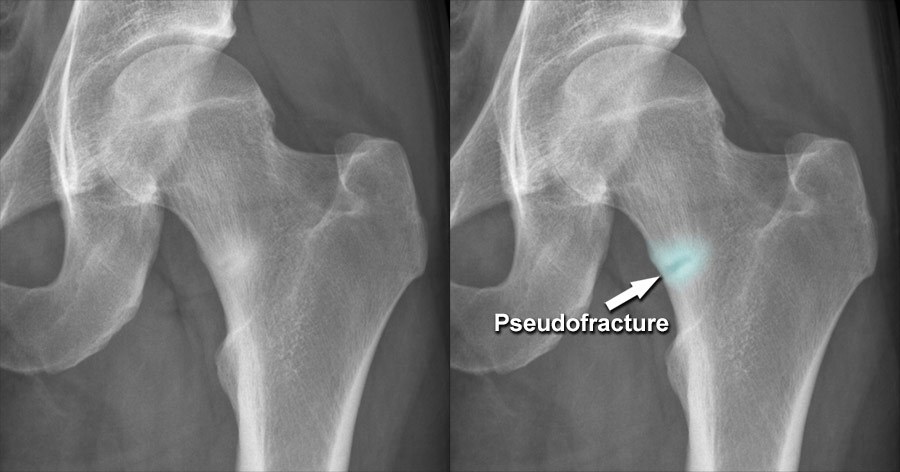
Oncogenic osteomalacia:
tumors secrete FGF-23 and cause hypophosphatemia through renal phosphate wasting. Chronic hypophosphatemia leads to osteomalacia that appears as osteopenia and pseudofractures on radiographs.
Image from: radiologymasterclass.co.uk
tumors secrete FGF-23 and cause hypophosphatemia through renal phosphate wasting. Chronic hypophosphatemia leads to osteomalacia that appears as osteopenia and pseudofractures on radiographs.
Image from: radiologymasterclass.co.uk
Loading suggestions...